Page 5 of 36
PH7.2 | PH7.2 | Osteoporosis Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Classify anti-osteoporotic drugs into anti-resorptive and anabolic categories with specific examples
- Describe the pharmacokinetics, pharmacodynamics, and adverse effects of bisphosphonates, denosumab, teriparatide, and SERMs
- Devise an evidence-based management plan for postmenopausal female and male osteoporosis patients
- Apply renal function thresholds to select appropriate drugs in patients with CKD
- Justify drug sequencing from anti-resorptive to anabolic agents based on fracture severity
INSTRUCTIONS
Osteoporosis is a silent disease until a fracture occurs — and the first hip fracture in an elderly patient carries a one-year mortality of 20–30%. With India's ageing population and widespread vitamin D deficiency, pharmacological fracture prevention is a major public health concern. This guide covers the full pharmacological arsenal from the familiar bisphosphonates to the newer anabolic agents, and equips you to tailor management to both female and male patients.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 20 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 46 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old postmenopausal woman presents after a fall at home with acute back pain. Vertebral X-ray reveals a crush fracture of L2. Her DEXA scan shows T-score –3.2 at the lumbar spine, and her creatinine gives an eGFR of 32 mL/min/1.73m². She has been taking calcium and vitamin D tablets for five years, believing they are 'bone medicine.' You need to prescribe a drug that actually prevents her next fracture — and her renal function limits some options. Can you choose the right agent, counsel her on the administration technique, and monitor for the significant ADRs of her treatment?
WHY THIS MATTERS
Osteoporotic fractures are the third leading cause of disability-adjusted life years in elderly women worldwide. Hip fractures specifically carry 20–30% mortality in the first year and impose enormous loss of independence. Despite effective pharmacotherapy — bisphosphonates reduce vertebral fractures by 40–70% — osteoporosis remains widely undertreated because of its asymptomatic nature and patient misconceptions about treatment (e.g. calcium alone is sufficient). As a future clinician, understanding the mechanism, evidence, and practical limitations of each drug class is essential to offering fracture-preventive care that makes a real difference.
RECALL
Bone is a dynamic tissue undergoing constant remodelling: osteoclasts (derived from haematopoietic precursors) resorb old bone, while osteoblasts (mesenchymal origin) deposit new bone matrix. In healthy adults, these are coupled — resorption and formation are balanced. The key regulatory pathway is RANK-L / RANK / OPG: osteoblasts secrete RANK-L (receptor activator of NF-κB ligand), which binds RANK on osteoclast precursors, activating osteoclastogenesis and osteoclast survival. Osteoprotegerin (OPG), also secreted by osteoblasts, acts as a decoy receptor for RANK-L — it sequesters RANK-L and thus inhibits osteoclast activation. Oestrogen upregulates OPG and downregulates RANK-L — so post-menopausal oestrogen loss tips the balance toward osteoclast dominance and net bone resorption. PTH in sustained elevation (as in hyperparathyroidism) also drives osteoclast activation — but brief, intermittent PTH pulses paradoxically stimulate osteoblasts (the basis of teriparatide therapy). Vitamin D is essential for intestinal calcium absorption; its deficiency worsens negative calcium balance and secondary hyperparathyroidism.
Bone Remodelling Imbalance: The Pathophysiology of Osteoporosis
Osteoporosis is defined as a systemic skeletal disease characterised by low bone mass and microarchitectural deterioration of bone tissue, leading to increased bone fragility and fracture risk. The WHO diagnostic criterion is a bone mineral density (BMD) T-score ≤ –2.5 at the hip or lumbar spine by DEXA (dual-energy X-ray absorptiometry). Osteopenia = T-score –1.0 to –2.5. T-score below –3.5 with fracture history defines severe osteoporosis.
The central pathophysiological event is an uncoupling of bone remodelling in favour of resorption over formation. In postmenopausal osteoporosis (most common), loss of oestrogen reduces OPG production and increases RANK-L secretion by osteoblasts — osteoclast activation is unrestrained. This leads to trabecular thinning (especially vertebral bodies) and cortical porosity (femoral neck). Male osteoporosis accounts for approximately 20% of cases and is commonly secondary — due to hypogonadism, glucocorticoid use, alcoholism, anticonvulsants, or chronic disease. Primary male osteoporosis is less common but occurs in ageing men as testosterone levels decline.
The sclerostin pathway provides an additional node targeted pharmacologically: sclerostin, secreted by osteocytes, inhibits Wnt/β-catenin signalling in osteoblasts — reducing osteoblast differentiation and bone formation. Romosozumab (anti-sclerostin antibody) blocks this inhibitor, releasing osteoblast activity while simultaneously (via indirect effects) reducing osteoclast activity — a dual anabolic/anti-resorptive mechanism unique among approved agents.
RANK-L/RANK/OPG Axis and Denosumab Action
Therapeutic Goals: Fracture Prevention in Female and Male Patients
The primary goal of osteoporosis pharmacotherapy is fracture prevention — not merely DEXA score improvement. The most clinically significant fractures are vertebral compression fractures (back pain, height loss, kyphosis), hip fractures (highest mortality: 20–30% at one year), and distal radius fractures. Non-vertebral fracture reduction is harder to demonstrate in RCTs (heterogeneous population) but is a goal for anabolic agents and some bisphosphonates.
Treatment initiation thresholds:
- T-score ≤ –2.5 with or without prior fracture
- T-score –1.0 to –2.5 (osteopenia range) plus FRAX 10-year fracture probability ≥20% (major) or ≥3% (hip) — guides treatment in 'borderline' cases
- Prior low-trauma fracture at any T-score — treat irrespective of DEXA
Beyond pharmacotherapy, all patients need calcium 1000–1200 mg/day (dietary preferred; supplement if dietary intake insufficient) and vitamin D 800–1000 IU/day — these are adjuncts, not primary therapy. Fall prevention (exercise, home hazard assessment, vision correction, medication review) is equally important.
Duration considerations: Bisphosphonates may be given a 'drug holiday' after 5 years (oral) or 3 years (IV zoledronate) in low-risk patients — continued DEXA monitoring guides decisions. Drug holidays are not recommended for denosumab (rebound effect on cessation) or teriparatide (24-month lifetime limit, fixed). After stopping teriparatide, an anti-resorptive agent MUST be prescribed to preserve the anabolic gains.
SELF-CHECK
A postmenopausal woman with osteoporosis (T-score –2.8) has eGFR 30 mL/min. Which agent is most appropriate?
A. A. Alendronate 70 mg weekly (oral bisphosphonate)
B. B. Zoledronic acid IV infusion annually
C. C. Denosumab 60 mg SC every 6 months
D. D. Raloxifene 60 mg daily (SERM)
Reveal Answer
Answer: C. C. Denosumab 60 mg SC every 6 months
Denosumab is the preferred anti-resorptive in significant CKD. It is a monoclonal antibody (not renally cleared) and requires no dose adjustment. However, risk of hypocalcaemia increases in severe CKD — ensure calcium/vitamin D supplementation and monitor calcium levels. Alendronate and zoledronate (bisphosphonates) are contraindicated at eGFR <30–35 due to accumulation and risk of renal deterioration. Raloxifene is renally excreted and should be avoided in severe CKD; it is also ineffective for hip fracture prevention.
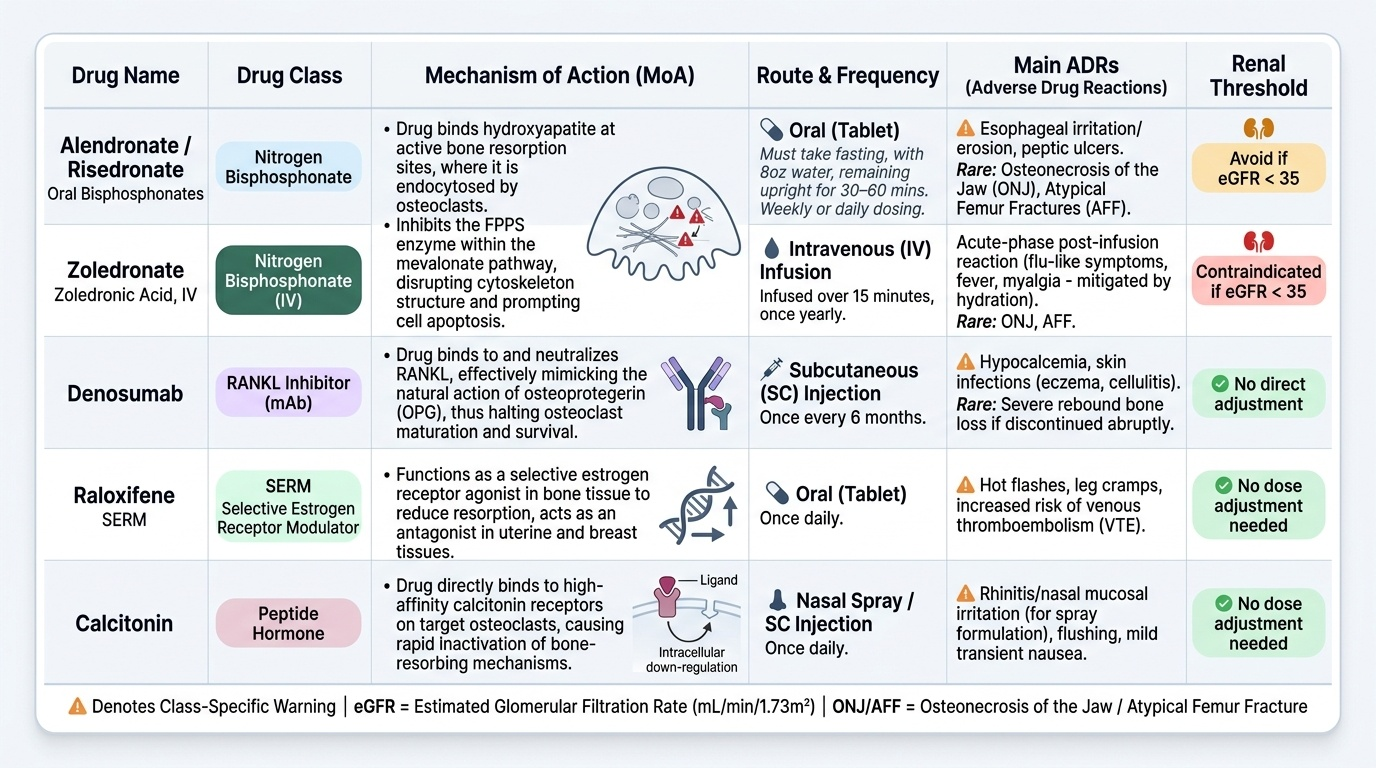
Anti-Resorptive Agents: Bisphosphonates, Denosumab, SERMs, Calcitonin
Anti-resorptive agents work by reducing the rate of osteoclast-mediated bone resorption, thereby slowing the loss of bone mass and reducing fracture risk. They do not directly stimulate new bone formation.
Bisphosphonates are the cornerstone of osteoporosis pharmacotherapy and the most widely prescribed anti-osteoporotic agents globally. They bind avidly to hydroxyapatite at bone resorption sites and are endocytosed by osteoclasts. Within the osteoclast, they inhibit farnesyl pyrophosphate synthase (an enzyme in the mevalonate/cholesterol biosynthesis pathway) — disrupting osteoclast cytoskeletal function, impairing osteoclast attachment to bone, and ultimately triggering osteoclast apoptosis. Non-nitrogen bisphosphonates (etidronate) incorporate into ATP analogues and are less potent. Nitrogen-containing bisphosphonates (alendronate, risedronate, ibandronate, zoledronate) are far more potent.
Pharmacokinetics: Oral bisphosphonates have extremely poor bioavailability (~0.5–2%) — must be taken fasting, with a full glass of water, 30–60 minutes before food, while remaining upright. IV zoledronate (5 mg once yearly) bypasses this absorption problem and is preferred in malabsorption or poor compliance. Renal excretion — oral bisphosphonates: avoid if eGFR <30–35; IV zoledronate: contraindicated eGFR <35.
ADRs:
- GI: oesophageal irritation, peptic ulceration (oral) — avoid in oesophageal disease; take upright
- Acute phase reaction: flu-like symptoms, fever, myalgia (first IV dose) — prehydrate
- Osteonecrosis of the jaw (ONJ): rare, more common with high-dose IV (oncology use) — dental check before starting long-term IV bisphosphonate
- Atypical femoral fracture (AFF): rare, with prolonged use (>5 years) — thigh/groin pain is warning; X-ray 'lateral cortical beaking'
- Hypocalcaemia: especially with IV — ensure calcium/vitamin D supplementation
Denosumab (Prolia): A fully human monoclonal IgG2 antibody against RANK-L — mimics OPG, blocking osteoclast formation, function, and survival. Administered SC every 6 months. Advantages: no renal dose adjustment (preferred in CKD), high efficacy (FREEDOM trial: 68% reduction in vertebral fractures). Key ADR: rebound bone loss on discontinuation — must transition to bisphosphonate if stopping denosumab. Also: hypocalcaemia (especially in CKD), skin infections (cellulitis), ONJ (at therapeutic doses, rare).
SERMs — Raloxifene: Selective oestrogen receptor modulator — oestrogen agonist in bone and cardiovascular tissue, antagonist in breast and uterus. Reduces vertebral fracture risk (~30–50%); does NOT reduce hip fracture risk (key limitation). Advantages: reduces breast cancer risk (ER-positive). Avoid in women with uterine bleeding or oestrogen-sensitive cancers. ADRs: hot flushes, deep venous thrombosis (DVT — oestrogen-like procoagulant effect), leg cramps. Not recommended in postmenopausal women who have had prior VTE.
Calcitonin (Salmon Calcitonin): Inhibits osteoclast activity by binding calcitonin receptors on osteoclasts. Nasal spray (200 IU daily) or SC injection. Modest efficacy (30% vertebral fracture reduction, no hip benefit). Analgesic effect for acute vertebral fracture pain is a useful clinical niche. Generally second-line due to modest efficacy and potential for long-term carcinogenicity (EMA restriction). ADRs: nasal irritation (nasal spray), nausea, flushing.
Provided image