Page 25 of 46
PH8.8 | PH8.8 | Antifungal Drugs — SDL Guide — SDL Guide
Learning Objectives
- Explain the types, kinetics, dynamics, and adverse effects of drugs used for fungal infections
- Classify antifungal drugs by their mechanism of action and target site
- Select appropriate antifungal therapy for common clinical scenarios including oral/vaginal candidiasis, invasive candidiasis, Aspergillus infection, cryptococcal meningitis, and dermatophytosis
INSTRUCTIONS
Fungal infections have increased dramatically over the past three decades, driven by growing populations of immunocompromised patients (HIV/AIDS, haematological malignancies, solid organ transplant recipients, critically ill patients on broad-spectrum antibiotics). As a clinician, you will encounter both superficial fungal infections (extremely common — oral thrush in HIV patients, vulvovaginal candidiasis, dermatophytosis) and life-threatening invasive infections (invasive aspergillosis, candidaemia, cryptococcal meningitis). The pharmacological challenge is unique: fungi are eukaryotes sharing many metabolic processes with human cells, making selective toxicity more difficult than for bacteria.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 59 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 60 (textbook)
- IDSA Guidelines: Aspergillosis 2016; Candidiasis 2016; Cryptococcal Meningitis 2010 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 18-year-old with acute myeloid leukaemia (AML) is in neutrophil nadir (ANC <100) following chemotherapy. He develops persistent fever despite broad-spectrum antibiotics (meropenem + vancomycin) for 5 days. CT chest shows bilateral nodular infiltrates with a 'halo sign.' Galactomannan antigen is positive. Invasive pulmonary aspergillosis is diagnosed. The resident prescribes fluconazole — readily available, familiar, well-tolerated. The attending overrules: 'Aspergillus is intrinsically resistant to fluconazole. This patient needs voriconazole.' The resident asks: 'Why can't fluconazole treat Aspergillus if it targets the same enzyme as voriconazole?' The answer lies in the structural differences between Candida and Aspergillus CYP51 enzymes — and understanding this saves this patient's life. A treatment delay of 48 hours in invasive aspergillosis increases mortality by 30%.
WHY THIS MATTERS
Fungal infections cause approximately 1.5 million deaths annually globally — more than malaria, and approaching tuberculosis mortality. In India, the COVID-19 pandemic revealed the devastating potential of mucormycosis ('black fungus') in diabetics given corticosteroids — tens of thousands of cases occurred in 2021. Vulvovaginal candidiasis affects 75% of women at least once in their lifetime. Dermatophytosis (ringworm) is ubiquitous in India's tropical climate. As a physician, you prescribe antifungals constantly — topical clotrimazole for tinea, fluconazole for oral thrush, voriconazole for neutropenic aspergillosis. Getting the choice right requires mechanistic understanding, not pattern memorisation.
RECALL
From previous SDLs: ergosterol is the principal sterol in fungal membranes (analogous to cholesterol in human cell membranes). Fungi use ergosterol for membrane fluidity, integrity, and as an anchor for membrane proteins. Because ergosterol is absent in human cells (which use cholesterol) and is structurally different, it provides the most exploitable selective toxicity target for antifungal drugs — exactly as bacterial cell walls (absent in human cells) provided the target for β-lactams. Amphotericin B targets ergosterol in both fungi and Leishmania (which also uses ergosterol) — explaining its use in kala-azar (from the protozoal SDL). Azoles as CYP inhibitors: azoles inhibit fungal CYP51 (14α-demethylase) — but they also inhibit human CYP3A4/2C9/2C19 to varying degrees, causing drug interactions.
Fungal Infection Pathophysiology: Why Antifungals Are Harder Than Antibacterials
The fundamental pharmacological challenge of treating fungal infections is that fungi are eukaryotes — like human cells, they have a nucleus, mitochondria, ribosomes identical in structure to the human 80S ribosome, and similar signalling pathways. This eukaryotic nature eliminates the most productive antibacterial targets: bacteria-specific 70S ribosomes, cell-wall peptidoglycan, and prokaryotic DNA gyrase.
The exploitable differences between fungal and human cells are fewer but clinically leverageable:
1. Ergosterol — the principal sterol of fungal cell membranes (humans use cholesterol). Structural differences between ergosterol and cholesterol allow certain drugs (polyenes, azoles, allylamines) to selectively target fungal membranes or their ergosterol biosynthesis pathway.
2. β-1,3-D-glucan — a polysaccharide component of the fungal cell wall, absent in mammalian cells. This is the target of echinocandins.
3. Cytosine deaminase — present in fungi (converts 5-FC to 5-FU, the active form); mammalian cells lack this enzyme in significant amounts, providing selectivity for flucytosine.
The clinical spectrum of fungal disease ranges from superficial (dermatophytosis, oral thrush, vaginal candidiasis — primarily in immunocompetent patients) to deep-seated/systemic (pneumocystosis, histoplasmosis, coccidioidomycosis — regional endemics) to life-threatening invasive (candidaemia, invasive aspergillosis, mucormycosis, cryptococcal meningitis — primarily in immunocompromised hosts). The severity of immunosuppression determines the likely fungal pathogen and the required intensity of antifungal therapy.
Key clinical contexts triggering antifungal need in India:
- HIV/AIDS — oral and oesophageal candidiasis; cryptococcal meningitis; Pneumocystis jirovecii pneumonia
- Neutropenia post-chemotherapy — invasive aspergillosis, invasive candidiasis
- Solid organ transplant recipients — Aspergillus, non-albicans Candida, Cryptococcus
- Broad-spectrum antibiotics → microbiome disruption → Candida overgrowth (vaginal candidiasis; C. difficile does not apply here but the ecological principle does)
- Corticosteroids + uncontrolled diabetes → mucormycosis (COVID-19 pandemic illustration)
- Prolonged ICU stay + central venous catheter → candidaemia
Therapeutic Goal: Exploit Ergosterol-Based Selective Toxicity
The central therapeutic strategy in antifungal pharmacology is exploiting the ergosterol pathway as the point of maximal selective toxicity. Three major drug classes attack this pathway at different points, and understanding their positions in the pathway prevents confusion about their mechanisms and spectra:
The ergosterol biosynthesis pathway (simplified):
Acetate → Squalene → [Squalene epoxidase: TERBINAFINE target] → Lanosterol → [14α-demethylase/CYP51: AZOLE target] → Ergosterol → [Ergosterol in membrane: POLYENE target]
- Polyenes (amphotericin B, nystatin): act at the END of the pathway — bind ergosterol already incorporated into the membrane, forming channels → ion leak → cell death. These are fungicidal because they physically disrupt the existing membrane, regardless of whether the organism is actively synthesising ergosterol.
- Azoles: act in the MIDDLE — inhibit 14α-demethylase (CYP51), blocking the conversion of lanosterol to ergosterol. This depletes ergosterol AND causes accumulation of toxic 14α-methylated sterols. Azoles are primarily fungistatic (they slow synthesis but cannot drain existing ergosterol from the membrane), requiring host immune clearance to kill the organism.
- Allylamines (terbinafine): act at the BEGINNING — inhibit squalene epoxidase, blocking squalene → squalene oxide conversion. This depletes ergosterol AND causes toxic squalene accumulation (directly membrane-disruptive). More fungicidal than azoles for dermatophytes.
The additional target — β-1,3-glucan synthase (echinocandins) — is orthogonal to the ergosterol pathway, targeting cell wall synthesis rather than membrane ergosterol. This is why echinocandins and azoles can be used synergistically: different targets, potentially additive mechanisms.
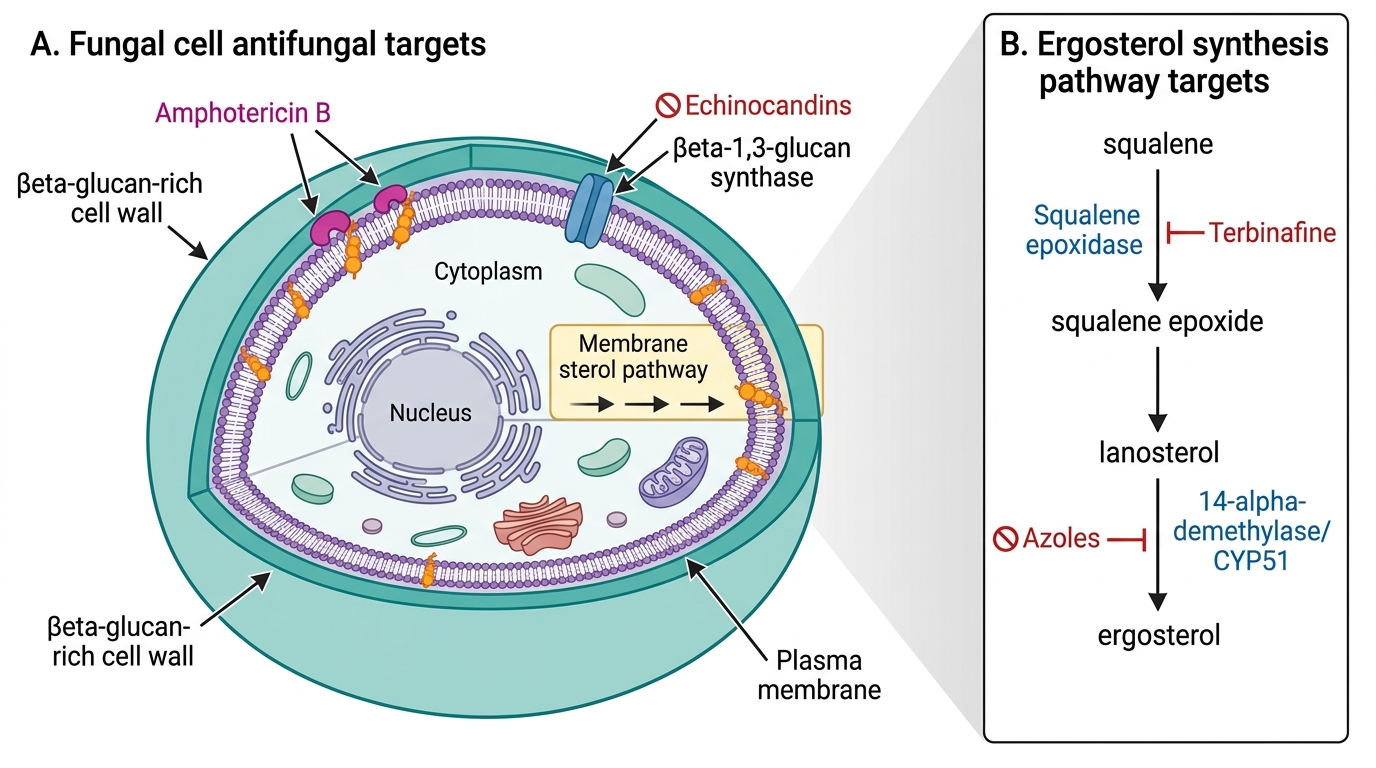
Antifungal Drug Target Sites in the Fungal Cell
Classification of Antifungal Drugs by Target
A systematic classification by pharmacological target organises all antifungal drugs logically:
Class 1 — Polyenes (ergosterol-binding):
- Amphotericin B (AmB): broad-spectrum fungicidal (Candida, Aspergillus, Cryptococcus, Mucor, dimorphic fungi); IV formulation; significant nephrotoxicity (conventional). Lipid formulations (liposomal AmB/L-AmB, amphotericin B lipid complex/ABLC, amphotericin B colloidal dispersion/ABCD) reduce nephrotoxicity by altering pharmacokinetics and RES uptake.
- Nystatin: too toxic for systemic use; topical only (oral thrush as oral suspension — 'swish and swallow'; vaginal candidiasis as pessary; skin candidiasis as cream).
Class 2 — Azoles (CYP51/14α-demethylase inhibitors):
- Imidazoles (2 nitrogen atoms in ring): clotrimazole, miconazole — topical only (less CYP-selective, more human CYP inhibition at systemic levels).
- Triazoles (3 nitrogen atoms — more CYP51-selective): fluconazole, itraconazole, voriconazole, posaconazole, isavuconazole — systemic use.
Class 3 — Echinocandins (β-1,3-glucan synthase inhibitors):
- Caspofungin, micafungin, anidulafungin — IV only; fungicidal vs Candida; NOT active vs Cryptococcus (which has minimal β-glucan in its polysaccharide capsule).
Class 4 — Allylamines (squalene epoxidase inhibitors):
- Terbinafine — primarily for dermatophytes; oral (systemic) for onychomycosis; topical for tinea pedis/corporis.
Class 5 — Others:
- Flucytosine (5-FC): antimetabolite (DNA/RNA synthesis); ONLY in combination with AmB for cryptococcal meningitis; NOT used alone (rapid resistance).
- Griseofulvin: disrupts microtubule function → impairs mitotic spindle → antimitotic effect against dermatophytes; oral; long course required (months for nail infections); largely superseded by terbinafine.