Page 21 of 46
PH8.7 | PH8.7 | Protozoal and Vector-Borne Disease Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Discuss the types, kinetics, and adverse effects of drugs used for amoebiasis, kala-azar, malaria, and filariasis
- Select appropriate drugs for each disease category based on clinical presentation and pathogen species
- Identify key safety issues: G6PD screening before primaquine; teratogenicity of miltefosine; management of P. falciparum vs P. vivax malaria
INSTRUCTIONS
India is endemic for all four disease categories in PH8.7. Malaria kills approximately 80,000 people annually in India; kala-azar remains endemic in Bihar, Jharkhand, Uttar Pradesh, and West Bengal; amoebiasis causes an estimated 100,000 deaths globally per year; lymphatic filariasis affects 21 million Indians. Understanding the pharmacotherapy for these diseases requires matching the drug to the specific biological niche of the pathogen — tissue vs luminal in amoebiasis; blood stage vs hypnozoite in malaria; the macrophage in leishmaniasis.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 63–65 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 62–63 (textbook)
- National Vector Borne Disease Control Programme (NVBDCP) India — Malaria Treatment Guidelines 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 25-year-old migrant labourer from Bihar returns to his home village after 3 months of work in Assam. He develops fever with chills and rigors, confirms malaria with RDT positive for P. vivax, and is treated with chloroquine by the local health worker. He recovers within 5 days. Three months later, he develops the same fever again. His blood film shows P. vivax. This is not treatment failure from chloroquine resistance — it is a RELAPSE from hypnozoites (dormant liver-stage parasites) that chloroquine cannot reach. The correct treatment includes primaquine for radical cure — but primaquine can cause fatal haemolysis in G6PD-deficient patients. How do you test safely, and what do you do if he is G6PD deficient? This scenario illustrates why a single drug is insufficient for P. vivax malaria, and why pharmacological understanding of the parasite life cycle is clinically essential.
WHY THIS MATTERS
Protozoal and vector-borne diseases disproportionately burden India's rural and tribal populations — the very patients you will care for in rural postings, district hospitals, and community health centres. Malaria remains the leading cause of fever in many endemic districts. Kala-azar is a neglected tropical disease that is 100% fatal if untreated and has a specific epidemiological geography (Bihar belt). Amoebiasis is ubiquitous wherever sanitation is poor. Filariasis causes chronic disability (lymphoedema, hydrocele) affecting productivity and quality of life. The drugs you learn in this SDL are genuinely life-saving in the Indian context.
RECALL
From the antibacterials SDL: metronidazole — nitroimidazole prodrug, activated by ferredoxin oxidoreductase in anaerobes/protozoa to reactive radical species → DNA strand breaks; bactericidal for strict anaerobes; active vs Giardia, Trichomonas, E. histolytica; avoid alcohol (disulfiram-like). Amphotericin B — binds ergosterol in fungal/protozoal membranes, forming pores → ion leak → cell death; nephrotoxic (conventional formulation); liposomal formulation reduces nephrotoxicity by targeting reticuloendothelial system macrophages. From microbiology: Plasmodium lifecycle — mosquito → liver stage (sporozoites → hepatic schizonts → merozoites into blood) → blood stage (erythrocytic cycle → fever at rupture) → gametocytes; P. vivax and P. ovale form hypnozoites (dormant hepatocytes); P. falciparum does not.
Protozoal and Vector-Borne Disease Burden in India
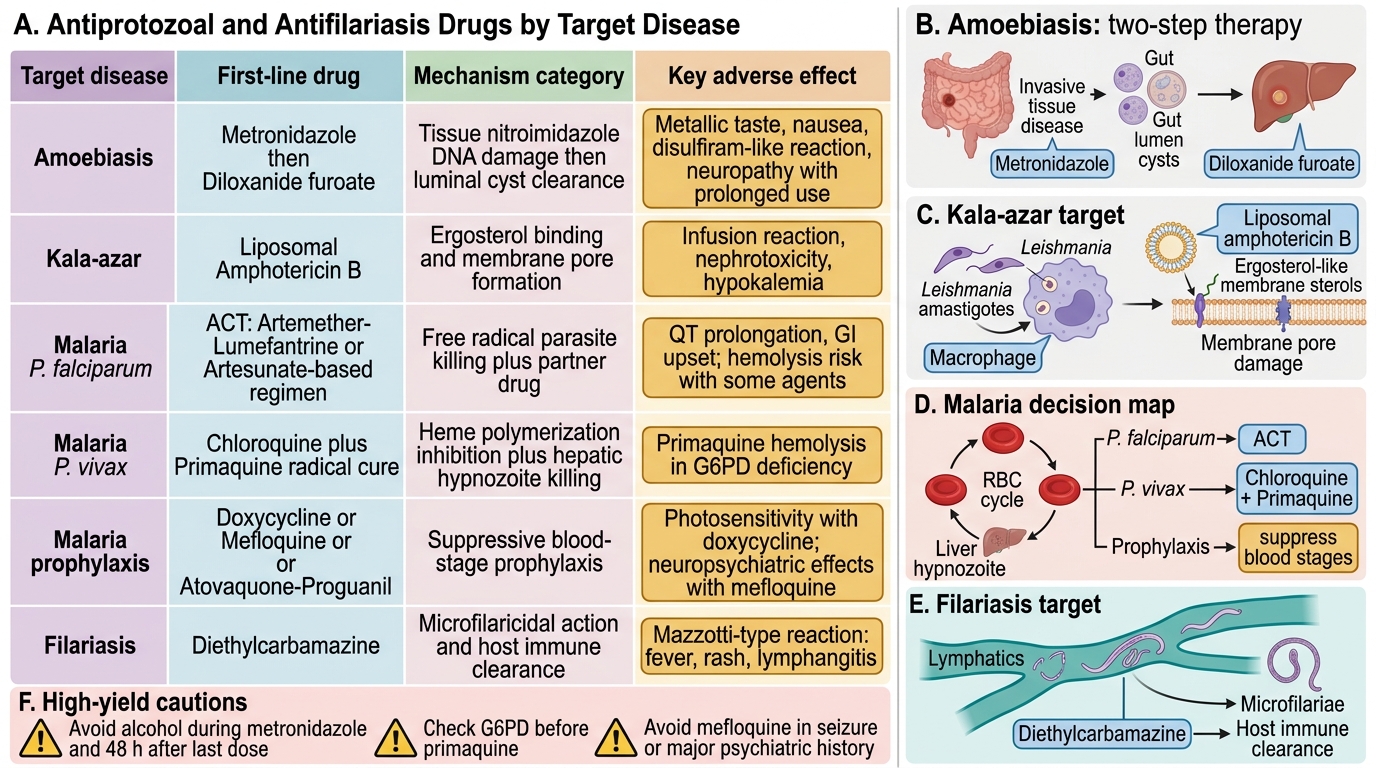
The pharmacological management of protozoal and vector-borne diseases is inseparable from their pathobiology — each parasite exploits a specific biological niche that defines where and how drugs must act. Understanding the disease-specific pathophysiology prevents the common error of prescribing a drug that reaches the wrong compartment.
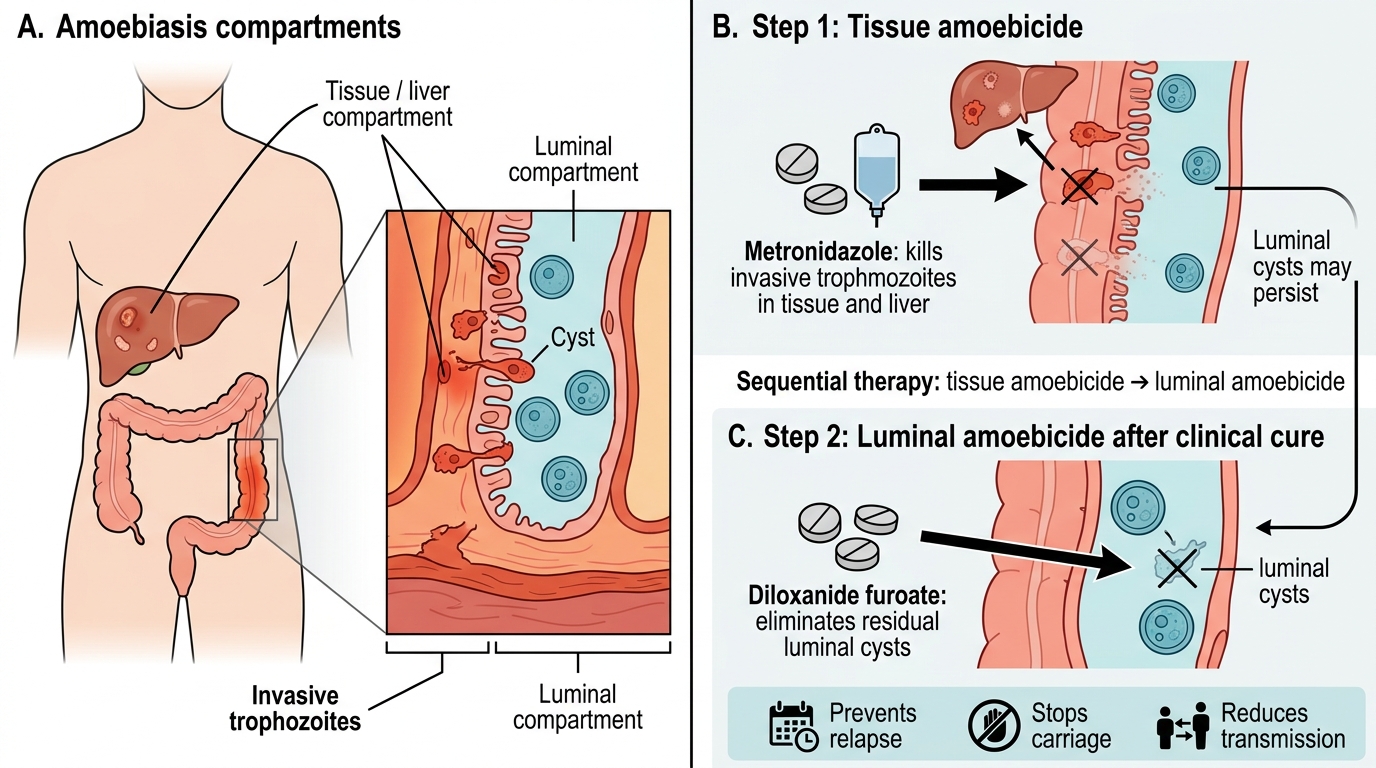
Amoebiasis (Entamoeba histolytica): E. histolytica exists in two forms: trophozoites (invasive, motile, cause disease — invade colonic epithelium and liver via portal blood) and cysts (non-invasive, transmitted in contaminated water/food, survive in environment). Pathophysiology: trophozoites secrete proteases and lectins that lyse host epithelial cells → flask-shaped ulcers in the colon → dysentery. Portal spread → liver abscess (right lobe predominantly, single in 85%). This dual compartment pathology — invasive trophozoites in tissue AND luminal cysts perpetuating transmission — mandates two drug types: a tissue amoebicide (metronidazole) to kill invasive forms and a luminal amoebicide (diloxanide furoate) to eliminate cysts.
Kala-azar / Visceral Leishmaniasis (Leishmania donovani): Transmitted by Phlebotomus sandfly bite → promastigotes deposited in skin → phagocytosed by macrophages → transform into amastigotes → multiply within phagolysosomes of macrophages in the liver, spleen, and bone marrow → hepatosplenomegaly, pancytopenia, cachexia. L. donovani cleverly inhibits phagolysosomal killing mechanisms within the macrophage. Drugs must reach the intramacrophage compartment — explaining why liposomal amphotericin B (which is preferentially phagocytosed by macrophages) is so effective.
Malaria (Plasmodium spp.): Anopheles mosquito injects sporozoites → liver (hepatic schizogony, 7–10 days, asymptomatic) → merozoites released into blood → invade erythrocytes → erythrocytic schizogony (48h for P. vivax/ovale/falciparum; 72h for P. malariae) → clinical fever at synchronous rupture. P. vivax/ovale form hypnozoites — dormant hepatic forms that can activate months-years later to cause relapse. P. falciparum uniquely causes cytoadherence (infected RBCs adhere to capillary endothelium) — explaining cerebral malaria, placental sequestration, and the severity of P. falciparum compared to other species.
Filariasis (Wuchereria bancrofti, Brugia malayi): Transmitted by Culex mosquito (W. bancrofti) or Mansonia (B. malayi). Adult worms reside in lymphatic vessels → lymphatic obstruction → lymphoedema, elephantiasis, hydrocele. Microfilariae circulate in blood (nocturnal periodicity for W. bancrofti — peak at night matching Culex feeding time). Drug targets: microfilariae (for transmission control) and adult worms (for disease prevention).
Therapeutic Goals: Tissue Kill, Radical Cure, and Transmission Prevention
Each disease group requires pharmacotherapy that addresses multiple biological targets simultaneously — which is why monotherapy often fails:
Amoebiasis: Two therapeutic goals: (1) kill invasive trophozoites in tissue (colon wall, liver abscess) — achieved by metronidazole or tinidazole; (2) eradicate luminal cysts to prevent ongoing transmission and reinfection — metronidazole does NOT reliably achieve this (poor concentration in colonic lumen) → must add a luminal amoebicide (diloxanide furoate or paromomycin). Prescribing metronidazole alone for symptomatic amoebiasis treats the invasive form but leaves the patient a cyst-passer who will reinfect others and themselves.
Kala-azar: Goal — kill all intramacrophage amastigotes in the reticuloendothelial system. Incomplete kill → relapse and resistance emergence. Treatment failure in India is compounded by: high rates of antimonial resistance in Bihar (making sodium stibogluconate obsolete there); HIV co-infection causing immune failure and high relapse rates with standard regimens.
Malaria — multiple goals: (1) Blood-stage schizonticide — reduces parasitaemia, terminates acute episode, prevents severe malaria; (2) Radical cure (vivax/ovale only) — kill hypnozoites with primaquine (the ONLY available hypnozoite-active drug globally); (3) Gametocytocide — primaquine kills P. falciparum gametocytes, interrupting onward mosquito transmission; (4) Causal prophylaxis — drugs active against exoerythrocytic forms (doxycycline, proguanil) prevent establishment of hepatic schizogony in exposed travellers.
Filariasis: Two goals: (1) microfilaricidal (kills circulating microfilariae — reduces transmission); (2) macrofilaricidal (kills adult worms — prevents disease progression and reinfection). DEC and ivermectin are primarily microfilaricidal. Doxycycline (targeting endosymbiotic Wolbachia bacteria in adult worms — depleting Wolbachia → adult worm death over months) is uniquely macrofilaricidal.
Antiprotozoal and Antifilariasis Drugs by Disease Target
Amoebiasis Pharmacotherapy
Amoebiasis is treated with a two-drug sequential strategy: a tissue amoebicide first (to treat invasive disease), followed by a luminal amoebicide (to clear residual intraluminal cysts).
Metronidazole — first-line tissue amoebicide:
- Mechanism: nitroimidazole prodrug; reduced by ferredoxin oxidoreductase (enzyme present in anaerobes and protozoa — absent in aerobic human cells, conferring selectivity) → reactive nitroso radical → DNA strand breaks → cell death.
- Dose for amoebiasis: 400–800mg TDS × 7–10 days (amoebic dysentery); 750mg TDS × 7–10 days (amoebic liver abscess).
- Clinical cure of liver abscess: 70–90% respond to metronidazole alone; aspiration is rarely needed (indicated: abscess >10cm, risk of rupture, poor response to metronidazole at 72 hours, left-lobe abscess near pericardium).
- ADRs: metallic taste (very common), nausea/vomiting, peripheral neuropathy with prolonged use, disulfiram-like reaction with alcohol — inhibits acetaldehyde dehydrogenase → acetaldehyde accumulation → flushing, nausea, palpitations. Warn patients strictly: avoid all alcohol during treatment AND for 48 hours after the last dose.
Diloxanide furoate — luminal amoebicide:
- Mechanism: not fully elucidated; poorly absorbed from GI tract → achieves high luminal concentrations → kills intraluminal trophozoites and cysts directly within the colonic lumen.
- Dose: 500mg TDS × 10 days. Given AFTER completing metronidazole (or tinidazole) course.
- Use: (a) asymptomatic cyst passers — diloxanide alone; (b) symptomatic amoebic dysentery/liver abscess — after metronidazole, complete a diloxanide course to eliminate residual luminal cysts.
- ADRs: minimal (flatulence, mild nausea — mostly luminal action with negligible systemic absorption).
Tinidazole — an alternative to metronidazole with a longer half-life (allowing shorter course): 2g/day × 2–3 days (amoebic dysentery); 2g/day × 3–5 days (liver abscess). Better tolerated than metronidazole (fewer GI effects). Same mechanism (nitroimidazole) and same alcohol-disulfiram interaction.
Paromomycin — aminoglycoside; purely luminal amoebicide (not absorbed); used as alternative to diloxanide furoate for asymptomatic cyst passers. Not recommended in pregnancy.
Sequential Therapy in Amoebiasis
SELF-CHECK
A patient with amoebic liver abscess is treated with metronidazole 750mg TDS × 10 days and recovers completely (fever resolves, abscess resolves on ultrasound). What additional treatment is required and why?
A. No further treatment needed — metronidazole has eliminated all amoebic forms
B. Add diloxanide furoate 500mg TDS × 10 days to eliminate residual luminal cysts and prevent relapse/transmission
C. Add chloroquine to prevent amoebic recurrence in the liver
D. Repeat metronidazole for another 7 days to ensure complete tissue sterilisation
Reveal Answer
Answer: B. Add diloxanide furoate 500mg TDS × 10 days to eliminate residual luminal cysts and prevent relapse/transmission
Metronidazole is an excellent tissue amoebicide (kills invasive trophozoites in the colon wall and liver) but does not reliably eliminate intraluminal cysts — it achieves poor luminal concentrations. After clinical cure with metronidazole, the patient may continue to harbour luminal E. histolytica cysts, remaining a potential source of reinfection and transmission to others. Diloxanide furoate 500mg TDS × 10 days, given after metronidazole, eliminates these residual luminal cysts and prevents relapse. This two-drug sequential strategy (tissue amoebicide → luminal amoebicide) is the standard of care for all symptomatic amoebiasis.