Page 2 of 36
PH7.1 | PH7.1 | Diabetes Mellitus Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Non-Insulin Oral Agents: Mechanisms, PK, and ADRs
Non-insulin oral agents target different nodes of the pathophysiological web, and their classification by mechanism is essential for rational combination therapy and avoiding redundancy.
Biguanides — Metformin: Metformin is the universal first-line agent for T2DM. Its primary mechanism is inhibition of hepatic gluconeogenesis via activation of AMP-activated protein kinase (AMPK) and inhibition of mitochondrial complex I, reducing hepatic glucose output by up to 30%. Secondary effects include enhanced peripheral glucose uptake and reduced intestinal glucose absorption. It does NOT stimulate insulin secretion — no hypoglycaemia risk when used alone. Weight is neutral or slightly reduced. Key ADRs: GI intolerance (nausea, diarrhoea — start low, take with food), rare but serious lactic acidosis (contraindicated when eGFR <30, in hepatic failure, alcoholism, contrast media exposure). Dose reduce when eGFR 30–45.
Sulfonylureas (SU): Bind and close ATP-sensitive K⁺ (KATP) channels on pancreatic β-cells → membrane depolarisation → Ca²⁺ influx → insulin release. Entirely dependent on residual β-cell function. 1st generation (tolbutamide, chlorpropamide, tolazamide) — shorter acting (tolbutamide) to very long-acting (chlorpropamide, t½ 36 hr) — now rarely used. 2nd generation (glibenclamide/glyburide, glipizide, gliclazide, glimepiride) — more potent, shorter duration, better tolerated. Gliclazide is widely used in India (modified-release, lower hypoglycaemia risk). Glimepiride is a 2nd-generation SU (not 3rd-gen). Main ADRs: hypoglycaemia (most significant — especially glibenclamide, longest-acting 2nd-gen SU), weight gain (1–4 kg), chlorpropamide: SIADH, disulfiram reaction with alcohol.
Meglitinides (Glinides): Repaglinide and nateglinide bind the SUR1 subunit at a different site from SUs, causing rapid, short-duration insulin release — taken with each meal (postprandial glucose control). Lower hypoglycaemia risk than SUs (shorter action). Useful in irregular meal patterns.
DPP-4 Inhibitors (Gliptins): Sitagliptin, vildagliptin, saxagliptin, alogliptin inhibit dipeptidyl peptidase-4, the enzyme that degrades endogenous GLP-1 and GIP. Net effect: prolonged incretin activity → glucose-dependent insulin release, glucagon suppression. Weight-neutral. Very low hypoglycaemia risk (glucose-dependent). Renal dose adjustment required (sitagliptin 50 mg eGFR 30–45; 25 mg eGFR <30). ADRs: nasopharyngitis, mild URI. Saxagliptin associated with increased HHF risk in SAVOR-TIMI trial (avoid in HF).
Thiazolidinediones (TZD) — Pioglitazone: Activates PPARγ (peroxisome proliferator-activated receptor gamma) nuclear receptors in adipose, muscle, and liver → enhanced insulin signalling and fat redistribution from visceral to subcutaneous. Takes weeks for full effect. ADRs: weight gain (2–5 kg), fluid retention → CONTRAINDICATED in HF, bladder cancer risk (pioglitazone, avoid if prior bladder cancer), osteoporotic fractures (especially in women). Hepatotoxicity: monitor LFTs (troglitazone was withdrawn; pioglitazone rare).
Alpha-glucosidase Inhibitors: Acarbose and voglibose competitively inhibit intestinal alpha-glucosidase enzymes, slowing carbohydrate hydrolysis and glucose absorption — reduces postprandial glucose spikes. No systemic absorption, no hypoglycaemia alone. ADRs: flatulence, bloating, diarrhoea (common, limits compliance). Useful in postprandial hyperglycaemia dominant cases.
| Drug Class | Mechanism | Key ADR | Renal Caution |
|---|---|---|---|
| Metformin | ↓ Hepatic glucose output (AMPK) | GI intolerance, lactic acidosis | Stop <eGFR 30, reduce 30–45 |
| Sulfonylureas (2nd-gen) | KATP channel closure → insulin↑ | Hypoglycaemia, weight gain | Caution; prefer gliclazide |
| Meglitinides | Rapid KATP closure (meal-time) | Hypoglycaemia (low) | Repaglinide hepatic |
| DPP-4 inhibitors | ↑ Incretin effect | Nasopharyngitis, URI | Dose-reduce in CKD |
| Pioglitazone (TZD) | PPARγ activation | Weight gain, fluid retention, HF risk | OK in CKD (no renal dose adj) |
| Acarbose/Voglibose | ↓ Carbohydrate absorption | Flatulence, bloating | Avoid severe renal impairment |
Injectable Non-Insulin Agents: GLP-1 RAs, Dual Agonists, SGLT2 Inhibitors
The newest drug classes in diabetes pharmacotherapy have shifted the therapeutic goal from glucose control alone to cardiovascular and renal risk reduction — arguably the most important paradigm shift in diabetes management in two decades.
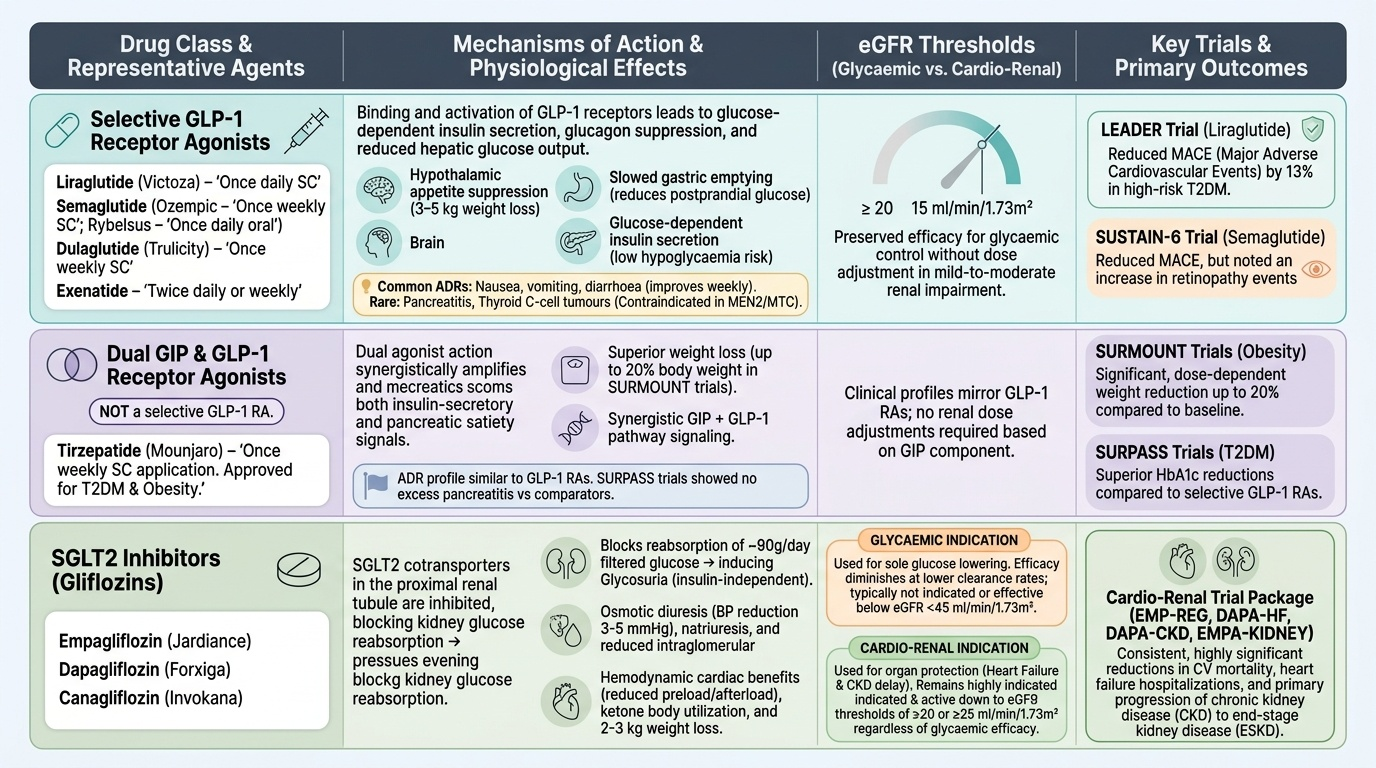
GLP-1 Receptor Agonists (GLP-1 RAs): Liraglutide (Victoza, once daily SC), semaglutide (Ozempic, once weekly SC; Rybelsus, once daily oral), dulaglutide (Trulicity, once weekly SC), exenatide (twice daily or weekly). These agents bind and activate the GLP-1 receptor, producing: glucose-dependent insulin secretion (low hypoglycaemia risk), glucagon suppression, slowed gastric emptying (reduces postprandial glucose), hypothalamic appetite suppression (weight loss 3–5 kg), reduced hepatic glucose output. They are selective GLP-1 agonists — NOT dual agonists. Major ADRs: nausea/vomiting/diarrhoea (most common, improve over weeks), rare pancreatitis and thyroid C-cell tumours (caution in personal/family history of MEN2 or medullary thyroid cancer). CV outcome data: LEADER trial — liraglutide reduced MACE by 13% in T2DM patients with high CV risk. SUSTAIN-6 — semaglutide reduced MACE but increased retinopathy events.
Dual GIP/GLP-1 Receptor Agonist — Tirzepatide: Tirzepatide (Mounjaro) is a dual agonist of both GIP and GLP-1 receptors — it is NOT a selective GLP-1 RA. This distinction is critical: dual receptor action drives greater weight loss (up to 20% body weight in SURMOUNT trials) and superior HbA1c reduction compared to selective GLP-1 RAs. Approved for T2DM and obesity. The dual mechanism amplifies both insulin-secretory and satiety signals synergistically. ADR profile similar to GLP-1 RAs; no excess pancreatitis vs comparators in SURPASS trials.
SGLT2 Inhibitors (Gliflozins): Empagliflozin (Jardiance), dapagliflozin (Forxiga), canagliflozin (Invokana) inhibit sodium-glucose cotransporter 2 (SGLT2) in the proximal renal tubule, blocking reabsorption of ~90 g/day of filtered glucose → glycosuria (independent of insulin). Additional effects: osmotic diuresis (BP reduction), natriuresis, reduced intraglomerular pressure (reno-protective), haemodynamic cardiac benefits (reduced preload/afterload, ketone body utilisation). Weight loss 2–3 kg, BP reduction 3–5 mmHg.
Critical eGFR threshold distinction:
- Glycaemic indication (glucose lowering alone): not recommended below eGFR ~45 (insufficient tubular SGLT2 to drive meaningful glycosuria)
- Cardio-renal indication (HF, CKD): benefit continues down to eGFR ~20 (drug-specific) — driven by haemodynamic/renal mechanisms independent of glucose lowering
ADRs: genital mycotic infections (most common — urinary glycosuria promotes fungal growth), UTIs, euglycaemic DKA (perioperative, sick-day rule: STOP 3 days before surgery), Fournier's gangrene (rare, severe), volume depletion, canagliflozin: lower limb amputation risk (CANVAS). Key CV/renal trial data:
Provided image
CLINICAL PEARL
Prescribing SGLT2 inhibitors requires knowing TWO eGFR thresholds, not one. For purely glycaemic benefit: avoid below eGFR ~45 (insufficient tubular SGLT2). For cardio-renal benefit (HFrEF, CKD, albuminuria): continue down to eGFR ~20 — the haemodynamic and anti-inflammatory mechanisms work even when the kidney can no longer spill glucose. The DAPA-CKD trial demonstrated dapagliflozin's renal benefits even in non-diabetic CKD patients. Similarly, recall that tirzepatide ≠ semaglutide mechanistically — tirzepatide is the only approved DUAL GIP/GLP-1 agonist; semaglutide is a selective GLP-1 RA. In a clinical viva or prescription, conflating these is a factual error.
SELF-CHECK
Which of the following statements about SGLT2 inhibitors is CORRECT regarding eGFR thresholds?
A. A. They should be stopped at eGFR <45 for ALL indications
B. B. For glycaemic benefit, avoid below eGFR ~45; for cardio-renal benefit, can continue to eGFR ~20
C. C. They are safe at any eGFR and require no dose adjustment
D. D. They are contraindicated below eGFR 60
Reveal Answer
Answer: B. B. For glycaemic benefit, avoid below eGFR ~45; for cardio-renal benefit, can continue to eGFR ~20
SGLT2 inhibitors have TWO distinct eGFR thresholds depending on indication. The glycaemic benefit relies on tubular glucose loading — reduced below eGFR ~45. The cardio-renal benefit (HF, CKD) is mediated by haemodynamic and anti-inflammatory mechanisms — continues to eGFR ~20 (drug-specific). Option A incorrectly applies the glycaemic threshold universally. Option C is dangerously wrong. Option D is too conservative even for glycaemic use.
Clinical Decision-Making: Matching Drug to Patient
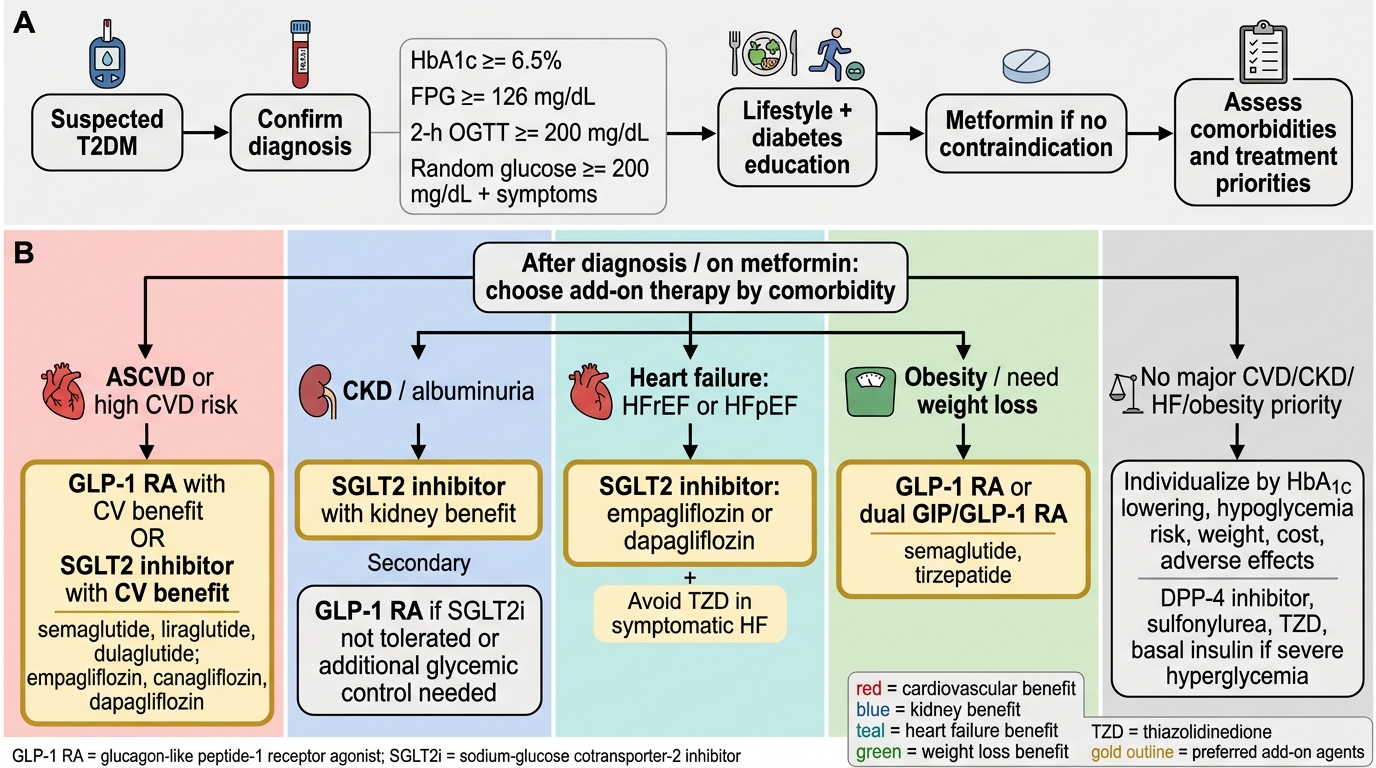
Pharmacological management of T2DM is stepwise and patient-centred, moving from monotherapy toward combination therapy as β-cell function declines and HbA1c targets are missed. The ADA/EASD 2023 framework, which aligns with NMC PH7.1 competency requirements, provides the following decision logic:
Step 1 — Metformin as universal first-line (unless contraindicated: eGFR <30, contrast procedure, hepatic failure, alcoholism). Start 500 mg OD with evening meal; uptitrate to 2000–2500 mg/day. Counsel on GI side effects; extended-release reduces them.
Step 2 — Patient-stratified add-on therapy. Once metformin is at maximum tolerated dose and HbA1c remains >7%:
- Established CVD or high CV risk: add GLP-1 RA (liraglutide, semaglutide) or SGLT2i — both have mortality benefit proven in RCTs. LEADER (liraglutide), SUSTAIN-6 (semaglutide), EMPA-REG (empagliflozin), CANVAS (canagliflozin) — choose based on HF status, weight, route preference.
- Heart failure (HFrEF, LVEF <40%): SGLT2i is the agent of choice — empagliflozin and dapagliflozin have the strongest HF-specific outcome data (EMPEROR-Reduced, DAPA-HF). AVOID pioglitazone (worsens fluid retention/HF). Saxagliptin — AVOID (SAVOR-TIMI: HHF risk).
- CKD (eGFR 20–60): SGLT2i (cardio-renal dose, continue to eGFR ~20) reduces albuminuria and CKD progression (CREDENCE, DAPA-CKD). Metformin stop <eGFR 30. DPP-4i (dose-adjusted) are renal-safe.
- Obesity/weight reduction priority: GLP-1 RA > tirzepatide (dual GIP/GLP-1) > SGLT2i. Avoid SU, insulin (weight-gaining).
- Hypoglycaemia risk (elderly, solo drivers, irregular meals): DPP-4i, GLP-1 RA, SGLT2i (glucose-dependent/independent mechanisms — low intrinsic hypoglycaemia risk). Avoid SU monotherapy in vulnerable patients.
- Cost-constrained patients: Metformin + gliclazide/glipizide (generic, affordable). Counsel on hypoglycaemia risk and sick-day rules.
Prevention of complications: Tight glycaemic control (HbA1c <7%) reduces microvascular complications (DCCT, UKPDS). For macrovascular prevention: choose SGLT2i/GLP-1 RA for demonstrated CV mortality reduction. ACE inhibitor/ARB for nephropathy regardless of BP. Annual retinal screening, foot examination, creatinine/eGFR monitoring is standard practice.
Obese patient management principle: Drugs that lower weight ALSO reduce insulin resistance — a virtuous cycle. Sequencing: metformin → GLP-1 RA or SGLT2i → tirzepatide if needed. Reserve SU and insulin for cases where other options are ineffective, unavailable, or contraindicated.
T2DM Pharmacotherapy Selection Algorithm