Page 9 of 36
PH7.3 | PH7.3 | Thyroid Disorder Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Hyperthyroidism Drugs: Thionamides, Iodine, Beta-Blockers
The pharmacological management of hyperthyroidism uses a combination of agents targeting different aspects of the pathophysiology: synthesis inhibition (thionamides), temporary organification block (iodine/iodides), peripheral T4→T3 conversion inhibition (PTU, propranolol), and symptom control (beta-blockers).
Provided image
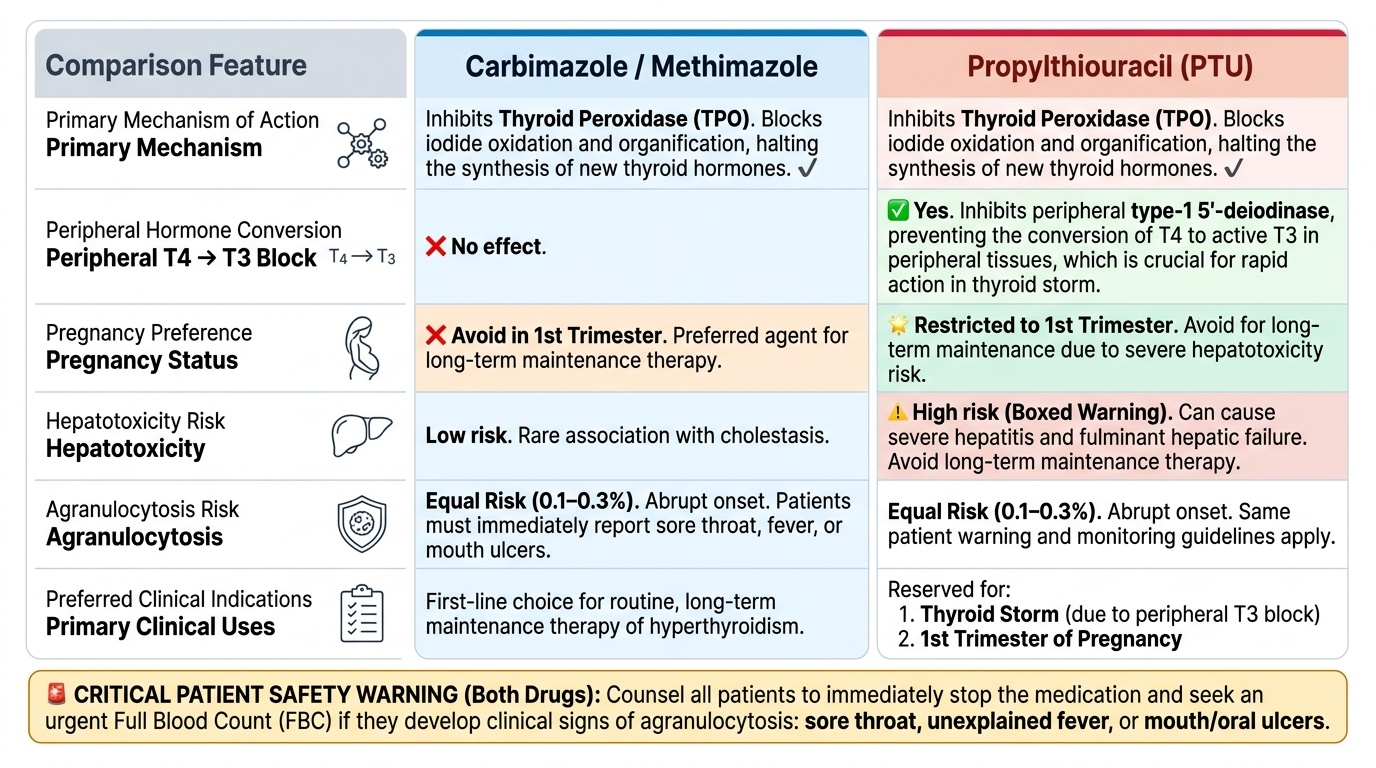
Thionamides — Carbimazole and PTU:
Both carbimazole (converted in vivo to methimazole — the active form) and propylthiouracil (PTU) inhibit thyroid peroxidase (TPO), blocking iodide oxidation and organification — thus stopping new thyroid hormone synthesis. Existing stored hormone continues to be released, explaining the 1–3 week delay to biochemical effect. For clinical symptom control during this lag, combine with a beta-blocker.
Critical difference — PTU's extra mechanism: PTU, unlike carbimazole, also inhibits peripheral type-1 5'-deiodinase — blocking T4→T3 conversion at peripheral tissues (liver, kidney). This provides a faster reduction in circulating T3 and is crucial in thyroid storm.
ADRs of thionamides:
- Agranulocytosis (most serious, 0.1–0.3%) — abrupt onset, reversible if caught early; WARN ALL PATIENTS to stop the drug and report immediately if they develop sore throat, fever, or oral ulcers. Check FBC if suspected — drug holiday + G-CSF if severe.
- Hepatotoxicity: PTU > carbimazole — PTU causes severe hepatitis (including fulminant hepatic failure) with long-term use, especially concerning in children and prolonged adult therapy → prefer carbimazole for maintenance; PTU restricted to 1st trimester pregnancy and thyroid storm.
- Rash, pruritus (switch to the other thionamide if minor).
- Cholestasis (rare, carbimazole).
- SLE-like syndrome (PTU, rare).
Iodine and Iodides (Lugol's Iodine): High-dose iodide transiently blocks organification via the Wolff-Chaikoff effect (iodine overload inhibits TPO-dependent organification). Additionally reduces thyroid gland vascularity (surgically useful). Uses: (1) Pre-operative preparation for thyroidectomy in Graves' disease — 10–14 days of Lugol's before surgery reduces vascularity and surgical bleeding; (2) Thyroid storm adjunct; (3) Radiation emergency prophylaxis. NOT for long-term antithyroid therapy — thyroid 'escapes' Wolff-Chaikoff effect after 1–2 weeks.
Beta-Blockers (Propranolol): Non-selective beta-blocker. Controls adrenergic symptoms of hyperthyroidism: tachycardia, tremor, anxiety, sweating, heat intolerance. Does NOT reduce thyroid hormone synthesis — purely symptomatic. Additional property: propranolol at high doses inhibits peripheral T4→T3 conversion (type-2 deiodinase, hepatic). Used as bridge therapy while thionamides take effect, and in thyroid storm.
Radioactive Iodine (¹³¹I): Oral sodium iodide-131 — concentrated in thyroid follicular cells (as iodine is) → emits beta radiation → destroys thyroid tissue. Safe, definitive outpatient treatment for Graves' disease, toxic adenoma, and toxic multinodular goitre. Onset of effect: 6–12 weeks; may cause initial transient worsening (radiation thyroiditis). Contraindications: pregnancy, breast-feeding, active Graves' ophthalmopathy (may worsen eye disease), large compressive goitre, suspected malignancy. Most patients ultimately become hypothyroid (intended in many; treated with levothyroxine).
CLINICAL PEARL
PTU vs Carbimazole — the pregnancy switch rule: In the first trimester, use PTU (carbimazole teratogenicity risk). From the second trimester, switch back to carbimazole (PTU's hepatotoxicity risk outweighs its benefits in prolonged use). This bidirectional switch is one of the most clinically tested aspects of thyroid pharmacology. Separately: agranulocytosis is a medical emergency in any patient on thionamides — every patient prescribed carbimazole or PTU MUST receive a written warning to attend hospital immediately if they develop sore throat, fever, or mouth ulcers. A verbal reminder at every prescription is good practice.
SELF-CHECK
A patient with Graves' disease develops a sore throat and fever on day 14 of carbimazole. The FBC shows total WBC 1.2 × 10⁹/L (neutrophils 0.3 × 10⁹/L). The next step is:
A. A. Reduce the carbimazole dose and add antibiotics
B. B. Switch to PTU and continue antithyroid therapy
C. C. Stop carbimazole immediately, isolate and monitor for infection, consider G-CSF
D. D. Add lithium carbonate as an alternative antithyroid agent
Reveal Answer
Answer: C. C. Stop carbimazole immediately, isolate and monitor for infection, consider G-CSF
This is drug-induced agranulocytosis — a potentially fatal ADR of thionamides. STOP the drug immediately. Switching to PTU is NOT safe as cross-reactivity of agranulocytosis between carbimazole and PTU is well-documented (~30–50%). The patient is severely neutropenic (ANC ~0.3) and at high infection risk — reverse barrier nursing, blood cultures, broad-spectrum antibiotics if febrile, G-CSF to stimulate neutrophil recovery. Alternative antithyroid options (Lugol's iodine, cholestyramine, lithium — very rarely used) may be considered short-term. Definitive management: radioactive iodine or surgery once euthyroid is re-established safely.
Clinical Decision-Making: Managing Hypothyroidism and Hyperthyroidism
Sound clinical pharmacology in thyroid disease requires integrating the patient's disease type, severity, comorbidities, and special circumstances (pregnancy, planned surgery, cardiac disease) into a coherent management plan.
Hypothyroidism management:
- Overt hypothyroidism (elevated TSH + low free T4, symptomatic): Levothyroxine 1.6 mcg/kg/day starting dose in young healthy adults. Start low (12.5–50 mcg/day) in elderly (>60 years) and those with cardiac disease — rapid T3 increase can precipitate angina, AF, acute MI. Uptitrate every 6–8 weeks guided by TSH.
- Subclinical hypothyroidism (raised TSH, normal free T4): Treatment debated. Generally treat if TSH >10 mIU/L, or if symptomatic, or in pregnancy. TREAT trial showed levothyroxine did NOT improve QoL in older adults with subclinical hypothyroidism — individualize.
- Myxoedema coma: IV liothyronine (300–400 mcg loading dose) — most rapid T3 delivery when peripheral conversion is impaired; concurrent IV hydrocortisone (relative adrenal insufficiency common), rewarming, supportive care.
Hyperthyroidism management:
Choice of treatment modality for Graves' disease:
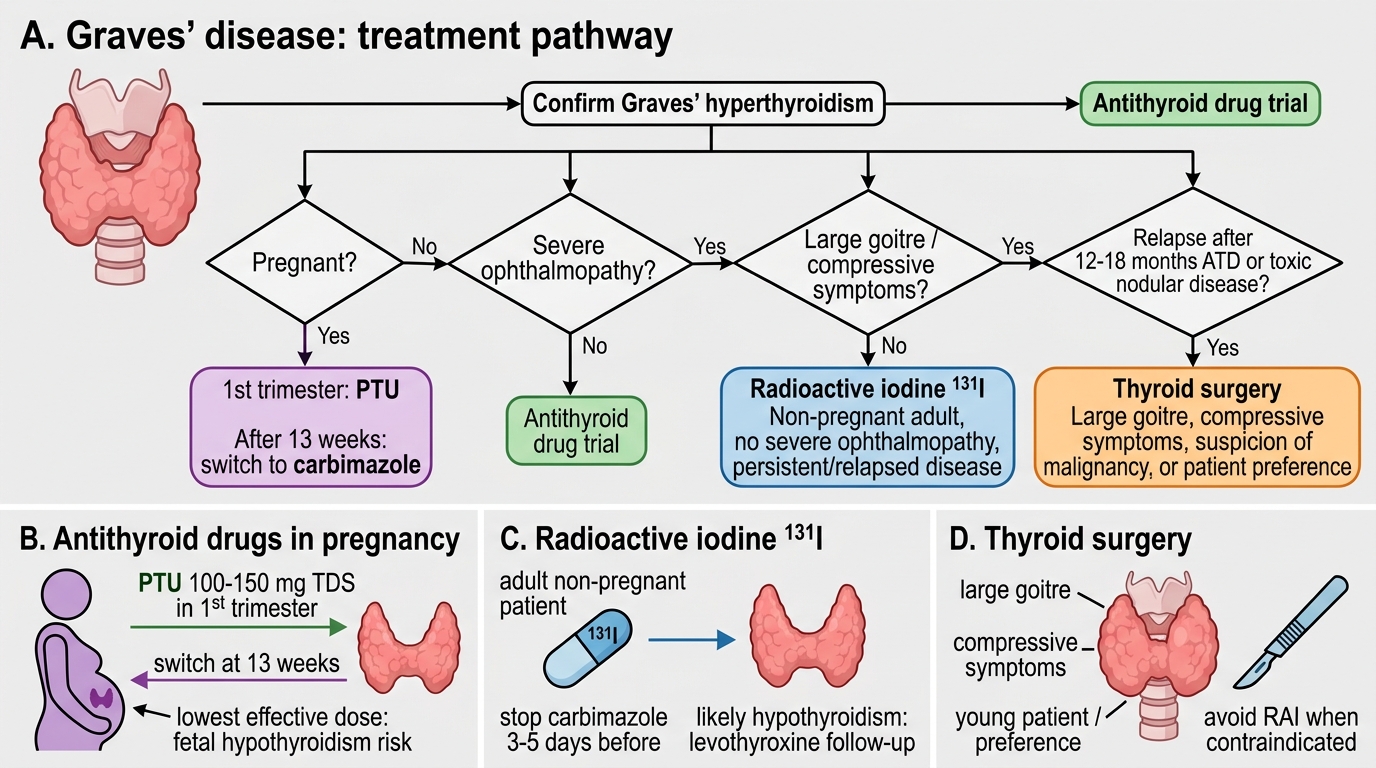
1. Antithyroid drugs (carbimazole/PTU): First-line for most patients; remission rate ~50% after 12–18 months; relapse common (30–40% within 2 years). Preferred in: pregnancy, mild disease, young patients seeking euthyroidism without radiation.
2. Radioactive iodine (¹³¹I): Preferred in: older patients, relapsed Graves', toxic multinodular goitre, toxic adenoma. Contraindicated in pregnancy. Results in hypothyroidism in most cases — this is planned and acceptable.
3. Thyroidectomy (subtotal): Preferred in: large goitre (compressive symptoms), co-existing suspected thyroid malignancy, severe Graves' ophthalmopathy where rapid euthyroidism is needed, patient preference, or failure of medical therapy. Pre-operative preparation: carbimazole to achieve euthyroidism, then Lugol's iodine 10–14 days before surgery (reduces vascularity and surgical bleeding).
Thyroid storm management (thyrotoxic crisis — life-threatening emergency):
1. PTU 200 mg 6-hourly (blocks synthesis AND peripheral T4→T3 conversion) — first choice because of dual mechanism
2. After PTU loading: Lugol's iodine (1 hour AFTER PTU — if given before PTU, will provide iodine substrate for ongoing synthesis)
3. Propranolol IV — heart rate control, additional T4→T3 conversion inhibition
4. Hydrocortisone — adrenal axis support (stress response); also inhibits T4→T3 conversion
5. Treat precipitating cause (infection, surgery, iodine load)
Graves' Disease Management Algorithm
Self-Assessment: Thyroid Drug Scenarios
Test your integration of thyroid pharmacology with these scenarios:
Scenario A: A 32-year-old woman with Graves' hyperthyroidism is 7 weeks pregnant. Her free T4 is 3.8 ng/dL (very elevated). What drug do you start, at what dose range, and what do you tell her about the drug holiday at 13 weeks?
Answer: PTU — preferred in 1st trimester (carbimazole teratogenicity). Starting dose typically 100–150 mg TDS, titrated to lowest effective dose. At 13 weeks, switch to carbimazole (PTU hepatotoxicity risk increases with duration). Inform that both drugs cross the placenta and can cause fetal hypothyroidism — use the lowest effective dose. Breastfeeding: low-dose carbimazole is preferred (less breast milk transfer than PTU).
Scenario B: A 50-year-old man with toxic nodular goitre and persistent hyperthyroidism despite 18 months of carbimazole. No ophthalmopathy. He refuses surgery. TSH <0.01, free T4 elevated. What do you recommend?
Answer: Radioactive iodine (¹³¹I) — standard for non-pregnant adult with relapsed or persistent hyperthyroid nodular disease. Pre-treat with carbimazole if severely thyrotoxic, stop carbimazole 3–5 days before radioiodine (to allow iodine uptake). Warn that hypothyroidism is likely (plan levothyroxine). Monitor TSH at 6 weeks, 3 months, 6 months.
Scenario C: Why is Lugol's iodine given AFTER PTU in thyroid storm, not before?
Answer: If iodine is given before thionamide, the thyroid uses the excess iodide as substrate for more T4/T3 synthesis ('iodide escape' from the Wolff-Chaikoff effect can take longer than the storm). PTU must first block TPO so no new hormone synthesis occurs; only then does Lugol's iodine addition safely exploit the Wolff-Chaikoff block on organification without providing substrate for synthesis.
SELF-CHECK
Which statement correctly describes the additional pharmacological advantage of PTU over carbimazole?
A. A. PTU has lower teratogenicity risk, making it safer in all trimesters
B. B. PTU inhibits peripheral T4 to T3 conversion by blocking 5'-deiodinase, in addition to blocking TPO
C. C. PTU does not cross the placenta at all
D. D. PTU has a longer half-life, allowing once-daily dosing
Reveal Answer
Answer: B. B. PTU inhibits peripheral T4 to T3 conversion by blocking 5'-deiodinase, in addition to blocking TPO
PTU's unique additional mechanism is inhibition of peripheral 5'-deiodinase (type 1), blocking conversion of T4 to the more active T3. This provides a faster reduction in circulating T3 and is specifically useful in thyroid storm. PTU does NOT have lower teratogenicity — carbimazole is teratogenic in the 1st trimester (making PTU preferred then), but PTU itself carries hepatotoxicity risk with prolonged use. PTU crosses the placenta (less than carbimazole, but not zero). PTU has a short half-life (1–2 hours) requiring 3× daily dosing.