Page 12 of 36
PH7.4 | PH7.4 | Anterior Pituitary Hormone Modulators — SDL Guide — SDL Guide (Part 2)
Per-Drug-Class PK, PD, Uses, and ADRs
Each drug class in anterior pituitary pharmacology has distinctive pharmacokinetic properties that determine formulation choice and monitoring needs.
Provided image
Octreotide: Half-life ~1.7 hours (SC); octreotide LAR (long-acting release) is a monthly depot injection that maintains steady-state levels — preferred for chronic acromegaly management. Excreted mostly in bile; dose reduction in hepatic impairment. Normalises IGF-1 in 50–65% of acromegaly patients in clinical studies. For acute GI variceal bleeding: IV infusion.
Lanreotide (Somatuline): Another LAR somatostatin analogue; autogel formulation — SC deep injection every 4 weeks. Comparable efficacy to octreotide LAR for acromegaly.
Cabergoline: Oral, metabolised hepatically, half-life 63–68 hours — once or twice weekly dosing. Preferred over bromocriptine for prolactinoma (higher normalisation rate, better tolerability). Less first-pass than bromocriptine. Start low (0.25 mg twice weekly), titrate up to 3 mg/week. Achieves prolactin normalisation in 80–85% and tumour shrinkage in >60–70% of prolactinomas.
Leuprolide: Available as daily SC injection, monthly depot, or 3-monthly depot. After initial LH/FSH surge (1–2 weeks), sustained administration downregulates pituitary GnRH receptors → suppressed FSH/LH → castrate testosterone in men (used for prostate cancer) or suppressed oestrogen/progesterone in women (endometriosis, fibroids). For precocious puberty: monthly depot → arrested pubertal progression + bone maturation.
Pegvisomant: Daily SC injection. Uniquely lowers IGF-1 without lowering GH (feedback loop lost, GH may increase). Monitor: IGF-1 (treatment target), liver enzymes. Used in SSA-refractory or SSA-intolerant acromegaly.
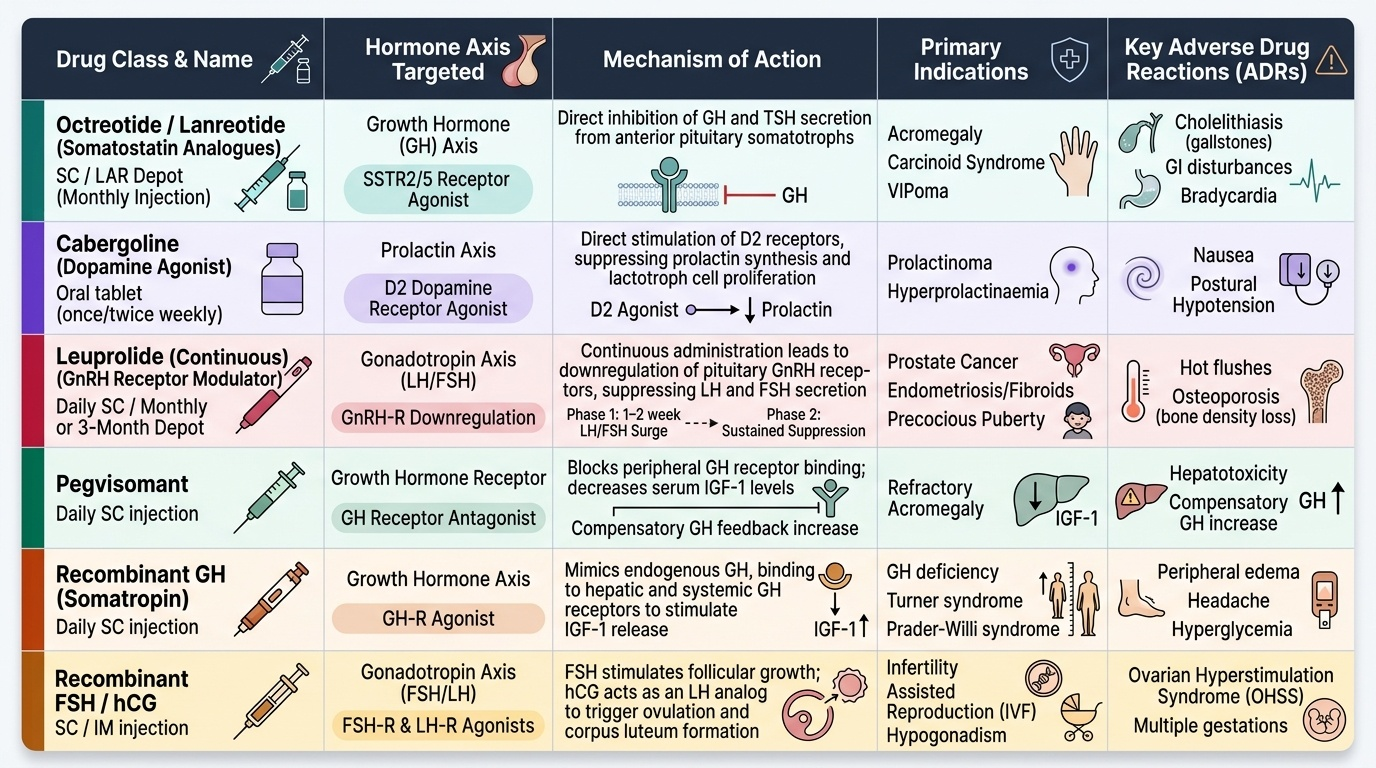
| Drug | Axis | Mechanism | Primary Indication | Key ADRs |
|---|---|---|---|---|
| Octreotide/Lanreotide | GH (SSTR2/5) | Inhibit GH secretion | Acromegaly, carcinoid, VIPoma | Cholelithiasis, GI, bradycardia |
| Cabergoline | Prolactin (D2) | Inhibit prolactin secretion | Prolactinoma, hyperprolactinaemia | Nausea, postural hypotension |
| Leuprolide (continuous) | LH/FSH (GnRH-R downreg.) | Suppress LH/FSH | Prostate cancer, endometriosis, precocious puberty | Hot flushes, osteoporosis |
| Pegvisomant | GH-R antagonist | Block GH action → ↓ IGF-1 | Refractory acromegaly | Hepatotoxicity, GH rise |
| Recombinant GH | GH-R agonist | Replace GH | GH deficiency (children/adults) | Oedema, headache, glucose↑ |
| Recombinant FSH/hCG | FSH-R/LH-R | Stimulate gonadal function | Infertility | OHSS (ovarian hyperstimulation) |
CLINICAL PEARL
Pegvisomant does NOT lower GH — and that is by design. Students often confuse monitoring endpoints: for SSAs (octreotide), the endpoint is both GH normalisation AND IGF-1 normalisation. For pegvisomant, the endpoint is IGF-1 alone — GH levels often rise (because negative feedback via IGF-1 is blocked). Monitoring: IGF-1 is the clinical measure; GH rising is expected. Separately: the leuprolide flare effect in prostate cancer is clinically dangerous — the initial testosterone surge (2 weeks) can worsen bone pain or cause spinal cord compression if metastases present. Standard practice: co-administer an anti-androgen (bicalutamide) for the first 4 weeks to block the flare.
SELF-CHECK
A patient with acromegaly is started on pegvisomant. Three months later, GH levels have risen from 12 to 28 ng/mL but IGF-1 has normalised. The most appropriate interpretation is:
A. A. Drug failure — GH is still elevated; switch to octreotide
B. B. Expected response — pegvisomant lowers IGF-1 (the treatment target), not GH; GH rise reflects lost negative feedback
C. C. Pituitary tumour progression — urgent MRI required
D. D. Dose of pegvisomant is too low — increase immediately
Reveal Answer
Answer: B. B. Expected response — pegvisomant lowers IGF-1 (the treatment target), not GH; GH rise reflects lost negative feedback
Pegvisomant is a GH receptor antagonist that blocks GH action, reducing IGF-1 production. Because IGF-1 is reduced, the negative feedback on the pituitary is also reduced, allowing GH secretion to increase. The treatment endpoint is IGF-1 normalisation, not GH suppression. This is expected pharmacology, not drug failure. GH rise alone without rising IGF-1 is not a criterion for escalation. Annual MRI is appropriate monitoring for pituitary tumour growth, but rising GH on pegvisomant is a known phenomenon, not evidence of progression.
Clinical Decision-Making: Acromegaly, Prolactinoma, and Hypogonadism
Anterior pituitary pharmacology comes together in the management of three key clinical conditions. Each follows a logical treatment hierarchy based on mechanism and evidence.
Acromegaly management:
First-line definitive treatment is transsphenoidal surgery (cure rate 60–80% for microadenoma, lower for macroadenoma). Medical therapy is used: (a) pre-operatively to shrink tumour and improve surgical outcomes (SSA for 3–6 months), (b) post-operatively if surgery is incomplete or GH/IGF-1 remains elevated, (c) as primary medical therapy in patients unfit for surgery or refusing it. First-line medical: SSAs (octreotide LAR or lanreotide autogel monthly). If SSA insufficient: add cabergoline (adjunct, modest additional effect) or switch to pegvisomant (refractory cases). Radiotherapy (stereotactic radiosurgery) is third-line, with delayed effect (years).
Prolactinoma management:
Contrast acromegaly — dopamine agonists are FIRST-LINE for prolactinoma, not surgery. Cabergoline is preferred (>80% prolactin normalisation; >60% tumour shrinkage). In microprolactinoma: medical therapy alone for 2–3 years; many achieve remission. In macroprolactinoma: medical therapy reliably shrinks the tumour (better than surgery for most). Surgery is reserved for mass effect not responding to medical therapy, cabergoline failure, or patient preference. In pregnancy: usually stop dopamine agonist unless macroprolactinoma enlarging.
Precocious puberty and prostate cancer (GnRH analogues):
- Precocious puberty (central, GnRH-dependent): leuprolide or triptorelin monthly depot → sustained GnRH receptor desensitisation → arrested puberty; continued until appropriate pubertal age. Bone age monitored (prevent premature epiphyseal fusion).
- Prostate cancer: leuprolide or goserelin monthly/3-monthly depot → chemical castration (testosterone <50 ng/dL). Standard in locally advanced/metastatic prostate cancer; combined with anti-androgens (bicalutamide) initially to prevent flare. Monitoring: PSA response, testosterone levels, bone density (long-term).
Self-Assessment: Pituitary Drug Scenarios
Apply your understanding of anterior pituitary pharmacology to these two scenarios:
Scenario A: A 45-year-old man with a GH-secreting pituitary macroadenoma undergoes transsphenoidal surgery, but post-operative GH is still 8.2 ng/mL (normal <1 ng/mL) and IGF-1 remains elevated. What is the next pharmacological step? What if this first-line pharmacological step achieves only 40% IGF-1 reduction after 6 months?
Answer: First-line medical therapy: octreotide LAR or lanreotide autogel (SSA monthly injection). If SSA response is partial (IGF-1 not normalised): add cabergoline (10–20% additional response) or switch to pegvisomant (GH receptor antagonist — lowers IGF-1 even when GH remains elevated; second-line for SSA-resistant acromegaly). Monitor: IGF-1 (target normalisation), annual MRI, glucose (SSAs can worsen glycaemia).
Scenario B: A 28-year-old woman wants to conceive. She has hypogonadotropic hypogonadism (low FSH, LH, and oestrogen; thin endometrium). How do you use a GnRH analogue to help her conceive — and how does this differ from its use in prostate cancer? Answer: For fertility in hypogonadotropic hypogonadism: use pulsatile GnRH (via a programmable pump, SC, every 60–90 minutes) — this mimics normal hypothalamic GnRH pulsatility, stimulating pituitary FSH/LH release and then ovarian folliculogenesis. Alternatively: exogenous recombinant FSH/LH injections. Contrast with prostate cancer: continuous leuprolide depot — sustained GnRH receptor stimulation → downregulation → FSH/LH suppression → testosterone castration. Same drug class, opposite dosing pattern, opposite hormonal effect.
SELF-CHECK
Why does continuous leuprolide administration suppress LH and FSH, while pulsatile GnRH administration stimulates them?
A. A. Leuprolide is a GnRH antagonist; pulsatile GnRH is an agonist
B. B. Continuous GnRH agonist overwhelms the normal pulsatile signal, downregulating GnRH receptors on gonadotrophs; pulsatile dosing mimics physiological GnRH release, maintaining receptor sensitivity
C. C. Leuprolide suppresses LH/FSH because it is a long-acting form that is metabolised differently
D. D. The pituitary only responds to GnRH when it is given IV
Reveal Answer
Answer: B. B. Continuous GnRH agonist overwhelms the normal pulsatile signal, downregulating GnRH receptors on gonadotrophs; pulsatile dosing mimics physiological GnRH release, maintaining receptor sensitivity
Leuprolide is a GnRH AGONIST, not antagonist — the suppression is pharmacodynamic. GnRH receptors on anterior pituitary gonadotrophs are physiologically tuned to respond to PULSATILE input. Continuous stimulation with a potent, long-acting GnRH agonist overwhelms this system, causing receptor internalisation and desensitisation — gonadotrophs stop responding, and LH/FSH fall to castrate levels after 2–4 weeks. Pulsatile GnRH (from a pump) mimics physiological hypothalamic pulsatility and maintains receptor responsiveness. This pharmacodynamic principle — agonist-induced receptor downregulation — also applies to beta-agonists in asthma with overuse.