Page 26 of 46
PH8.8 | PH8.8 | Antifungal Drugs — SDL Guide — SDL Guide (Part 2)
Polyenes and Azoles: Mechanisms, Spectra, and ADRs
Amphotericin B (conventional IV formulation):
- Mechanism: the large polyene macrolide ring has a hydrophobic face (interacts with ergosterol) and a hydrophilic face (lines the pore interior). AmB inserts into the fungal membrane as ergosterol-AmB complexes → forms transmembrane ion-conducting pores → K⁺ and Mg²⁺ leak out → membrane potential lost → cell death. Fungicidal against most susceptible fungi.
- Spectrum: Candida spp. (most including non-albicans), Aspergillus, Cryptococcus, Mucor/Rhizopus (mucormycosis — AmB is first-line), dimorphic fungi (Histoplasma, Blastomyces, Coccidioides), Leishmania.
- ADRs: (a) Nephrotoxicity — the dose-limiting toxicity; proximal renal tubular damage, distal tubular acidosis, hypomagnesaemia, hypokalaemia; creatinine often doubles. Prevention: adequate IV hydration before and after infusion (500mL normal saline), avoid nephrotoxic co-medications (aminoglycosides, NSAIDs, ciclosporin). Monitor Cr, K, Mg daily during therapy. (b) Infusion reactions — fever, chills, rigors, hypotension during infusion (30–60 minutes into infusion); due to cytokine release (TNF-α, IL-1, PGE2). Premedication: paracetamol 1g + diphenhydramine 25–50mg + hydrocortisone 50mg IV (if severe) before infusion. (c) Anaemia (erythropoietin suppression). Lipid formulations (L-AmB) reduce nephrotoxicity by altering pharmacokinetics (less renal tubular accumulation) — but are significantly more expensive.
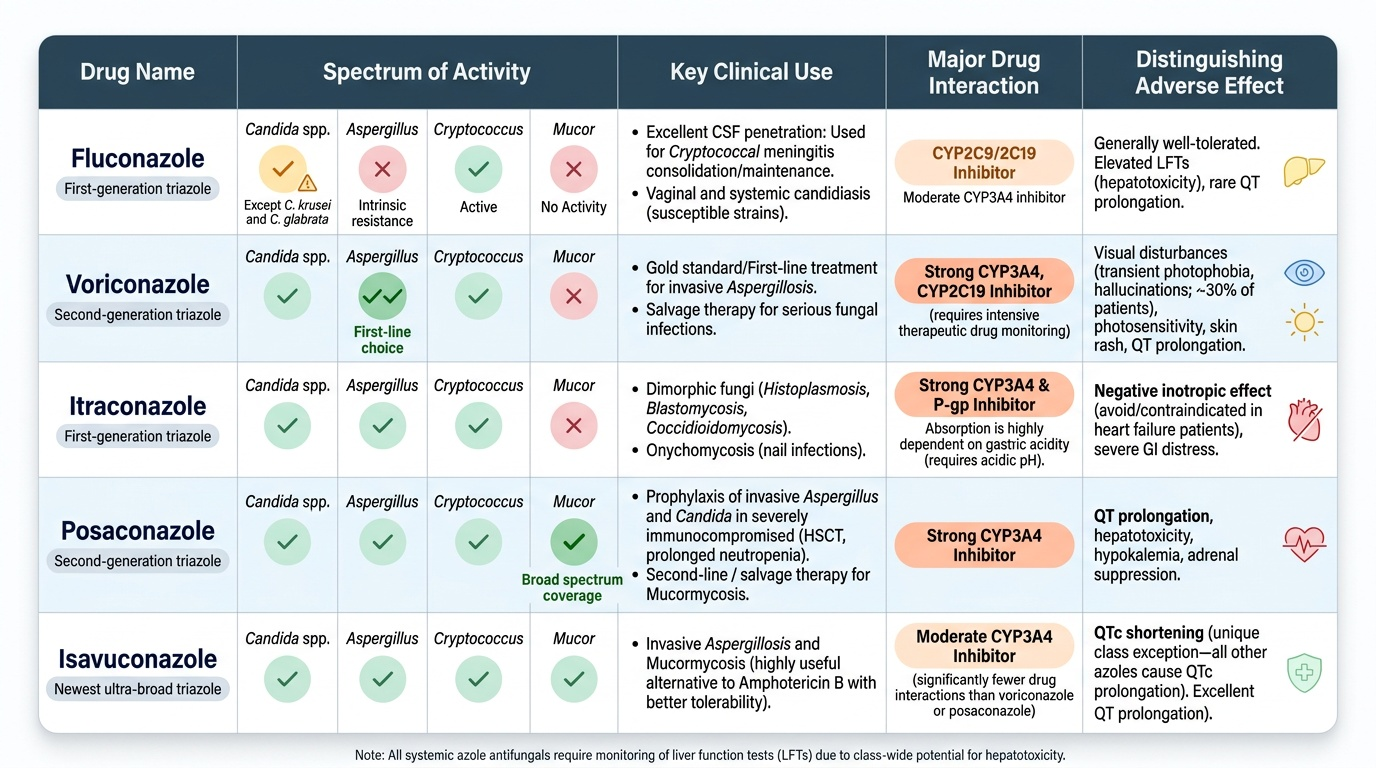
Fluconazole (first-generation triazole):
- Mechanism: inhibits CYP51 (14α-demethylase) → blocks lanosterol → ergosterol conversion → ergosterol depletion + accumulation of 14α-methylsterols → membrane dysfunction. Fungistatic (requires intact immune function for fungal killing).
- Unique PK: highly water-soluble; excellent oral bioavailability (>90%); excellent CSF penetration (CSF levels 80% of plasma — why it is used for cryptococcal meningitis consolidation/maintenance).
- Spectrum: Candida albicans (most isolates), Candida tropicalis, Cryptococcus neoformans. NOT Aspergillus (fluconazole does not inhibit Aspergillus CYP51 isoform at achievable plasma concentrations — intrinsic resistance — this is the clinical trap in the hook scenario). NOT Candida krusei (intrinsic resistance) or Candida glabrata (high MIC).
- ADRs: well-tolerated; GI (nausea); hepatotoxicity (elevated LFTs, rare fulminant hepatic failure); QT prolongation (dose-related); CYP3A4 and CYP2C9 inhibitor → elevated warfarin (INR up), ciclosporin, tacrolimus, statins, phenytoin levels.
Voriconazole (extended-spectrum triazole):
- Spectrum: Aspergillus spp. (the first-line treatment for invasive aspergillosis — Walsh NEJM 2002, superior to conventional AmB); Candida spp. (including C. krusei and C. glabrata); Fusarium; Scedosporium.
- Unique ADRs: (a) Visual disturbances (photopsia) — transient, dose-related; patients report bright lights, colour changes, blurring during the first weeks of treatment. Resolves spontaneously. Most common unique ADR of voriconazole. (b) Hepatotoxicity — monitor LFTs. (c) Phototoxicity — prolonged voriconazole → increased skin cancer risk. (d) CYP2C19 polymorphism in metabolism: poor metabolisers (absent CYP2C19 — common in Asians ~15–20%) accumulate 4–10× higher levels → toxicity; ultra-rapid metabolisers have subtherapeutic levels → treatment failure. Therapeutic drug monitoring (TDM) recommended (trough 1–5.5 mcg/mL). (e) Potent CYP3A4 inhibitor — drug interactions.
Itraconazole: Broad spectrum (Candida, Aspergillus, Cryptococcus, dimorphic fungi including Histoplasma, Blastomyces, Sporotrichosis); oral; capsule formulation requires acidic pH for absorption (take with food, not with proton pump inhibitors or antacids); solution (cyclodextrin) has better absorption. ADRs: hepatotoxicity; negative inotrope (avoid in cardiac failure); drug interactions (CYP3A4 inhibitor).
Posaconazole: Broadest-spectrum azole including Mucor/Rhizopus (mucormycosis) and most Candida spp.; oral suspension or tablets; used for prophylaxis in high-risk neutropenic patients and salvage therapy for mucormycosis.
Provided image
SELF-CHECK
An HIV-positive patient with CD4 count 50 cells/μL develops severe headache, fever, and confusion. CSF: Indian ink preparation shows encapsulated yeast, CSF cryptococcal antigen positive. Which antifungal regimen is most appropriate for induction therapy?
A. Fluconazole 800mg/day orally — excellent CSF penetration for Cryptococcus
B. Caspofungin IV — echinocandins are first-line for CNS fungal infections
C. Amphotericin B (liposomal) IV + flucytosine for 2 weeks, followed by fluconazole consolidation
D. Voriconazole IV — first-line for invasive fungal CNS infections
Reveal Answer
Answer: C. Amphotericin B (liposomal) IV + flucytosine for 2 weeks, followed by fluconazole consolidation
The standard induction regimen for HIV-associated cryptococcal meningitis (IDSA guidelines) is: L-AmB (or conventional AmB) + flucytosine for 2 weeks (induction), followed by fluconazole 400mg/day × 8 weeks (consolidation), then fluconazole 200mg/day (maintenance/secondary prophylaxis until immune reconstitution on ART). The combination of AmB + 5-FC provides synergistic fungicidal activity: AmB disrupts the membrane (enhances 5-FC entry); 5-FC inhibits DNA synthesis (pyrimidine analogue). Fluconazole monotherapy is inadequate for induction (lower fungicidal activity, slower CSF clearance); it is appropriate for consolidation/maintenance. Caspofungin has NO activity vs Cryptococcus (intrinsic resistance — minimal β-glucan in Cryptococcal capsule). Voriconazole has activity vs Cryptococcus but is not established as a preferred CNS cryptococcal therapy.
Echinocandins, Allylamines, and Other Antifungals
Echinocandins (caspofungin, micafungin, anidulafungin):
- Mechanism: cyclic lipopeptides that inhibit β-(1,3)-D-glucan synthase — an enzyme encoded by FKS1/FKS2 genes, responsible for polymerising glucose into β-glucan, a structural polysaccharide in the fungal cell wall. Inhibition reduces β-glucan content → cell wall weakness → osmotic lysis → cell death. This target is absent in mammalian cells — the reason echinocandins have an exceptionally wide safety margin and minimal drug interactions (not metabolised by CYP enzymes).
- Spectrum: Fungicidal vs Candida (including azole-resistant Candida krusei and C. glabrata); Fungistatic vs Aspergillus; No activity vs Cryptococcus (Cryptococcus has minimal β-glucan and a thick polysaccharide capsule that the echinocandin molecule cannot penetrate effectively — intrinsic resistance).
- Clinical use: invasive candidiasis/candidaemia (first-line, especially in azole-resistant or haemodynamically unstable patients); Aspergillus as second-line or salvage; NOT for Cryptococcus.
- IV formulation only (large lipopeptide — poor oral bioavailability); long half-lives allowing once-daily dosing.
- ADRs: Minimal — excellent tolerability profile. Histamine-mediated infusion reactions with rapid caspofungin infusion (administer over ≥1 hour). Transient liver enzyme elevations. No renal toxicity. No significant CYP interactions (a major advantage over azoles).
Terbinafine (allylamine):
- Mechanism: inhibits squalene epoxidase → blocks squalene → squalene oxide conversion → two toxic effects: (1) ergosterol depletion; (2) squalene accumulation (directly toxic to fungal membranes, disrupting their integrity). Fungicidal vs dermatophytes (Trichophyton, Epidermophyton, Microsporum) — particularly effective because the combination of ergosterol depletion + squalene toxicity kills dermatophytes more effectively than azoles.
- Spectrum: Dermatophytes (tinea pedis, tinea corporis, tinea cruris, onychomycosis). NOT Candida (terbinafine has poor activity vs Candida — squalene epoxidase isoform in Candida is less susceptible).
- PK: highly lipophilic; accumulates in skin, hair, nails (long tissue half-life → sustained nail levels during oral therapy for onychomycosis).
- ADRs: Hepatotoxicity (check LFTs at baseline; stop if LFTs >3× ULN — rare, but liver failure reported); GI (nausea, diarrhoea); taste disturbance (ageusia — reversible); headache. Dose: 250mg/day × 12 weeks for toenail onychomycosis (superior to griseofulvin which requires 6–18 months).
Flucytosine (5-FC):
- Mechanism: prodrug; cytosine permease in the fungal membrane transports 5-FC into the cell → fungal cytosine deaminase converts 5-FC to 5-fluorouracil (5-FU) → 5-FU incorporated into RNA (disrupts translation) AND converted to 5-FUMP (inhibits thymidylate synthase → blocks thymidine synthesis → inhibits DNA synthesis). Human cells lack significant cytosine deaminase activity — selective toxicity.
- NEVER use as monotherapy — single-step mutations in cytosine deaminase or permease cause rapid high-level resistance. Combine with amphotericin B (synergistic for cryptococcal meningitis): AmB disrupts the fungal membrane, increasing 5-FC uptake; 5-FC inhibits DNA synthesis — the combination is more rapidly fungicidal than either alone.
- ADRs: Myelosuppression (anaemia, leukopenia, thrombocytopenia) — because some 5-FU does form in the gut (from intestinal bacteria deaminating 5-FC) and is absorbed systemically → bone marrow toxicity. Monitor CBC weekly. Hepatotoxicity (elevated LFTs). Requires renal dose adjustment (renally excreted).
Griseofulvin:
- Mechanism: binds to tubulin, disrupting microtubule assembly → impairs mitotic spindle function → dermatophyte cells cannot complete cell division. Fungistatic. Active ONLY against dermatophytes.
- Uses: tinea capitis (preferred in children — griseofulvin has better paediatric data), tinea corporis (increasingly replaced by terbinafine). Onychomycosis requires 6–18 months; largely superseded by terbinafine.
- ADRs: GI (nausea, diarrhoea — take with fatty food for better absorption), headache, teratogenic in animals (avoid in pregnancy and for 1 month after in men + 6 months in women — may impair fertility), hepatotoxicity (rare), photosensitivity, peripheral neuropathy (prolonged use), drug interaction with warfarin (CYP inducer — reduces warfarin levels, like rifampicin).
SELF-CHECK
A 75-year-old diabetic on tacrolimus post-renal transplant develops candidaemia with Candida krusei (intrinsically fluconazole-resistant). Which antifungal is most appropriate?
A. Fluconazole 800mg daily loading dose — the loading dose achieves adequate levels for resistant strains
B. Voriconazole IV — active against Candida krusei and safer than amphotericin B
C. Caspofungin IV — echinocandins are fungicidal vs Candida krusei and have no significant drug interaction with tacrolimus
D. Amphotericin B conventional IV — broadest spectrum, definitively kills Candida krusei
Reveal Answer
Answer: C. Caspofungin IV — echinocandins are fungicidal vs Candida krusei and have no significant drug interaction with tacrolimus
Candida krusei is intrinsically resistant to fluconazole (loading doses do not overcome intrinsic resistance). Caspofungin (echinocandin) is first-line for candidaemia in this patient for three reasons: (1) fungicidal vs Candida krusei — echinocandins are active against all Candida spp. including azole-resistant strains; (2) no significant CYP drug interactions — critically important in a transplant patient on tacrolimus (whose levels are tightly monitored; azole CYP3A4 inhibitors dramatically increase tacrolimus levels, causing nephrotoxicity); (3) minimal nephrotoxicity (conventional AmB would worsen renal graft function). Voriconazole has activity vs C. krusei but inhibits tacrolimus metabolism (CYP3A4 inhibitor) — requires dose adjustment and monitoring, making caspofungin simpler and safer.
Clinical Decision-Making: Matching Antifungal to Clinical Syndrome
The clinical application of antifungal pharmacology follows a syndrome-based algorithm that integrates organism likelihood, site of infection, immune status, drug spectrum, and drug interactions.
Oral candidiasis (thrush): Most often C. albicans in HIV (CD4 <200), denture wearers, patients on inhaled corticosteroids. First-line: nystatin suspension (swish and swallow 4–6 hourly × 7–14 days) for mild disease; fluconazole 150mg single dose or 50–100mg daily × 7–14 days for moderate-severe or recurrent. Oesophageal candidiasis (dysphagia, retrosternal pain) — fluconazole 200–400mg/day × 14–21 days (IV if not tolerating oral).
Vulvovaginal candidiasis: Uncomplicated: topical clotrimazole 1% cream × 7 days OR oral fluconazole 150mg single dose. Complicated/recurrent: fluconazole 150mg every 72 hours × 3 doses, then weekly maintenance × 6 months.
Candidaemia and invasive candidiasis: Echinocandin first-line (caspofungin, micafungin, anidulafungin) — IDSA guidelines; step-down to fluconazole when clinically stable AND the isolate is fluconazole-susceptible AND blood cultures are negative. Remove central venous catheter. Duration: ≥14 days after last positive culture and symptom resolution.
Invasive aspergillosis: Voriconazole — first-line (IDSA 2016); superior to AmB (Walsh NEJM 2002). Primary alternative: isavuconazole or L-AmB. Duration: ≥6–12 weeks, depending on immunosuppression resolution. Galactomannan surveillance and CT halo sign monitoring guide response. Echinocandins (caspofungin) as salvage or combination therapy.
Mucormycosis (Rhizopus, Mucor, Lichtheimia): Liposomal amphotericin B (L-AmB) first-line — amphotericin B is the only established active agent (mucormycetes are intrinsically resistant to most azoles except posaconazole; voriconazole is NOT active vs Mucor — this is clinically important given its role in prophylaxis which may allow Mucor breakthrough). Posaconazole or isavuconazole as step-down or combination. Surgical debridement essential. Correct the underlying predisposing factor (diabetes, corticosteroids).
Cryptococcal meningitis: AmB (conventional or L-AmB) + 5-FC × 2 weeks (induction) → fluconazole 400mg/day × 8 weeks (consolidation) → fluconazole 200mg/day (maintenance until CD4 >200 on ART). Crucial adjunct: therapeutic lumbar puncture (repeated LP) to control raised intracranial pressure — ICP management is as important as antifungal therapy in preventing morbidity.
Dermatophytosis (tinea): Terbinafine topical (cream) × 2–4 weeks for tinea pedis/corporis/cruris. Systemic terbinafine 250mg/day × 4–12 weeks for tinea capitis or extensive disease; × 12 weeks for toenail onychomycosis. Griseofulvin for tinea capitis in children (better paediatric evidence than terbinafine for this indication). Itraconazole as alternative for onychomycosis.
Prophylaxis in immunocompromised: Fluconazole (Candida prophylaxis in solid organ transplant, haematology); posaconazole (Aspergillus prophylaxis in AML/MDS on high-dose chemotherapy or HSCT — NEJM 2007 trial); voriconazole (HSCT — especially active against Aspergillus).
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
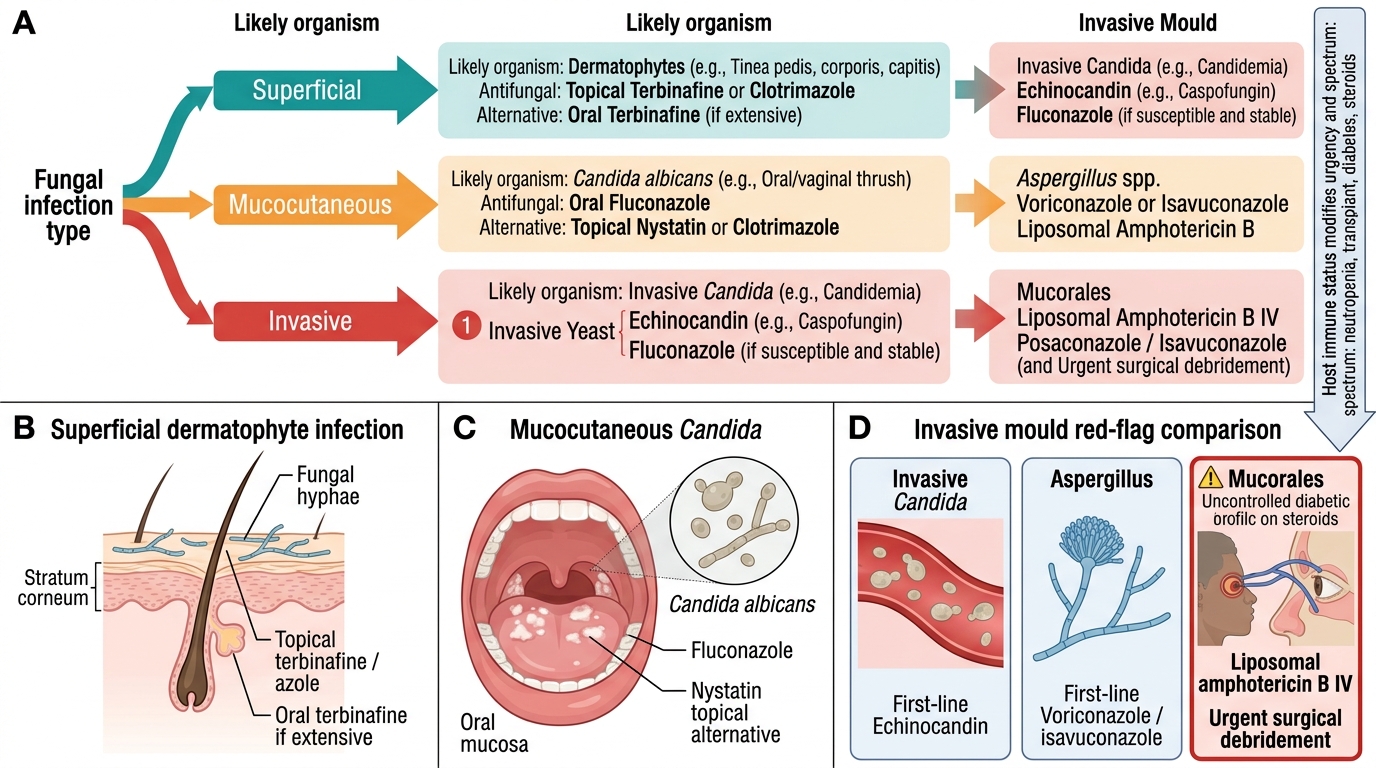
Algorithm for Antifungal Selection
SELF-CHECK
An uncontrolled diabetic patient (HbA1c 11%) with COVID-19 on systemic dexamethasone develops right orbital pain, facial swelling, and black nasal discharge 2 weeks into admission. MRI shows right orbital apex involvement. Mucormycosis is suspected. Which antifungal is first-line, and what is the key surgical intervention?
A. Voriconazole IV — first-line for all invasive mould infections in immunocompromised patients
B. Caspofungin IV — echinocandins cover Mucor as part of their broad mould spectrum
C. Liposomal amphotericin B (L-AmB) IV combined with urgent surgical debridement of necrotic tissue
D. Posaconazole oral — broadest azole spectrum including Mucor; surgical intervention not needed if started early
Reveal Answer
Answer: C. Liposomal amphotericin B (L-AmB) IV combined with urgent surgical debridement of necrotic tissue
Mucormycosis requires two simultaneous treatments: (1) L-AmB IV — the only reliably active antifungal agent against Mucorales (voriconazole is NOT active vs Mucor; echinocandins have minimal activity vs Mucorales; this is a critical clinical distinction — voriconazole prophylaxis can allow Mucor breakthrough). Posaconazole or isavuconazole are alternatives/step-down. (2) Urgent surgical debridement of all necrotic tissue — fungi invade blood vessels causing thrombosis and infarction; antifungals alone cannot penetrate avascular necrotic tissue. Medical therapy alone without debridement has high mortality. Additionally: correct the predisposing factors — stop corticosteroids if possible, control hyperglycaemia aggressively.
CLINICAL PEARL
Voriconazole's spectrum trap: Aspergillus YES, Mucor NO. Voriconazole is first-line for invasive aspergillosis and is used as prophylaxis in many haematology units. However, voriconazole has NO activity against Mucorales (Mucor, Rhizopus, Lichtheimia). In units using voriconazole prophylaxis, mucormycosis has emerged as a 'breakthrough' infection because voriconazole selectively eliminates Aspergillus competition while leaving Mucor unchallenged. The clinical consequence: a neutropenic patient on voriconazole prophylaxis who develops fever and sinus/orbital signs should be evaluated urgently for mucormycosis, not just assessed for voriconazole treatment failure. Treatment switch to L-AmB is urgent in that scenario.