Page 8 of 36
PH7.3 | PH7.3 | Thyroid Disorder Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Describe the mechanism of action and pharmacokinetics of levothyroxine and liothyronine for hypothyroidism
- Classify antithyroid drugs and explain the additional advantage of propylthiouracil over carbimazole
- Justify drug selection in special scenarios: pregnancy (trimester-specific), thyroid storm, and pre-operative preparation
- Devise a management plan for a patient presenting with hypothyroidism or hyperthyroidism
INSTRUCTIONS
Thyroid disorders are the most common endocrine diseases in India after diabetes, affecting an estimated 42 million people. Hypothyroidism is frequently under-recognised, and hyperthyroidism (especially Graves' disease) carries significant morbidity if untreated. The pharmacological management of both conditions is nuanced — drug choice in pregnancy (trimester-specific), the critical role of PTU's extra mechanism, and the risks of radioactive iodine are all high-yield clinical pharmacology concepts.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 20 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 46 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old pregnant woman at 10 weeks gestation presents with tremor, palpitations, heat intolerance, and weight loss despite good appetite. TSH is undetectable, free T4 is 4.2 ng/dL (markedly elevated), and the patient has an exophthalmos. She is diagnosed with Graves' disease. Her obstetrician asks you: Which antithyroid drug is safest in the first trimester? When should you consider switching drugs? Can she receive radioactive iodine? This clinical scenario encapsulates the most important prescribing decisions in thyroid pharmacotherapy.
WHY THIS MATTERS
Thyroid disease spans a pharmacological spectrum from simple hormone replacement to complex antithyroid regimens with life-threatening adverse effects (agranulocytosis). The correct drug choice depends not just on the disease but on the patient: a pregnant woman with Graves' disease needs a different drug in the 1st trimester than in the 2nd; a patient in thyroid storm needs rapid T4→T3 blockade that only PTU provides; a patient on levothyroxine with concurrent iron or calcium supplements may be under-replaced due to absorption interactions. These nuances are assessed in NMC clinical pharmacology examinations and directly affect patient safety.
RECALL
The thyroid gland synthesises two hormones: thyroxine (T4) and triiodothyronine (T3). Synthesis occurs in follicular cells: (1) Iodide trapping — active transport via Na⁺/I⁻ symporter (NIS) from blood into follicular cells; (2) Oxidation — iodide → iodine by thyroid peroxidase (TPO) using H₂O₂; (3) Organification — iodine covalently binds tyrosine residues on thyroglobulin (MIT = monoiodotyrosine; DIT = diiodotyrosine); (4) Coupling — MIT + DIT → T3; DIT + DIT → T4 (catalysed by TPO); (5) Release — thyroglobulin proteolysis; T4 and T3 released into blood (5:1 ratio, T4 predominates). T4 is a prohormone — most T3 (80%) is produced by peripheral deiodination of T4 in liver and kidney by 5'-deiodinase (type 1). T3 is 3–4× more potent than T4 with shorter half-life. HPT axis: TRH (hypothalamus) → TSH (pituitary) → T3/T4 synthesis; T3/T4 exert negative feedback on both. TSH measurement is the primary clinical monitoring tool — highly sensitive to small changes in thyroid hormone levels.
Thyroid Physiology Recap: Synthesis, Regulation, and Peripheral Action
Understanding thyroid pharmacology requires a clear map of where in the synthetic pathway each drug intervenes. Thionamides (carbimazole, PTU) block thyroid peroxidase — the enzyme responsible for iodide oxidation, organification, and coupling. Since they do not discharge stored thyroglobulin, their onset of action takes 1–3 weeks as pre-formed hormone is consumed. This lag is clinically critical: do not expect immediate symptom relief from thionamides alone — beta-blockers address the adrenergic symptoms while thionamides work upstream.
Lugol's iodine (potassium iodide + iodine solution) works by the Wolff-Chaikoff effect: high concentrations of iodide paradoxically inhibit their own organification, temporarily blocking further thyroid hormone synthesis. This effect is transient (1–2 weeks, before 'escape'), making Lugol's iodine useful only as a short-term adjunct — pre-operatively to reduce gland vascularity (Plummer's preparation), or in thyroid storm. It must never be used as the primary antithyroid treatment due to escape.
PTU's unique additional mechanism: In addition to TPO inhibition (shared with carbimazole/methimazole), PTU inhibits peripheral 5'-deiodinase — the enzyme that converts circulating T4 to the active T3. This dual action makes PTU particularly valuable in thyroid storm (where circulating T3 must be reduced quickly) and is the pharmacological basis for its preferred use in the first trimester of pregnancy.
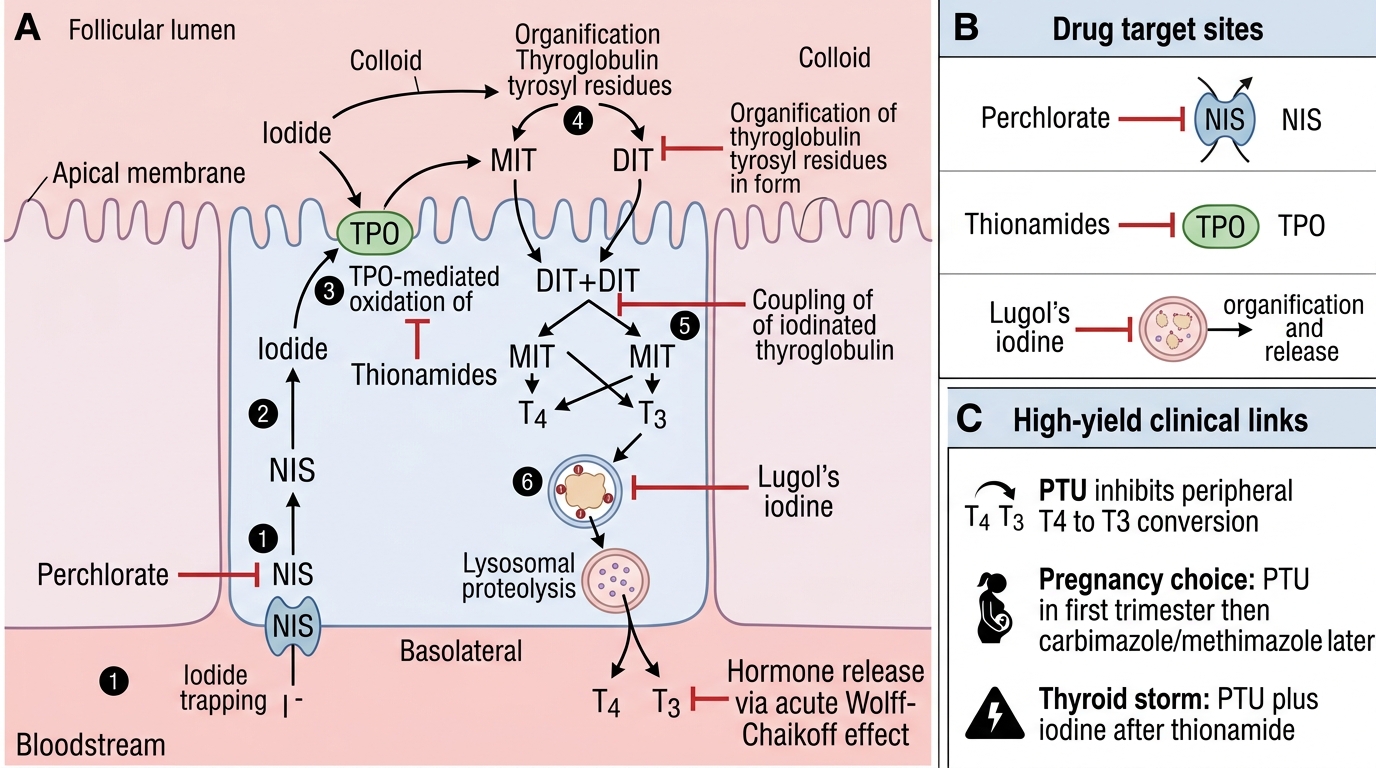
Thyroid Hormone Synthesis and Antithyroid Drug Targets
Therapeutic Goals: Restoring Euthyroidism
The overarching goal of thyroid pharmacotherapy is the restoration and maintenance of euthyroidism — a biochemical and clinical state in which thyroid hormone levels are appropriate for the patient's physiological needs, reflected by a normal TSH.
For hypothyroidism: the target TSH is 0.5–2.5 mIU/L for most adults; in the elderly or those with cardiovascular disease, a TSH of 1–4 mIU/L may be acceptable; in pregnancy, the target is lower (0.1–2.5 mIU/L in 1st trimester) due to increased metabolic demands and fetal development dependence on maternal thyroid hormones. The goal is not simply a normal TSH but resolution of symptoms (fatigue, cold intolerance, weight gain, constipation, bradycardia, dyslipidaemia).
For hyperthyroidism: the treatment goal depends on the chosen modality — medical therapy aims for biochemical euthyroidism within 4–8 weeks of antithyroid drug initiation; definitive therapy (radioactive iodine, surgery) aims for controlled euthyroidism or planned hypothyroidism (treated with levothyroxine). For Graves' ophthalmopathy, prompt achievement of euthyroidism is important as both hypo- and hyperthyroidism can worsen eye disease.
Monitoring tool: TSH is the gold-standard monitoring test — it responds sensitively to free T4 changes. However, TSH lags behind free T4 changes by 6–8 weeks; in initial dose adjustment, measure free T4 AND TSH together for the first few months. A low TSH alone does not require dose reduction if the patient is clinically euthyroid and free T4 is normal — this is particularly relevant in patients on levothyroxine who feel better at a slightly lower TSH.
SELF-CHECK
A 24-year-old woman with Graves' disease is 8 weeks pregnant. She is started on antithyroid therapy. Which drug is preferred at this stage and why?
A. A. Carbimazole — safer in all trimesters
B. B. Propylthiouracil (PTU) — crosses the placenta less and carbimazole is teratogenic in the 1st trimester
C. C. Radioactive iodine — most definitive treatment
D. D. Propranolol only — antithyroid drugs are contraindicated in pregnancy
Reveal Answer
Answer: B. B. Propylthiouracil (PTU) — crosses the placenta less and carbimazole is teratogenic in the 1st trimester
PTU is preferred in the FIRST TRIMESTER of pregnancy for two reasons: (1) carbimazole is associated with a teratogenic syndrome (aplasia cutis, choanal atresia, omphalocele) especially in the 1st trimester critical organogenesis period; (2) PTU crosses the placenta less than carbimazole. After the 1st trimester (from 2nd trimester onward), switch back to carbimazole because PTU carries higher risk of severe maternal hepatotoxicity with prolonged use. Radioactive iodine is absolutely contraindicated in pregnancy (fetal thyroid ablation). Propranolol alone does not treat hyperthyroidism.
Hypothyroidism Drugs: Levothyroxine and Liothyronine
Levothyroxine (L-thyroxine, LT4) is the standard treatment for hypothyroidism and one of the most commonly prescribed drugs globally. It is a synthetic T4 — an inactive prohormone that must be converted to T3 peripherally by 5'-deiodinase. This peripheral conversion system provides the physiological T3/T4 mix, making levothyroxine a near-perfect replacement for natural thyroid hormone secretion.
Pharmacokinetics: Oral absorption is 70–80% in the fasting state — greatly reduced by food (especially fibre-rich meals), calcium supplements, iron supplements, antacids, cholestyramine, and PPIs. Must be taken 30–60 minutes before breakfast on an empty stomach. Half-life is 7 days (T4), allowing once-daily dosing. Time to full effect at a given dose: 6–8 weeks (due to the long T4 half-life). Metabolism: hepatic deiodination, glucuronidation; renal excretion of metabolites.
Dosing: Typical full replacement dose is 1.6 mcg/kg/day. However, in elderly patients and those with ischaemic heart disease, start with 12.5–25 mcg/day and uptitrate slowly every 4–6 weeks — because rapid normalisation of T4 increases myocardial oxygen demand and can precipitate angina or arrhythmia. Overcorrection (over-treatment) suppresses TSH below normal and causes iatrogenic hyperthyroidism — risk of atrial fibrillation (especially in elderly), osteoporosis (with prolonged TSH suppression), and tremor.
Drug interactions: Many commonly used drugs impair levothyroxine absorption — counsel patients explicitly: take alone with plain water, at least 2–4 hours before iron, calcium, or antacids. Rifampicin, phenytoin, carbamazepine induce hepatic enzymes → increase levothyroxine clearance (may need dose increase). Amiodarone (rich in iodine) causes complex interactions — can cause both hypo- and hyperthyroidism.
ADRs (mainly from over-treatment): palpitations, anxiety, tremor, insomnia, weight loss, diarrhoea, AF (especially in elderly). Under-treatment: persistent fatigue, weight gain, constipation, bradycardia.
Liothyronine (L-triiodothyronine, LT3): Synthetic T3 — more potent, faster onset (half-life 1 day), immediate action. Used in: myxoedema coma (IV liothyronine — when rapid T3 action is needed and peripheral T4→T3 conversion is impaired in critically ill patients), combination T4+T3 therapy in patients with persistent symptoms on levothyroxine alone, and diagnosis of thyroid cancer (acute TSH stimulation after stopping levothyroxine before radioiodine scanning). Disadvantages: short half-life requires multiple daily doses; higher risk of cardiac ADRs with peaks of T3 activity.