Page 28 of 46
PH8.9 | PH8.9 | Anthelmintic Drugs — SDL Guide — SDL Guide
Learning Objectives
- Discuss the types, kinetics, dynamics, and adverse effects of drugs used for intestinal helminthiasis
- Select appropriate anthelmintic drugs for common helminth infections encountered in India
- Apply drug class knowledge to clinical scenarios including hookworm anaemia, neurocysticercosis, and schistosomiasis
INSTRUCTIONS
Soil-transmitted helminths (Ascaris lumbricoides, Trichuris trichiura, hookworm species) infect over 600 million people in India, primarily affecting children and contributing to iron-deficiency anaemia, malnutrition, and impaired cognitive development. Neurocysticercosis (Taenia solium) is the most common cause of acquired epilepsy in developing countries. Schistosomiasis, though not endemic in India, is important for travelers and the global picture. This SDL covers the key anthelmintic drug classes — their mechanisms, spectra, and clinical applications.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 65 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 64 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-year-old girl is brought to the paediatric OPD in rural Rajasthan with severe anaemia (Hb 6g/dL), poor growth, and passing pale stools. Her mother reports seeing worms in the stool. Stool examination shows hookworm eggs (Ancylostoma duodenale) and Ascaris lumbricoides eggs. She is also found to have an Enterobius vermicularis infection (perianal pruritus at night). The attending prescribes albendazole 400mg single dose with a plan for iron supplementation and protein-calorie support. Is this the right drug? Does a single dose cover all three worms? And what about the family — Enterobius is highly contagious within households?
WHY THIS MATTERS
Intestinal helminthiasis is among the most prevalent conditions you will treat in community practice, rural postings, and paediatric clinics across India. The WHO preventive chemotherapy programme administers annual single-dose albendazole or mebendazole to over 200 million school-age children in India. In clinical practice, the key pharmacological competency is knowing which drug covers which worm (some anthelmintics are broad-spectrum; others are narrow), the dosing, and the special considerations for pregnancy, organ involvement, and drug interactions.
RECALL
From microbiology: helminths are multicellular organisms (roundworms = nematodes; flatworms = cestodes/trematodes) with a complex neuromuscular system. Unlike bacteria and fungi, helminths do NOT divide rapidly in the human host — their pathology is from direct tissue damage (hookworm blood-sucking = iron-deficiency anaemia), immune-mediated responses (Ascaris eosinophilia), mechanical obstruction (heavy Ascaris loads), or tissue migration (larva migrans). The absence of rapid cell division means antibiotics and antifungals are useless; drugs must target the helminth's neuromuscular system or unique metabolic pathways. From the filariasis SDL: ivermectin — glutamate-gated chloride channels in invertebrates (absent in mammals); albendazole — beta-tubulin inhibitor; both used in WHO MDA for lymphatic filariasis.
Helminthic Disease Burden and Pathophysiology
Helminths are evolutionarily ancient multicellular parasites that have co-evolved with human hosts over millennia. Their pharmacological challenge is distinct from bacteria and fungi: they are much larger, do not divide rapidly in the human host (making antimitotic strategies less effective), and have immune-evasion mechanisms that allow them to survive for years to decades in a human host.
Why helminths are pharmacologically different:
- Multicellular organisms with complex organ systems — muscles, nervous system, reproductive system, cuticle — provide more diverse drug targets than single-celled pathogens.
- No rapid cell division in the adult stage (unlike bacteria or cancer cells) — drugs that target cell division (like β-lactams, which target peptidoglycan synthesis) are irrelevant. Instead, the most productive targets are the neuromuscular system (paralysis → expulsion) and unique metabolic processes (glucose uptake; oxidative phosphorylation).
- Immune evasion — helminth survival strategies include shedding surface antigens, releasing immunosuppressive molecules, and inhabiting protected niches (intracellular: Trichinella in muscle; subcutaneous: filariae; intestinal lumen with mucus coating: Ascaris).
Indian helminth burden (key species):
- Ascaris lumbricoides (roundworm): ~230 million infected in India; transmission via faecally contaminated soil/vegetables (embryonated eggs ingested → hepatic migration → lung migration → Löffler's syndrome eosinophilic pneumonitis → swallowed → adult intestinal worm); adult worms: 20–35cm, live 1–2 years; iron-deficiency and protein malnutrition.
- Hookworm (Ancylostoma duodenale): Skin penetration (walking barefoot on contaminated soil); larvae migrate to lungs (similar to Ascaris) → gut; adults attach to duodenal/jejunal mucosa → blood-sucking (0.03–0.15mL/worm/day) → iron-deficiency anaemia (the clinical signature of hookworm).
- Trichuris trichiura (whipworm): Caecal and colonic inhabitant; heavy infection → colitis, rectal prolapse in children.
- Enterobius vermicularis (pinworm/threadworm): Perianal pruritus at night (when female migrates to lay eggs); highly contagious within households via faecal-oral + retrograde autoinfection.
- Strongyloides stercoralis: Unique — can complete its lifecycle within the human host (autoinfection → hyperinfection in immunocompromised → disseminated strongyloidiasis with sepsis from enteric bacteria).
- Taenia solium (pork tapeworm): Taeniasis (intestinal adult worm, clinically benign); neurocysticercosis (larval cysts = cysticerci in brain → the leading cause of acquired epilepsy in developing countries; treated with albendazole + steroids).
Therapeutic Goal: Paralysis, Metabolic Disruption, and Expulsion
The therapeutic goals for helminthic infections reflect three pharmacological strategies, each exploiting a different biological vulnerability:
Strategy 1 — Neuromuscular paralysis and expulsion: The worm's neuromuscular system provides selective toxicity targets because helminth neurons differ from mammalian neurons in receptor types. Drugs that cause spastic paralysis (sustained depolarisation) or flaccid paralysis (hyperpolarisation) render the worm unable to maintain its position in the gut → normal peristalsis expels the paralysed worm. Examples: pyrantel (spastic paralysis via cholinergic nicotinic receptor activation); ivermectin (flaccid paralysis via glutamate-gated Cl⁻ channel activation); piperazine (flaccid paralysis via GABA-receptor activation).
Strategy 2 — Metabolic disruption (glucose uptake / microtubule function): Helminth survival depends on aerobic glycolysis (glucose uptake from the intestinal lumen) and normal microtubule function (for cellular transport, secretion, cell division in the larval stages). Benzimidazoles (albendazole, mebendazole) bind to β-tubulin of helminths (selectivity over mammalian tubulin exploits structural differences in the colchicine binding site) → inhibit microtubule polymerisation → impaired glucose uptake, cellular transport, secretory processes, and larval development → worm death (slower killing than neuromuscular agents — egg counts may fall before worm death; clinical improvement may take days).
Strategy 3 — Membrane disruption and immune attack: Praziquantel increases Ca²⁺ permeability of the schistosome and tapeworm tegument (outer membrane) → sustained muscle contraction (spastic paralysis) → disruption of the tegument → exposure of tegumental antigens to the host immune system → immune-mediated worm death. The host immune system is an essential partner in praziquantel's action — praziquantel is less effective in immunocompromised patients.
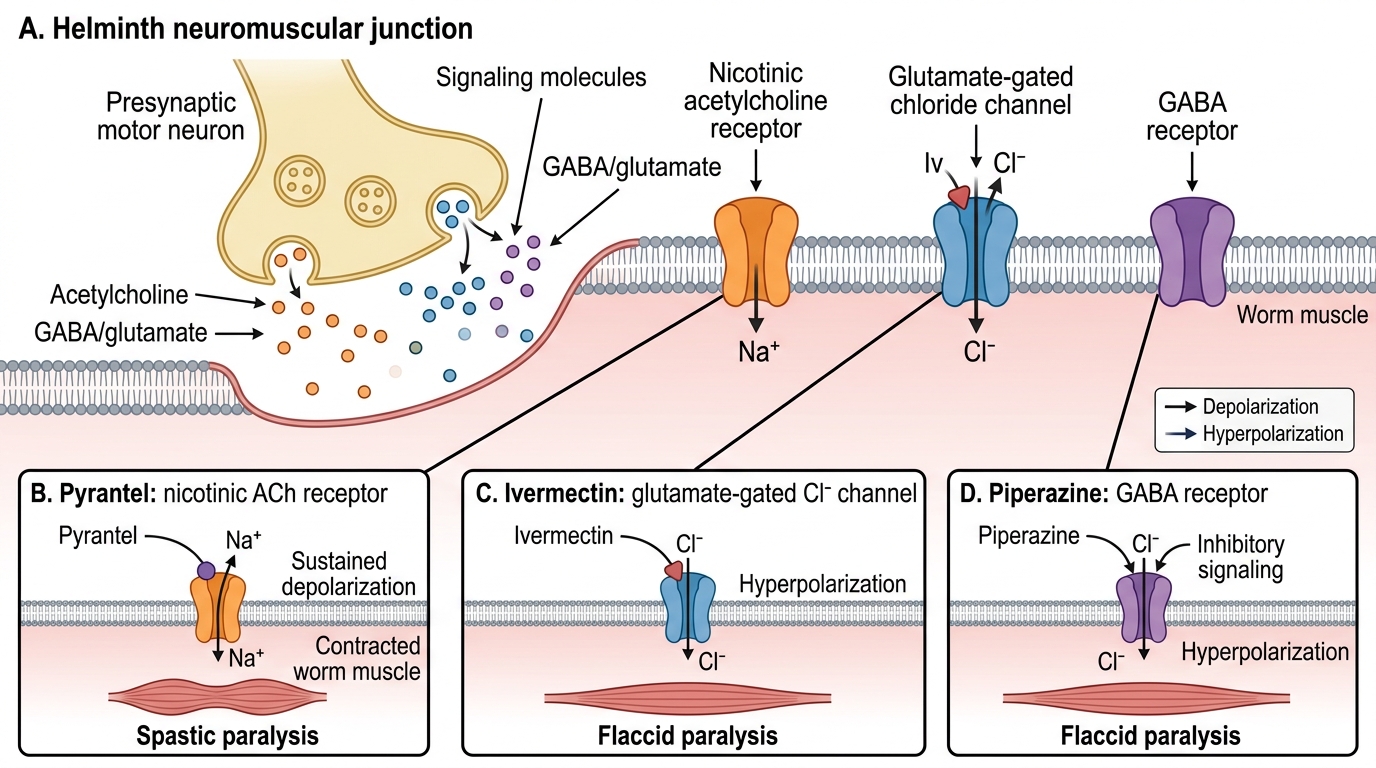
Anthelmintic Drug Targets at the Helminth Neuromuscular Junction
Classification of Anthelmintic Drugs
Anthelmintic drugs can be classified by their primary mechanism of action:
Provided image
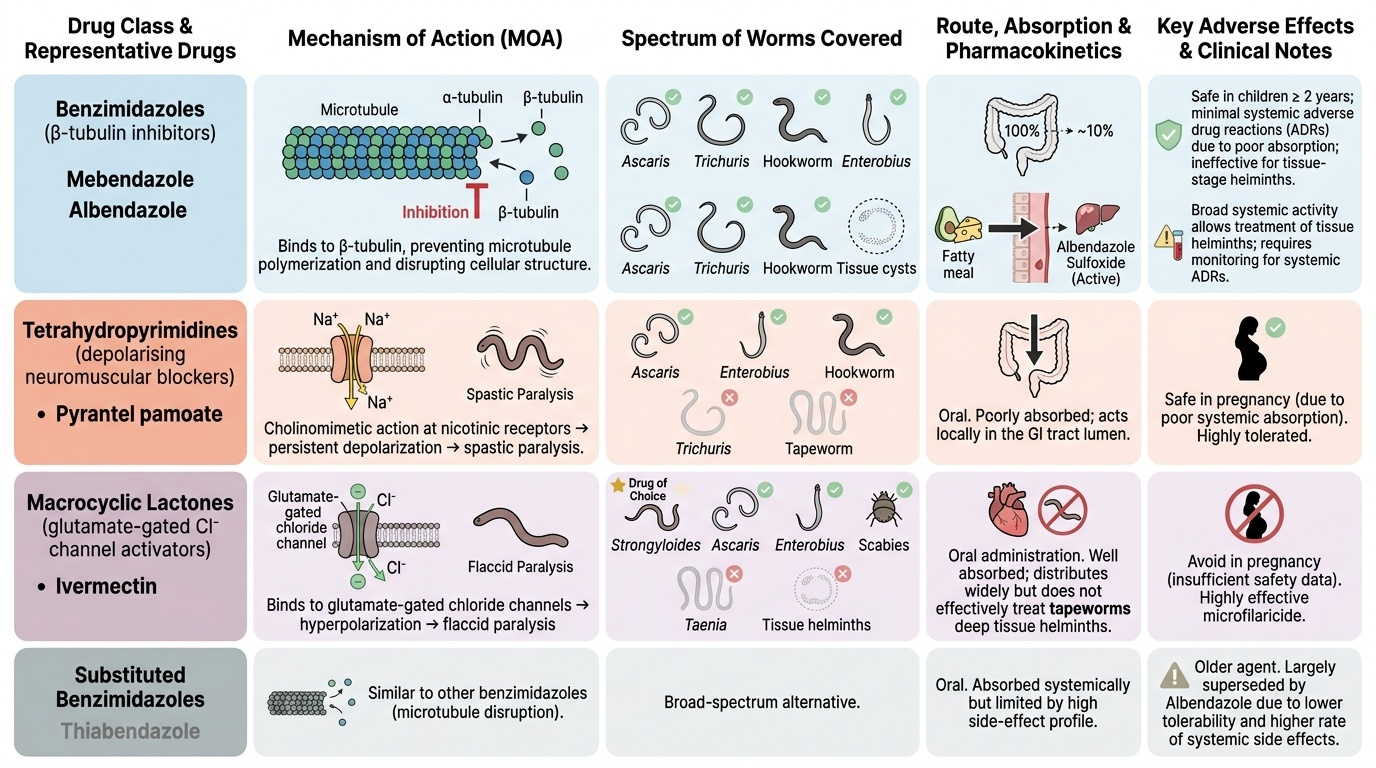
Benzimidazoles (β-tubulin inhibitors):
- Mebendazole — poorly absorbed from GI tract (~10% absorbed); very high luminal concentrations; local gut action; effective against Ascaris, Trichuris, hookworm, Enterobius. Safe in children >2 years. Poor systemic activity (advantage for intestinal helminths — minimal ADRs; disadvantage — cannot treat tissue helminths).
- Albendazole — better absorbed (especially with fatty meal, due to lipophilicity) → systemic activity → can reach tissue helminths; requires hepatic activation to albendazole sulfoxide (active metabolite). Broad-spectrum intestinal + tissue activity.
Tetrahydropyrimidines (depolarising neuromuscular blocking agents):
- Pyrantel pamoate — poorly absorbed; luminal action; cholinomimetic at nicotinic receptors of worm neuromuscular junction → sustained depolarisation → spastic paralysis. Covers Ascaris, Enterobius, hookworm. Safe in pregnancy (poorly absorbed). NOT effective vs Trichuris (different neuromuscular receptor sensitivity).
Macrocyclic lactones (glutamate-gated chloride channel activators):
- Ivermectin — binds invertebrate-specific glutamate-gated chloride channels → hyperpolarisation → flaccid paralysis. Active vs strongyloides (drug of choice for strongyloides — both intestinal and disseminated), Ascaris, Enterobius, filariae (microfilaricidal), scabies, lice. Avoid in pregnancy (insufficient safety data). Not for Taenia tapeworms or tissue helminths.
Substituted benzimidazole — broad-spectrum alternative:
- Thiabendazole — older, largely superseded by albendazole; still used in some settings for strongyloides.
Tetrahydropyrimidine derivatives / amidine compounds:
- Piperazine — GABA receptor agonist → hyperpolarisation → flaccid paralysis; mainly for Ascaris (round worm) and Enterobius; largely superseded by albendazole in most settings; safe in pregnancy; interaction risk with phenothiazines (mutual antagonism).
For tapeworms and trematodes:
- Praziquantel — Ca²⁺ channel activation → tegument disruption → immune-mediated death; drug of choice for schistosomiasis, neurocysticercosis (Taenia solium cysts in brain), taeniasis, liver flukes (Clonorchis, Fasciola — though Fasciola is resistant to praziquantel; use triclabendazole).
- Niclosamide — uncouples oxidative phosphorylation in tapeworm mitochondria → worm death; very poorly absorbed (intestinal action only); for taeniasis (intestinal tapeworm Taenia saginata/solium). Note: niclosamide is NOT appropriate for neurocysticercosis (poorly absorbed — cannot reach brain cysts). Must not be used for Taenia solium if there is risk of autoinfection/neurocysticercosis — kill of intestinal tapeworm may release viable eggs.