Page 29 of 46
PH8.9 | PH8.9 | Anthelmintic Drugs — SDL Guide — SDL Guide (Part 2)
Benzimidazoles, Pyrantel, and Ivermectin: Mechanisms and Uses
Albendazole — the workhorse of modern anthelmintic therapy:
- Mechanism: binds selectively to the colchicine-binding site on helminth β-tubulin (lower affinity for mammalian tubulin — selectivity basis) → inhibits tubulin polymerisation → disrupts microtubule formation → impairs: (a) cytoskeletal integrity, (b) vesicular transport (secretory functions, glucose transporter localisation), (c) cellular division in larval stages. Result: slow worm starvation and death (over 1–3 days for adult worms).
- Spectrum: Intestinal: Ascaris, hookworm (Ancylostoma + Necator), Enterobius, Trichuris, Strongyloides. Tissue: hydatid (Echinococcus — cysticidal in combination with surgery/aspiration), neurocysticercosis (Taenia solium cysts), toxocariasis (visceral larva migrans), cutaneous larva migrans.
- PK: lipophilic, poorly water-soluble; absorption increased 3–5× when taken with a fatty meal (important counselling point: 'take with food'). Hepatic first-pass activation to albendazole sulfoxide (the active metabolite — achieves therapeutic systemic concentrations); further oxidised to inactive sulfone. Eliminated renally.
- ADRs for single-dose intestinal use: minimal — transient GI discomfort (nausea, diarrhoea), headache. ADRs for prolonged-dose tissue use (hydatid, neurocysticercosis): hepatotoxicity (monitor LFTs at baseline and every 2 weeks during prolonged cycles); alopecia (reversible, common); bone marrow suppression (leukopenia — check CBC). Teratogenic (animal studies) — avoid in first trimester and ideally throughout pregnancy; safe alternatives exist (pyrantel, mebendazole for intestinal use).
- Standard intestinal dose: 400mg single dose (adults and children ≥2 years); for Enterobius, repeat at 2 weeks (and treat all household members — reinfection from perianal eggs otherwise guaranteed).
Mebendazole:
- Same mechanism as albendazole (β-tubulin). Key PK difference: very poorly absorbed (~10%) — acts primarily in the gut lumen. This means: excellent gut luminal concentrations with minimal systemic exposure → excellent safety for intestinal helminths; but inadequate plasma levels for tissue helminths (hydatid, neurocysticercosis). Dose: 100mg BD × 3 days for Trichuris, hookworm, Ascaris; 100mg single dose for Enterobius (repeat at 2 weeks).
Pyrantel pamoate:
- Mechanism: depolarising neuromuscular blocking agent — acts at the acetylcholine nicotinic receptors on helminth muscle, causing sustained muscle depolarisation → spastic paralysis → worm cannot maintain intestinal position → expelled by peristalsis. Poorly absorbed (99% luminal action) — minimal systemic effects.
- Spectrum: Ascaris, Enterobius, hookworm. NOT Trichuris (Trichuris neuromuscular receptors less sensitive to pyrantel; mebendazole/albendazole preferred).
- Dose: 10mg/kg single dose (base); maximum 1g. Suitable for children from any age and in pregnancy (SAFE — not absorbed systemically).
- ADRs: minimal; transient nausea, abdominal cramps. Interaction with piperazine: antagonistic (both act on worm NMJ but via different/opposing receptors — use one or the other, not both).
Ivermectin:
- Mechanism: activates glutamate-gated chloride (GluCl) ion channels in invertebrate neurons and muscle membranes → sustained chloride ion influx → membrane hyperpolarisation → flaccid paralysis → worm death. GluCl channels are absent in mammals (invertebrate-specific) — the basis of selective toxicity. (Note: ivermectin can penetrate the mammalian CNS in large doses or when P-glycoprotein — the blood-brain barrier pump — is absent; this explains toxicity in certain dog breeds with MDR1/ABCB1 mutation).
- Spectrum: Strongyloides stercoralis (drug of choice; single dose 200mcg/kg — also prevents hyperinfection syndrome in immunocompromised); filarial microfilariae (MDA); Ascaris; Enterobius; cutaneous larva migrans; scabies (oral); head lice.
- Avoid in pregnancy (limited safety data; teratogenic in animals). Avoid in children <15kg. Mazzotti-like reaction in heavily filarial-infected patients (from dying microfilariae).
SELF-CHECK
A 7-year-old child presents with perianal pruritus at night. Scotch-tape test shows Enterobius vermicularis eggs. The whole family (2 adults, 3 children) lives in the same room. What is the most appropriate management?
A. Treat the child only with albendazole 400mg single dose — not necessary to treat asymptomatic family members
B. Treat all family members with albendazole 400mg single dose; repeat the dose for all in 2 weeks; implement hand-washing and linen hygiene measures
C. Use mebendazole 500mg BD × 3 days for the child only — a longer course is needed for Enterobius
D. Treat with pyrantel pamoate for the child only — safe for school-age children; adults do not need treatment
Reveal Answer
Answer: B. Treat all family members with albendazole 400mg single dose; repeat the dose for all in 2 weeks; implement hand-washing and linen hygiene measures
Enterobius vermicularis is highly contagious within households: the female migrates to the perianal skin at night to lay eggs (thousands of eggs per laying), eggs survive on surfaces for up to 3 weeks, and autoinfection is common (hand-to-mouth). All household members should be treated simultaneously to prevent ping-pong reinfection. Albendazole 400mg single dose (or mebendazole 100mg single dose) is given to all household members, and the dose is repeated at 2 weeks (to cover re-infection from environmental eggs and autoinfection cycle). Hygiene measures (washing hands, laundering bedlinen and underwear daily, showering in the morning) are essential adjuncts. Treating the index patient alone while leaving infected household members guarantees reinfection.
Praziquantel, Niclosamide, and Other Anthelmintics
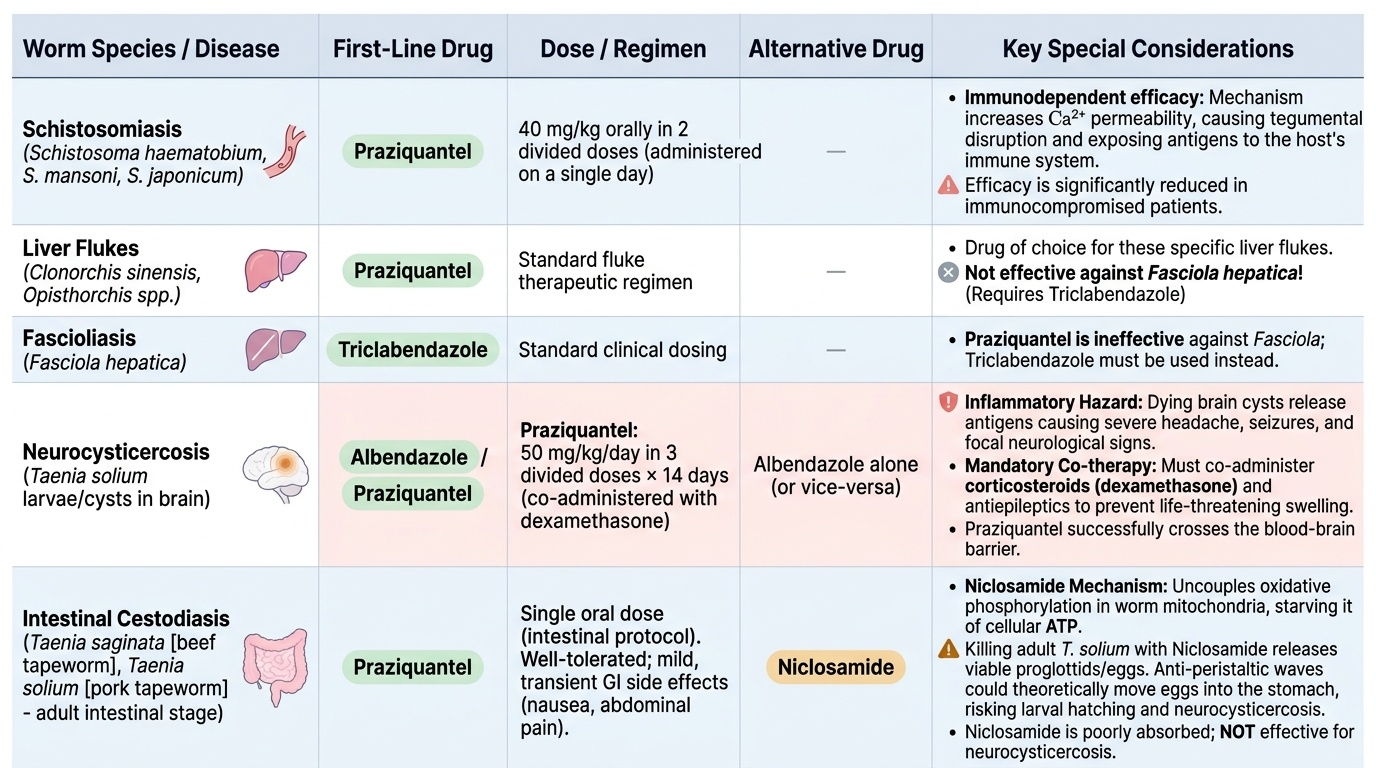
Praziquantel — broad-spectrum for trematodes and cestodes:
- Mechanism: Praziquantel increases calcium permeability of the worm's tegument (outer surface) → massive influx of Ca²⁺ → sustained tetanic muscular contraction (spastic paralysis) → disruption of the tegument surface → exposes tegumental antigens to the host immune system → immune-mediated attack kills the worm. Praziquantel thus harnesses the host's own immune response as part of its mechanism — explaining reduced efficacy in immunocompromised patients.
- Spectrum: Schistosoma spp. (all major species: S. haematobium, S. mansoni, S. japonicum) — drug of choice; Taenia spp. (intestinal tapeworm — T. saginata, T. solium); Neurocysticercosis (T. solium cysts in brain — alternative to albendazole, both used); Liver flukes (Clonorchis sinensis, Opisthorchis — drug of choice; NOT Fasciola hepatica — praziquantel is largely ineffective vs Fasciola; use triclabendazole).
- PK: good oral absorption; significant first-pass metabolism; crosses blood-brain barrier (effective in neurocysticercosis).
- ADRs: well-tolerated for intestinal use; GI (nausea, diarrhoea, abdominal pain — common, transient). For neurocysticercosis: dying cysts release inflammatory antigens → severe headache, seizures, focal neurological signs — must co-administer corticosteroids (dexamethasone) and antiepileptics during praziquantel (or albendazole) treatment for neurocysticercosis. This inflammatory response can be life-threatening without steroid cover.
- Dose: schistosomiasis: 40mg/kg in 2 divided doses (single day); neurocysticercosis: 50mg/kg/day in 3 divided doses × 14 days (with dexamethasone).
Provided image
Niclosamide — for intestinal tapeworm:
- Mechanism: inhibits oxidative phosphorylation in tapeworm mitochondria (uncouples electron transport → tapeworm starves of ATP) AND stimulates ATPase activity → inadequate energy → tapeworm paralysis → disintegration/death.
- Spectrum: intestinal tapeworm (Taenia saginata [beef tapeworm] and Taenia solium [pork tapeworm] — intestinal forms). NOT for neurocysticercosis (very poorly absorbed → cannot reach brain cysts).
- Important caution for T. solium: killing the intestinal adult T. solium worm with niclosamide releases viable proglottids (that may contain eggs). There is a theoretical risk that antiperistaltic waves could move proglottids/eggs proximally, allowing autoinfection and neurocysticercosis development. Risk is low but real — some authorities prefer praziquantel (which also kills any cysticerci already present) over niclosamide for T. solium intestinal infection. However, niclosamide is widely used and the actual risk of this complication is considered low.
- ADRs: minimal (very poorly absorbed) — nausea, vomiting; well-tolerated.
Piperazine:
- Mechanism: GABA-receptor agonist on worm neuromuscular junction → hyperpolarisation → flaccid paralysis → worm expelled by peristalsis. Note: piperazine causes FLACCID paralysis (by hyperpolarisation), while pyrantel causes SPASTIC paralysis (by depolarisation). These mechanisms are antagonistic — never combine.
- Spectrum: Ascaris and Enterobius (limited spectrum; largely superseded by albendazole).
- Safe in pregnancy and young children. ADRs: GI; rare neurotoxicity at high doses.
SELF-CHECK
A 25-year-old man presents with seizures and headache. MRI brain shows multiple ring-enhancing lesions. CSF reveals mild lymphocytic pleocytosis. Serology for Taenia solium is positive. Neurocysticercosis is diagnosed. What is the pharmacotherapy plan?
A. Praziquantel alone — drug of choice for all tapeworm infections, no steroid needed
B. Niclosamide — effective for all forms of Taenia solium infection including CNS cysts
C. Albendazole 15mg/kg/day × 8–30 days with dexamethasone and antiepileptics; praziquantel is an alternative
D. Ivermectin single dose — covers all tissue helminths including neurocysticercosis
Reveal Answer
Answer: C. Albendazole 15mg/kg/day × 8–30 days with dexamethasone and antiepileptics; praziquantel is an alternative
Neurocysticercosis (T. solium cysts in the brain) requires treatment with albendazole (15mg/kg/day in 2 divided doses × 8–30 days, in cycles) OR praziquantel (50mg/kg/day × 14 days) — both are accepted first-line options; albendazole is preferred in most guidelines. Crucially, cysticidal therapy (killing cysts) triggers an intense inflammatory response from host immune attack on dying cyst antigens → worsening cerebral oedema, seizures, raised ICP. Corticosteroids (dexamethasone) MUST be co-administered to blunt this inflammatory response and prevent herniation. Antiepileptic drugs are used for seizure control. Niclosamide cannot reach brain cysts (not absorbed). Ivermectin covers intestinal nematodes and microfilariae but NOT Taenia or cysticerci.
Clinical Decision-Making: Drug Choice by Helminth
Provided image
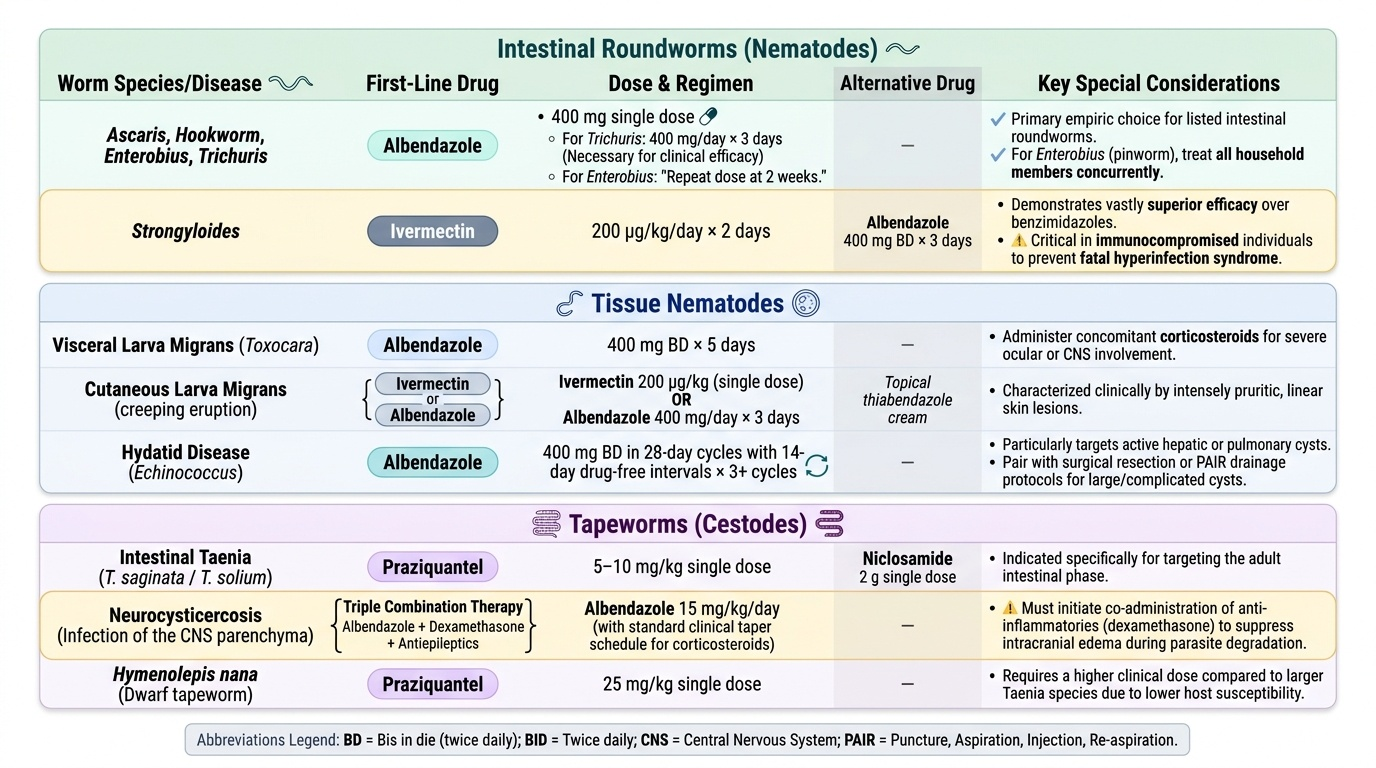
The clinical selection of anthelmintic drugs follows a straightforward algorithm based on the infecting organism and clinical context. The key discriminators are: (1) roundworm vs tapeworm vs fluke; (2) intestinal vs tissue location; (3) special populations (pregnancy, immunocompromised, children).
Roundworms (nematodes) — intestinal:
- Ascaris, hookworm, Enterobius, Trichuris: Albendazole 400mg single dose (first-line for all). For Trichuris: 400mg/day × 3 days (single dose less effective vs Trichuris). For Enterobius: repeat at 2 weeks; treat all household members.
- Strongyloides: Ivermectin 200mcg/kg/day × 2 days (drug of choice — far superior to albendazole; especially important in immunocompromised to prevent hyperinfection/disseminated strongyloidiasis).
Tissue nematodes:
- Visceral larva migrans (Toxocara): albendazole 400mg BD × 5 days ± steroids for severe ocular/CNS involvement.
- Cutaneous larva migrans (hookworm larva in skin): ivermectin 200mcg/kg single dose OR albendazole 400mg/day × 3 days (topical thiabendazole also effective).
- Hydatid disease (Echinococcus — cysts in liver/lungs): albendazole 400mg BD in 28-day cycles with 14-day drug-free intervals × 3+ cycles (surgery/PAIR drainage + albendazole for larger cysts).
Tapeworms (cestodes):
- Taenia saginata or T. solium (intestinal): praziquantel 5–10mg/kg single dose OR niclosamide 2g single dose.
- Neurocysticercosis (T. solium in brain): albendazole 15mg/kg/day + dexamethasone + antiepileptics (see above).
- Hymenolepis nana (dwarf tapeworm): praziquantel 25mg/kg single dose.
Trematodes (flukes):
- Schistosomiasis: praziquantel 40mg/kg in 2 divided doses (single day).
- Fasciola hepatica (sheep liver fluke): triclabendazole (praziquantel NOT effective vs Fasciola — common exam and clinical pitfall).
- Opisthorchis/Clonorchis (fish liver flukes): praziquantel.
Special populations:
- Pregnancy: pyrantel pamoate (safe — not absorbed) or mebendazole (local gut action, minimal systemic exposure) for intestinal roundworms. Avoid albendazole (1st trimester teratogenicity risk), ivermectin (limited data), praziquantel (1st trimester caution).
- Immunocompromised with suspected strongyloides: ivermectin urgently — disseminated strongyloidiasis is potentially fatal if untreated; hyperinfection with albendazole alone may progress despite treatment.