Page 22 of 46
PH8.7 | PH8.7 | Protozoal and Vector-Borne Disease Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Kala-Azar (Visceral Leishmaniasis) Pharmacotherapy
Visceral leishmaniasis (kala-azar) in India is caused by Leishmania donovani transmitted by the Phlebotomus argentipes sandfly. India — particularly the Bihar-Bengal-Jharkhand cluster — accounts for over 70% of global kala-azar cases. Untreated kala-azar is nearly 100% fatal. Treatment has been revolutionised by the introduction of liposomal amphotericin B (L-AmB) as first-line therapy in India.
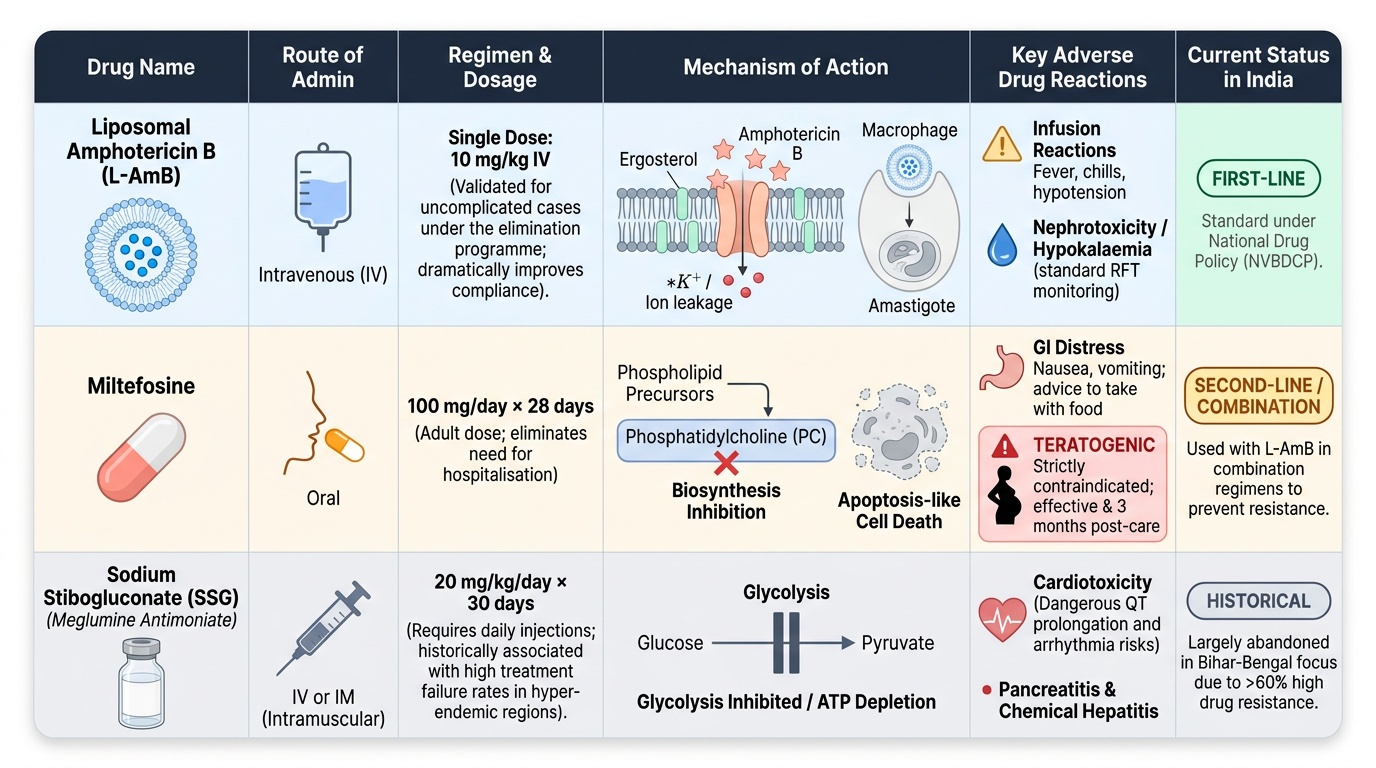
Liposomal Amphotericin B (L-AmB) — first-line in India:
- Mechanism: amphotericin B binds ergosterol in the leishmanial cell membrane (protozoa have ergosterol, not cholesterol — the basis of selective toxicity), forming ion-conducting pores → membrane depolarisation → cell lysis. The liposomal formulation is preferentially phagocytosed by macrophages in the reticuloendothelial system — exactly where L. donovani amastigotes reside — achieving targeted drug delivery.
- National Drug Policy India (NVBDCP): single-dose L-AmB 10mg/kg IV has been validated for uncomplicated kala-azar and is the standard treatment under the elimination programme. Single-dose dramatically improves adherence and programme implementation vs multi-dose schedules.
- ADRs: significantly reduced vs conventional amphotericin B. Infusion reactions (fever, chills, hypotension — acute during infusion; premedicate with paracetamol + antihistamine + hydration). Nephrotoxicity rare at standard VL doses (but monitor RFT). Hypokalaemia.
Miltefosine — first oral drug for kala-azar:
- Mechanism: phospholipid analogue; inhibits leishmanial phosphatidylcholine biosynthesis and signal transduction pathways; also induces apoptosis-like death in Leishmania.
- Dose: 100mg/day (adult >25kg) × 28 days orally.
- Advantages: oral administration; eliminates need for hospitalisation.
- ADRs: GI adverse effects (nausea, vomiting — take with food); teratogenic — causes embryonic death and fetal malformations in animal studies; absolutely contraindicated in pregnancy; effective contraception required during treatment and for 3 months after.
- Use in combination with L-AmB (shorter L-AmB course + miltefosine) in India to prevent resistance emergence — LEAP trial showed combination non-inferior with potentially lower resistance risk.
Sodium Stibogluconate (SSG) / Meglumine antimoniate — pentavalent antimony compounds (historical):
- Mechanism: inhibits leishmanial glycolysis and fatty acid oxidation; requires reduction to trivalent antimony (active form) within macrophages.
- No longer used as first-line in Bihar, India — >60% clinical resistance documented due to widespread unregulated use. Still used in some African kala-azar settings where L-AmB is unavailable.
- ADRs: pancreatitis, hepatotoxicity, cardiotoxicity (QT prolongation), myalgia, nephrotoxicity.
Paromomycin (aminoglycoside — injectable): bactericidal against Leishmania (protein synthesis inhibition, membrane disruption); 11mg/kg/day IM × 21 days; now used mainly in combination regimens in India.
Provided image
Malaria Pharmacotherapy
Malaria pharmacotherapy requires matching the drug to the parasite species AND the clinical presentation (uncomplicated vs severe malaria).
Classification of antimalarial drugs by life-cycle stage:
- Blood schizonticides (active against asexual erythrocytic stages — the clinical disease stage): chloroquine, quinine, artemisinin derivatives, mefloquine, lumefantrine, amodiaquine, piperaquine, atovaquone-proguanil.
- Tissue schizonticides (exoerythrocytic stage — liver): Primaquine (active vs hypnozoites in vivax/ovale — radical cure); proguanil, doxycycline (causal prophylaxis — prevent hepatic schizogony).
- Gametocytocides: Primaquine (kills P. falciparum gametocytes — reduces transmission); artemisinin derivatives have some gametocytocidal activity.
P. falciparum malaria (uncomplicated): First-line — Artemisinin-based Combination Therapy (ACT):
- Artemether-lumefantrine (AL): fixed-dose combination, 6-dose regimen over 3 days. Standard national first-line.
- Artesunate-amodiaquine or Dihydroartemisinin-piperaquine: alternatives.
- Artemisinin mechanism: the endoperoxide bridge of artemisinin is activated by haem iron (within the parasite's food vacuole) → free radical generation → alkylation of parasite proteins → rapid parasite killing. Fastest-acting antimalarial drug.
- Partner drug (lumefantrine, amodiaquine, piperaquine) provides sustained blood-stage suppression and prevents artemisinin resistance selection.
P. falciparum malaria (severe): IV artesunate — drug of choice. SEAQUAMAT trial (adults in Asia) and AQUAMAT trial (children in Africa): IV artesunate superior to IV quinine in reducing mortality in severe P. falciparum. IV artesunate 2.4mg/kg at 0, 12, 24 hours, then daily; switch to oral ACT once tolerating orally. Quinine IV (quinine dihydrochloride) — reserve for settings without artesunate; risk of hypoglycaemia (stimulates insulin secretion), hypotension, QT prolongation, cinchonism (tinnitus, hearing loss, vision changes).
P. vivax malaria:
- Blood stage: chloroquine (25mg/kg over 3 days = 10mg/kg day 1, 10mg/kg day 2, 5mg/kg day 3) — P. vivax remains largely chloroquine-sensitive in India (unlike P. falciparum). Note: chloroquine-resistant P. vivax has emerged in PNG, Indonesia, and parts of India (Andaman and Nicobar) — ACT used for resistant vivax.
- Radical cure (hypnozoites): Primaquine 0.25mg/kg/day × 14 days (WHO standard) or 15mg/day × 14 days (Indian schedule). G6PD TESTING IS MANDATORY before primaquine. In G6PD-deficient patients: weekly primaquine 0.75mg/kg/week × 8 weeks (less haemolytic — slower haemolytic red cells replaced before reaching toxic threshold).
Chloroquine mechanism and resistance: Chloroquine accumulates in the parasite's digestive vacuole (food vacuole) by ion trapping (weak base, accumulates 1000-fold in acid pH). In the food vacuole, the parasite digests haemoglobin → releases ferriprotoporphyrin IX (FP) (toxic free haem). Normally, parasites polymerise FP into inert haemozoin (malaria pigment). Chloroquine inhibits FP polymerisation → free FP accumulates → parasite cell membrane disruption. Chloroquine resistance in P. falciparum: mutation in PfCRT (Plasmodium falciparum chloroquine resistance transporter — a lysosomal transporter) pumps chloroquine out of the food vacuole, preventing accumulation to inhibitory levels.
Primaquine: 8-aminoquinoline; unique activity vs hypnozoites (P. vivax, P. ovale) and vs P. falciparum gametocytes. Mechanism incompletely understood — generates reactive oxygen species that may be toxic to mitochondria of the parasite. G6PD deficiency interaction: primaquine generates oxidative stress in red blood cells; G6PD-deficient RBCs cannot regenerate NADPH to neutralise oxidative stress → haemolysis. Clinical: dark red-brown urine (haemoglobinuria), anaemia, jaundice within 1–3 days of starting primaquine. G6PD status MUST be tested before giving primaquine — qualitative point-of-care tests are sufficient for ruling out severe deficiency.
Malaria prophylaxis: Doxycycline 100mg/day (starting 1–2 days before travel, continuing 28 days after — causal and suppressive); chloroquine (for P. vivax endemic areas without resistance); mefloquine (weekly, neuropsychiatric ADRs — anxiety, depression, vivid dreams, psychosis — contraindicated in psychiatric history); atovaquone-proguanil (Malarone — well-tolerated, short post-travel course 7 days, expensive).
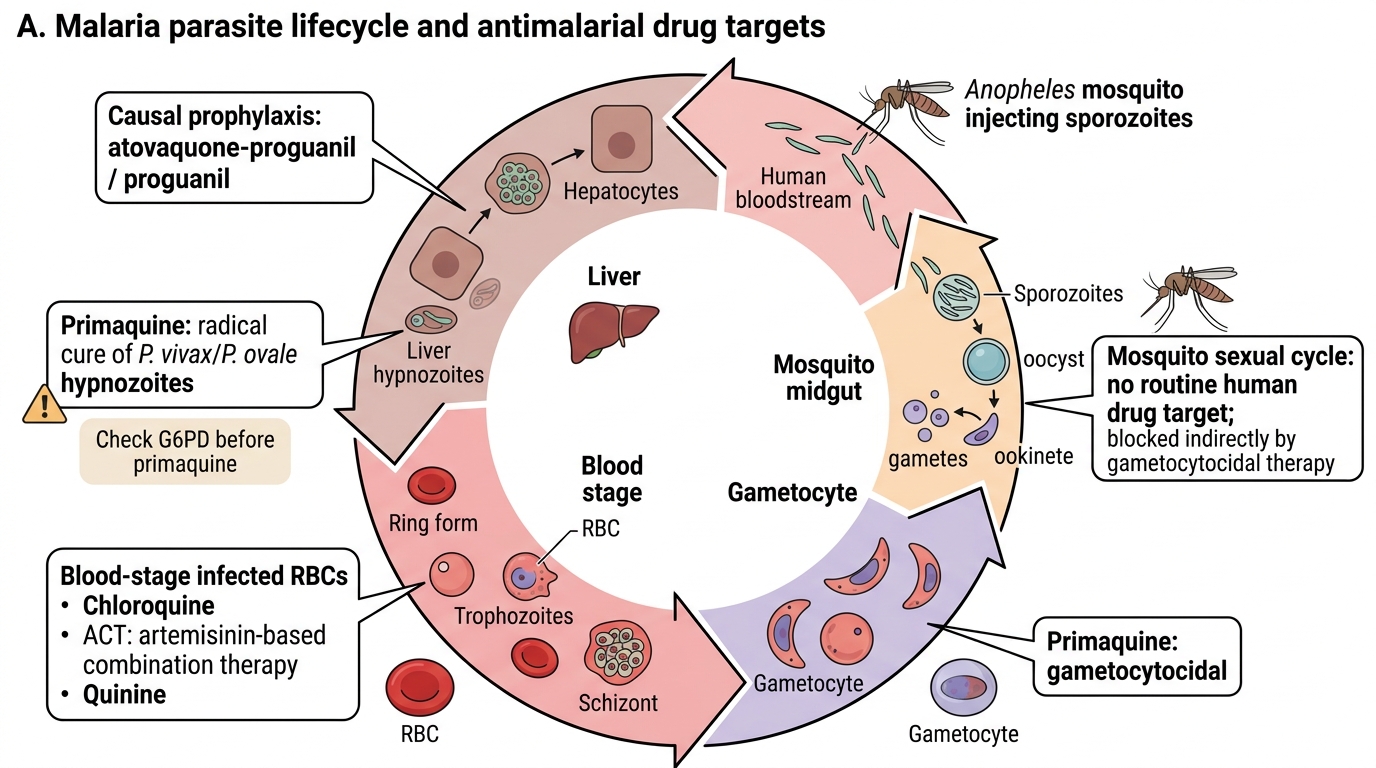
Malaria Lifecycle and Antimalarial Drug Targets
SELF-CHECK
A 22-year-old man presents with relapsing P. vivax malaria — his third episode in 18 months, each treated with chloroquine. He was never given primaquine. G6PD testing shows normal activity. What is the appropriate management?
A. Switch to artesunate-amodiaquine ACT — chloroquine resistance has developed in P. vivax
B. Chloroquine for blood-stage clearance plus primaquine 15mg/day × 14 days for radical cure of hypnozoites
C. Chloroquine alone — vivax malaria does not relapse; his recurrences are new infections
D. Chloroquine plus doxycycline for radical cure — doxycycline is the hypnozoitocidal drug of choice
Reveal Answer
Answer: B. Chloroquine for blood-stage clearance plus primaquine 15mg/day × 14 days for radical cure of hypnozoites
P. vivax forms hypnozoites (dormant liver-stage parasites) that can reactivate months to years after the primary infection — causing relapses that are clinically indistinguishable from new infections. Treating the blood stage with chloroquine alone eliminates the acute episode but leaves hypnozoites untouched, allowing repeated relapses. Radical cure requires primaquine 15mg/day × 14 days to kill hypnozoites. G6PD testing is confirmed normal in this patient, so primaquine can be given safely. Doxycycline does NOT kill hypnozoites — it is a causal prophylactic that prevents hepatic schizogony before merozoite emergence, not a hypnozoitocide. Chloroquine resistance in P. vivax is not the correct interpretation of repeated episodes without prior radical cure.
Filariasis Pharmacotherapy
Lymphatic filariasis (LF) caused by Wuchereria bancrofti is the second leading cause of long-term disability globally after leprosy. India aims to eliminate LF by 2030 through mass drug administration (MDA). The pharmacotherapy involves drugs with distinct mechanisms targeting different parasitic stages.
Diethylcarbamazine (DEC):
- Mechanism: microfilaricidal — enhances host immune system recognition and killing of microfilariae (alters microfilarial surface — makes them 'visible' to the immune system); some macrofilaricidal activity (incomplete). Mechanism involves nitric oxide signalling and arachidonic acid pathway modulation.
- Dose: 6mg/kg/day in 3 divided doses × 12 days for LF treatment; single dose 6mg/kg for MDA.
- Mazzotti reaction: Rapid death of microfilariae → release of Wolbachia and larval antigens → inflammatory reaction (fever, urticaria, pruritus, arthralgia, lymphadenitis). Common in heavily infected individuals given DEC. Manage with antihistamines and NSAIDs.
- Contraindications: Active onchocerciasis (river blindness — DEC causes severe ocular reactions from dying microfilariae); avoid in Loa loa co-infected areas (high microfilarial load + DEC → encephalopathy, death — specifically documented in Cameroon/Central Africa). In India, LF coexists with loiasis in Northeast India — caution required.
Ivermectin:
- Mechanism: binds glutamate-gated chloride ion channels in invertebrate nerve and muscle cells → hyperpolarisation → paralysis and death of microfilariae and larval stages. These channels are absent in mammals — selective toxicity.
- Primarily microfilaricidal; single-dose effect lasts ~12 months; also active vs ectoparasites (scabies, lice), intestinal helminths (strongyloides).
- ADRs: Mazzotti-like reaction (dying microfilariae — same as DEC); ivermectin is generally well-tolerated. Contraindicated in pregnancy (limited safety data); avoid in children <15kg.
Albendazole:
- Mechanism: binds β-tubulin in helminths → inhibits microtubule polymerisation → impaired glucose uptake and cellular function → worm death. Primarily active against adult worms (macrofilaricidal effect is weak); in MDA, albendazole is used for its synergistic action with DEC or ivermectin and for clearing intestinal helminths simultaneously.
- Dose in MDA: 400mg single dose.
WHO Mass Drug Administration (MDA) for LF elimination:
- Strategy: annual single-dose MDA to the entire at-risk population × 5–6 years — interrupts transmission by reducing microfilaraemia below the threshold for mosquito infection.
- Regimens: (a) DEC 6mg/kg + albendazole 400mg (standard two-drug MDA — in areas without onchocerciasis or loiasis co-endemicity); (b) Ivermectin + albendazole (in onchocerciasis co-endemic areas — DEC contraindicated); (c) DEC + albendazole + ivermectin (triple-drug MDA — newer approach achieving faster transmission interruption in trials).
Doxycycline for macrofilaricidal activity: W. bancrofti adult worms carry Wolbachia endosymbiotic bacteria as obligate intracellular symbionts. Wolbachia are essential for worm fertility and survival. Doxycycline 200mg/day × 4–6 weeks depletes Wolbachia → adult worm sterilisation and eventual death over 6–12 months. This is the only currently available drug that reliably kills adult worms (macrofilaricidal). Used in individual patient treatment when chronic lymphoedema is present (targeting the worm population, not just microfilariae).
SELF-CHECK
During a filariasis MDA programme, a health worker proposes using DEC alone in an area co-endemic for both lymphatic filariasis and onchocerciasis (river blindness). What is the serious risk of this decision and what is the correct drug regimen?
A. DEC alone causes resistance in Wuchereria bancrofti; use ivermectin + albendazole + DEC
B. DEC causes severe ocular inflammation in onchocerciasis patients due to rapid killing of Onchocerca volvulus microfilariae in the eye; use ivermectin + albendazole instead
C. DEC interacts with albendazole to cause severe hepatotoxicity; MDA should be suspended
D. DEC is safe but monotherapy MDA is ineffective; dual DEC + albendazole is the minimum
Reveal Answer
Answer: B. DEC causes severe ocular inflammation in onchocerciasis patients due to rapid killing of Onchocerca volvulus microfilariae in the eye; use ivermectin + albendazole instead
In areas co-endemic for both lymphatic filariasis and onchocerciasis (river blindness — caused by Onchocerca volvulus), DEC is absolutely contraindicated. Rapid killing of O. volvulus microfilariae in the cornea and anterior chamber of the eye by DEC causes the 'Mazzotti reaction' locally — severe uveitis, punctate keratitis, and potentially irreversible visual loss. Ivermectin (which is safe in onchocerciasis — kills microfilariae without the severe ocular inflammation that DEC causes) + albendazole is the appropriate MDA regimen for onchocerciasis-LF co-endemic areas. Adding DEC (triple-drug MDA) is only appropriate in areas without onchocerciasis co-endemicity.