Page 11 of 36
PH7.4 | PH7.4 | Anterior Pituitary Hormone Modulators — SDL Guide — SDL Guide
Learning Objectives
- Classify drugs that modify anterior pituitary hormone release into agonists, antagonists, and analogues with specific examples for each hormone axis
- Describe the mechanisms, pharmacokinetics, indications, and adverse effects of somatostatin analogues, dopamine agonists, GnRH analogues, and pegvisomant
- Explain the paradoxical effect of continuous versus pulsatile GnRH analogue administration
- Devise a management approach for acromegaly and prolactinoma using pharmacological agents
INSTRUCTIONS
The anterior pituitary is the 'master conductor' of endocrine physiology, controlling five major hormonal axes. When tumours or genetic conditions derange this conductor — too much GH causing acromegaly, excess prolactin causing galactorrhoea and infertility, premature sex hormone secretion causing precocious puberty — pharmacological modulation of the pituitary or its hypothalamic inputs is the cornerstone of management. This guide covers the diverse pharmacology of anterior pituitary modulators through the lens of their clinical applications.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 20 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 38 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old man presents with progressive enlargement of his hands and feet over 3 years, prognathism (protruding jaw), coarsening of facial features, and a new diagnosis of type 2 diabetes. Serum IGF-1 is 3× upper limit of normal and GH fails to suppress on an oral glucose tolerance test. MRI shows a pituitary macroadenoma. The neurosurgeon plans transsphenoidal surgery, but the patient's pre-operative GH is still markedly elevated. Which drug can reduce tumour size pre-operatively and lower IGF-1 to reduce surgical risk? If post-operatively GH is still elevated, what is the next pharmacological step? This scenario encapsulates the medical management of acromegaly — the highest-yield pituitary pharmacology topic.
WHY THIS MATTERS
Anterior pituitary modulators span a remarkable pharmacological range — from drugs that mimic hormone deficiency (recombinant GH, gonadotropins for infertility) to drugs that suppress pathological excess (octreotide for acromegaly, cabergoline for prolactinoma). The GnRH analogue paradox — pulsatile stimulation vs continuous suppression of gonadotropins — is a fundamental pharmacodynamic concept with applications across endocrinology, oncology (prostate cancer), and reproductive medicine. Understanding these drugs requires mastery of feedback physiology and receptor pharmacodynamics.
RECALL
The anterior pituitary (adenohypophysis) secretes six main hormones, each regulated by hypothalamic releasing or inhibiting factors: GH (stimulated by GHRH, inhibited by somatostatin); TSH (stimulated by TRH, inhibited by somatostatin); ACTH (stimulated by CRH); FSH and LH (stimulated by GnRH/LHRH); Prolactin (tonically inhibited by dopamine from the tuberoinfundibular pathway — the only axis under tonic inhibition). Key: dopamine is the prolactin-inhibitory factor — drugs blocking dopamine (antipsychotics, metoclopramide) cause hyperprolactinaemia; drugs providing dopamine agonism (bromocriptine, cabergoline) suppress prolactin. GH's metabolic duality: GH directly opposes insulin (diabetogenic — stimulates hepatic glucose output, reduces peripheral uptake) while stimulating liver to produce IGF-1 (somatomedin C) which mediates GH's growth-promoting anabolic effects. Measuring IGF-1 is the best biomarker for chronic GH excess (acromegaly) as it has a stable plasma half-life unlike the pulsatile GH.
Anterior Pituitary and Its Hormonal Axes: A Drug Target Map
Understanding anterior pituitary pharmacology begins with mapping each drug class to the specific axis it modulates. The five anterior pituitary axes — GH/IGF-1, Prolactin, TSH, ACTH/cortisol, and FSH/LH/gonadal — are each subject to complex hypothalamic regulation, creating multiple drug-intervention nodes at different levels of each axis.
For the GH axis: GHRH stimulates GH release from somatotrophs; somatostatin inhibits GH release. Three drug strategies target this axis: (1) somatostatin analogues mimic somatostatin to suppress GH (octreotide, lanreotide); (2) pegvisomant blocks the GH receptor to prevent GH action peripherally; (3) dopamine agonists (bromocriptine) paradoxically suppress GH in acromegaly (though they stimulate GH in normal physiology). For the Prolactin axis: dopamine from the hypothalamus tonically inhibits pituitary lactotrophs. Dopamine agonists (bromocriptine, cabergoline) reduce prolactin secretion by activating D2 receptors on lactotrophs. For the FSH/LH axis: GnRH (LHRH) from the hypothalamus is normally released in pulses. Continuous GnRH analogue administration overwhelms the pulsatile signal, downregulating (desensitising) GnRH receptors on gonadotrophs — paradoxically suppressing LH and FSH. Pulsatile GnRH administration mimics physiological signalling, stimulating FSH/LH.
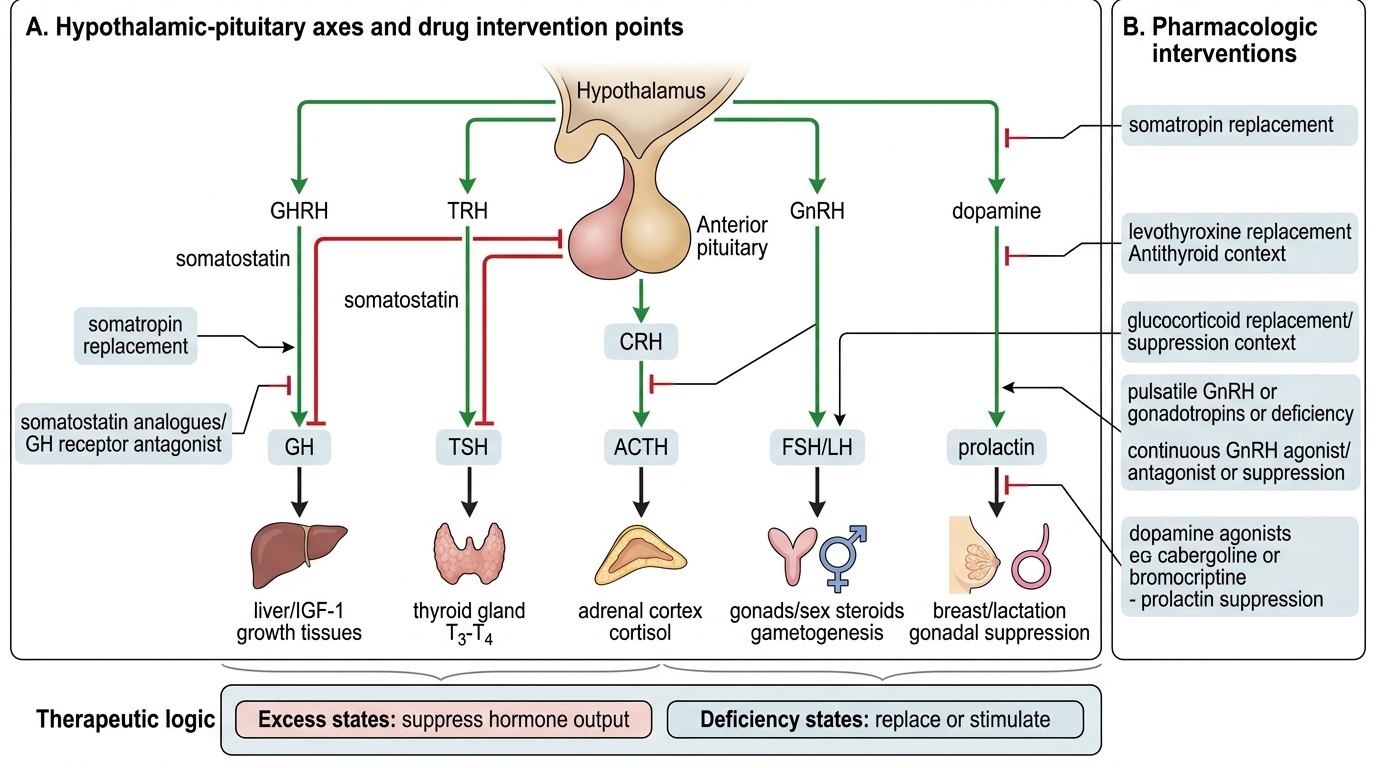
Hypothalamic-Pituitary Axes and Pharmacologic Control
Therapeutic Goals: Excess and Deficiency States
Anterior pituitary pharmacology is motivated by two fundamentally opposite pathological states: hormone excess (from pituitary tumours or ectopic production) and hormone deficiency (from pituitary destruction, surgery, or radiation). The therapeutic goal in each is opposite: excess → suppress; deficiency → replace.
Hormone excess states requiring pharmacological suppression:
- Acromegaly (GH excess): target IGF-1 normalisation and tumour control. Medical therapy is adjunctive/pre-operative or for post-surgical residual disease.
- Prolactinoma (prolactin excess): target prolactin normalisation, tumour shrinkage, and restoration of gonadal function. Medical therapy is first-line for most prolactinomas.
- Precocious puberty (premature LH/FSH secretion): target LH/FSH suppression to halt premature bone age advancement and sex development.
- Prostate cancer (androgen-sensitive): target testosterone suppression via LH suppression — castration level testosterone (<50 ng/dL).
Hormone deficiency states requiring replacement or stimulation:
- GH deficiency in children: recombinant GH (somatropin) SC daily.
- Hypogonadotropic hypogonadism (infertility): gonadotropin injections (FSH/LH/hCG) stimulate gonadal function; or pulsatile GnRH pump.
- Adrenal insufficiency (ACTH deficiency): tetracosactide (Synacthen test) for diagnosis; ACTH itself not commonly used for replacement (prefer cortisol directly).
Drug choice is guided by: the specific hormone axis, the goal (stimulate vs suppress), the patient's condition (pregnancy, cancer), and the available formulation (SC injection, depot, IV).
SELF-CHECK
A 32-year-old woman with a prolactin-secreting pituitary adenoma (microprolactinoma) has galactorrhoea and amenorrhoea. Prolactin is 280 ng/mL. First-line treatment is:
A. A. Transphenoidal surgery
B. B. Octreotide (somatostatin analogue)
C. C. Cabergoline (dopamine agonist)
D. D. Radiotherapy
Reveal Answer
Answer: C. C. Cabergoline (dopamine agonist)
Cabergoline is first-line for prolactinomas — medical therapy with a dopamine agonist normalises prolactin in >80% of cases and reduces tumour size in >60%. Cabergoline is preferred over bromocriptine (fewer ADRs, once/twice weekly dosing, higher efficacy). Surgery is reserved for macroprolactinomas causing mass effect that fail medical therapy, or patients who cannot tolerate dopamine agonists. Octreotide suppresses GH (acromegaly), not prolactin significantly. Radiotherapy is used for resistant/aggressive tumours as adjuvant.
Drug Classification: Agonists, Antagonists, and Analogues
Anterior pituitary modulators are pharmacologically diverse — they include receptor agonists, receptor antagonists, hormone analogues, and recombinant hormone replacements. A clear classification by the hormone axis they target provides the conceptual framework.
Somatostatin Analogues (SSAs): Octreotide, lanreotide, pasireotide. Natural somatostatin has a 2-minute half-life; SSAs have extended half-lives (octreotide 1.7 hours; long-acting release (LAR) formulations: monthly depot injection). Mechanism: bind somatostatin receptors (SSTR2, SSTR5) on pituitary somatotrophs → inhibit GH release. Also suppress insulin, glucagon, GI peptides, and gut motility. Uses: acromegaly, carcinoid syndrome, VIPoma, GI bleeding (variceal). ADRs: GI symptoms (nausea, steatorrhoea, cholelithiasis — reduced gallbladder motility), bradycardia, glucose dysregulation.
Dopamine Agonists: Bromocriptine (short half-life, twice daily), cabergoline (long half-life, once or twice weekly). Mechanism: activate D2 receptors on lactotrophs → inhibit prolactin secretion; activate D2 on somatotrophs in acromegaly → paradoxical GH suppression. Uses: hyperprolactinaemia (primary), prolactinoma (medical management), acromegaly (adjunct), Parkinson's disease (bromocriptine). Preferred agent: cabergoline — superior efficacy, better tolerability, less nausea, weekly dosing. ADRs: nausea/vomiting (start at low dose), postural hypotension, nasal congestion; high-dose cabergoline (Parkinson's doses) — cardiac valvular fibrosis (rare at prolactinoma doses).
GnRH Analogues (Leuprolide, Goserelin, Triptorelin): Synthetic GnRH agonist analogues that are more potent than native GnRH and resistant to degradation. Key paradox: pulsatile native GnRH → LH/FSH stimulation. Continuous GnRH analogue → initial LH/FSH surge (first 1–2 weeks) → receptor downregulation → LH/FSH suppression (castration levels). Uses of continuous (suppressive) use: prostate cancer (chemical castration), endometriosis, uterine fibroids, precocious puberty. Uses of pulsatile administration: hypogonadotropic hypogonadism (fertility treatment). ADRs (suppressive use): hot flushes, osteoporosis, erectile dysfunction, libido loss, mood changes. Initial GH/testosterone flare: add anti-androgen (bicalutamide) for the first 4 weeks in prostate cancer.
GH Receptor Antagonist — Pegvisomant: Modified GH molecule with altered structure that binds but does not activate the GH receptor — competitive antagonist. Does NOT lower GH levels (GH feedback is lost → GH may rise) but lowers IGF-1 (the clinically meaningful endpoint for acromegaly). Used in acromegaly refractory to SSAs or surgery. Monitor hepatic enzymes (hepatotoxicity concern).
Recombinant Gonadotropins and GH: Recombinant FSH (follitropin), LH, hCG for ovarian stimulation and infertility. Recombinant GH (somatropin) for GH deficiency in children and adults. Tetracosactide (Synacthen): synthetic ACTH(1-24) — used in the short Synacthen test for adrenal insufficiency diagnosis; can also treat infantile spasms (West syndrome).