Page 6 of 36
PH7.2 | PH7.2 | Osteoporosis Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Anabolic and Dual-Action Agents: Teriparatide and Romosozumab
For patients with severe osteoporosis (T-score ≤ –3.0, multiple fractures), anti-resorptive agents are often insufficient — the skeleton has already lost so much trabecular architecture that reducing further resorption yields limited gain. Anabolic agents that stimulate new bone formation are a qualitative advance — they rebuild bone architecture, not just slow its loss.
Teriparatide (Forteo): Consists of the biologically active N-terminal 34 amino acids of parathyroid hormone [PTH(1-34)]. The paradox of PTH: continuous elevation (as in hyperparathyroidism) activates osteoclasts and causes bone loss; intermittent, pulsatile administration (20 mcg SC daily) preferentially activates osteoblasts — net bone formation. The mechanism is complex: intermittent PTH increases IGF-1 production, reduces osteoblast apoptosis, and shifts Wnt signalling towards osteoblast proliferation. Efficacy: NEER trial — 65% reduction in vertebral fractures, 53% reduction in non-vertebral fractures in women with prior fractures. Administered as daily SC injection for up to 24 months (lifetime maximum) — this cap exists because of osteosarcoma development in rats given very high doses for their entire lifespan. Regulatory approval restricts lifetime use to 24 months. After stopping teriparatide, an anti-resorptive agent must be started to prevent rapid loss of the anabolic gains. ADRs: hypercalcaemia, nausea, leg cramps, dizziness, orthostatic hypotension (initial doses), rare increase in uric acid.
Abaloparatide is a PTH-related protein (PTHrP) analogue — similar mechanism, also anabolic, 24-month limit applies.
Romosozumab (Evenity): A monoclonal antibody against sclerostin — the osteocyte-derived Wnt inhibitor. By blocking sclerostin, Wnt/β-catenin signalling in osteoblasts is unleashed, dramatically increasing bone formation. Simultaneously, RANK-L is indirectly decreased, reducing resorption — a dual anabolic + anti-resorptive effect. Administered as 210 mg SC monthly for 12 months only (not long-term). FRAME trial: significant fracture reduction at 12 months versus placebo. CV risk concern: an imbalance in cardiovascular events (MI, stroke) was noted versus active comparator in ARCH trial — romosozumab is contraindicated within 12 months of MI or stroke. After romosozumab, transition to an anti-resorptive.
Drug sequencing rationale: For severe osteoporosis — start with anabolic (teriparatide/romosozumab) to build architecture, then transition to anti-resorptive (denosumab, bisphosphonate) to preserve gains. Anti-resorptive after anabolic = 'lock in the gains.' Anabolic after anti-resorptive (especially after denosumab) is less effective (blunted osteoblast response).
CLINICAL PEARL
Two sequencing rules determine treatment outcome in osteoporosis. First: after teriparatide (24 months, lifetime maximum), you MUST prescribe an anti-resorptive — without it, bone density falls rapidly back to pre-treatment levels within 12 months, wasting a full 2-year anabolic course. Second: denosumab is a commitment — it cannot simply be stopped without a transition plan. On denosumab discontinuation, RANK-L rebounds sharply (OPG-like block is lifted), triggering a burst of osteoclast activity that can cause rapid vertebral fractures within 6–12 months (rebound effect). Always bridge to a bisphosphonate when stopping denosumab.
SELF-CHECK
A 72-year-old woman with severe osteoporosis (T-score –3.8, two prior vertebral fractures) completes 24 months of teriparatide. What is the correct next step?
A. A. Stop all medication — anabolic course is complete
B. B. Start denosumab or a bisphosphonate to preserve the bone density gained
C. C. Restart teriparatide for another 24-month course
D. D. Switch to calcitonin nasal spray for maintenance
Reveal Answer
Answer: B. B. Start denosumab or a bisphosphonate to preserve the bone density gained
After completing teriparatide, an anti-resorptive (denosumab or bisphosphonate) must be started immediately to 'lock in' the anabolic gains. Without an anti-resorptive, the bone density gained returns to near-baseline within 12 months. Teriparatide cannot be restarted — the 24-month lifetime limit is a regulatory safety ceiling based on osteosarcoma risk in animal studies. Calcitonin is too weak to preserve the gains from a teriparatide course.
Clinical Decision-Making: Female vs Male Osteoporosis Management Plans
Management of osteoporosis is sex-specific due to differences in aetiology, hormonal milieu, and drug response. Both sexes require the same calcium/vitamin D foundation, lifestyle modification (weight-bearing exercise, fall prevention, smoking cessation), and treatment of secondary causes.
Postmenopausal Female Osteoporosis:
First-line: Alendronate 70 mg once weekly or risedronate 35 mg once weekly (oral bisphosphonates) — most evidence for hip and vertebral fracture prevention, generic, affordable. For patients with poor oral tolerance, oesophageal disease, or poor compliance: zoledronic acid 5 mg IV once yearly (highly effective; single infusion; but avoid in eGFR <35). For patients with CKD: denosumab (no renal dose adjustment). For younger postmenopausal women (<70 years) concerned about breast cancer: raloxifene — SERM with concurrent breast cancer risk reduction; however, does NOT protect against hip fractures and increases DVT risk.
Severe osteoporosis (T-score ≤ –3.0 with fractures): teriparatide 20 mcg SC daily × 24 months → transition to bisphosphonate or denosumab. Romosozumab if prior fractures and high CV risk is NOT a contraindication (check 12-month MI/stroke window).
Male Osteoporosis:
Secondary causes must be excluded first: measure testosterone, LH/FSH, calcium, phosphate, 25-OH vitamin D, PTH, thyroid function, PSA (if on anti-androgen therapy), and screen for glucocorticoid use, alcoholism. Primary hypogonadism → testosterone replacement (also improves bone density, but not a primary osteoporosis drug). Glucocorticoid-induced osteoporosis (GIO): initiate bisphosphonate if starting long-term steroids (prednisolone >7.5 mg/day for >3 months).
First-line: Alendronate or risedronate (both approved for male osteoporosis). Alternatively zoledronic acid for compliance issues. Teriparatide for severe male osteoporosis (T-score ≤ –2.5 with fractures or failure of anti-resorptives). Denosumab is approved and useful in male osteoporosis including men on ADT (androgen deprivation therapy) for prostate cancer.
| Feature | Female (Postmenopausal) | Male |
|---|---|---|
| First-line | Alendronate/risedronate | Alendronate/risedronate |
| CKD | Denosumab | Denosumab |
| Severe disease | Teriparatide 24 months → anti-resorptive | Teriparatide (or denosumab) |
| Additional option | Raloxifene (+ breast protection) | Testosterone (if hypogonadal) |
| Avoid | Raloxifene if prior DVT/stroke | — |
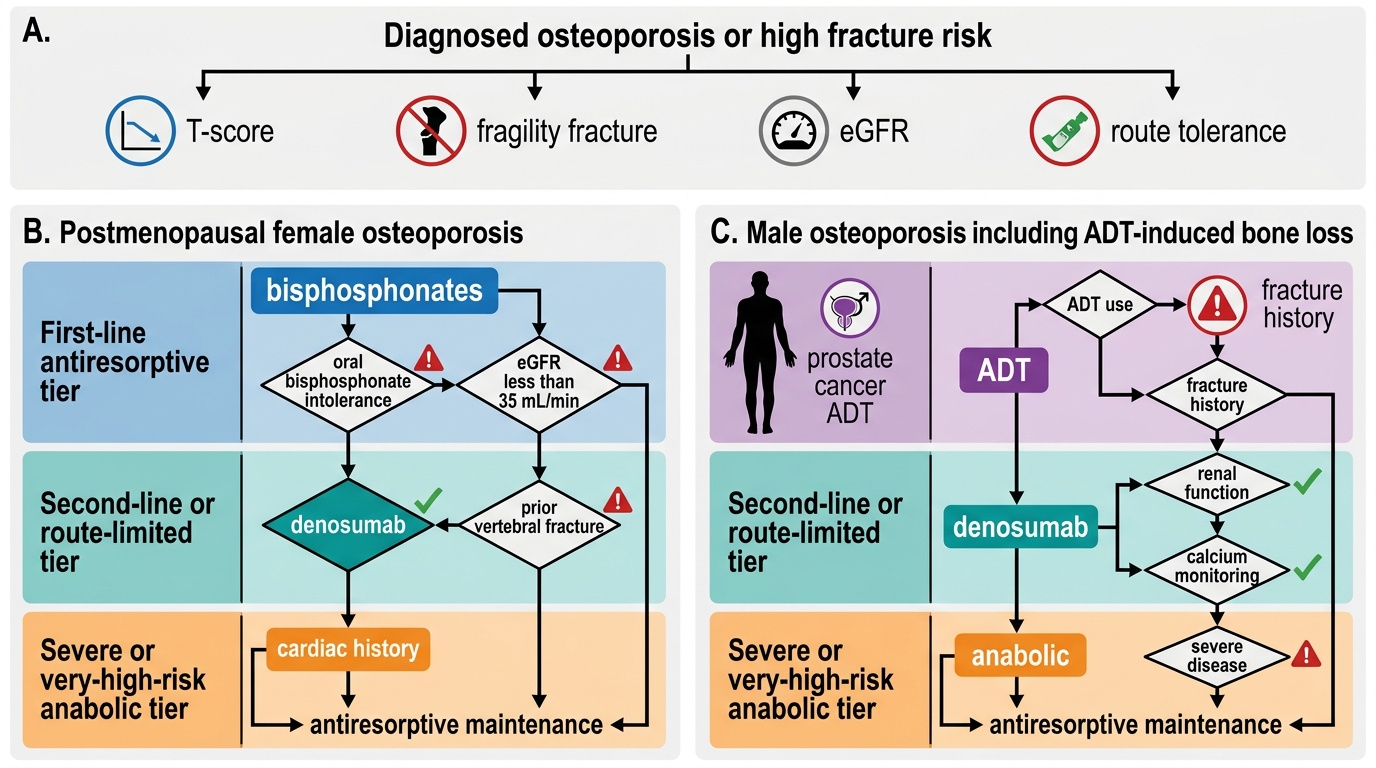
Osteoporosis Drug Selection Algorithm
Self-Assessment: Fracture Risk and Drug Choice
Apply the pharmacological principles above to these two clinical scenarios:
Scenario A (Female): A 65-year-old postmenopausal woman, T-score –3.1, one prior vertebral fracture, eGFR 55, no cardiac history. She is intolerant of oral bisphosphonates (oesophageal reflux disease). She asks whether she needs 'injections' and is concerned about cancer risk from treatment.
Recommendation: Zoledronic acid 5 mg IV once yearly (eGFR 55 is above the threshold of 35 for IV zoledronate; bypasses oesophageal issue). Alternatively denosumab SC 6-monthly — also no oral intake needed and no renal caution. Address cancer concern: neither drug causes cancer at therapeutic doses. Counsel on ONJ (rare, dental check before IV zoledronate) and acute phase reaction (first infusion).
Scenario B (Male): A 58-year-old man with prostate cancer on long-term androgen deprivation therapy (ADT) — testosterone suppressed — presents with T-score –2.7, no fracture history, eGFR 70. Management: ADT-induced osteoporosis is a well-recognised complication. Initiate denosumab 60 mg SC 6-monthly (approved for bone loss in men on ADT; equivalent efficacy; convenient SC injection). Monitor calcium. If eGFR deteriorates, denosumab remains preferred (no renal adjustment). Alendronate is a reasonable alternative. Testosterone replacement is not indicated while on intentional ADT for prostate cancer.
SELF-CHECK
Which anti-osteoporotic drug carries a specific warning about rebound vertebral fractures if discontinued abruptly?
A. A. Alendronate (oral bisphosphonate)
B. B. Teriparatide (PTH analogue)
C. C. Denosumab (RANK-L inhibitor)
D. D. Raloxifene (SERM)
Reveal Answer
Answer: C. C. Denosumab (RANK-L inhibitor)
Denosumab has a documented rebound effect on discontinuation — the RANK-L block (which mimics OPG) is lifted, causing a surge in osteoclast activity within 3–6 months, leading to rapid bone loss and sometimes multiple new vertebral fractures. This is a unique pharmacological hazard of denosumab not shared by bisphosphonates (which remain embedded in bone after stopping), teriparatide (which is stopped intentionally with planned anti-resorptive follow-on), or raloxifene (modest, gradual loss on stopping).