Page 14 of 36
PH7.5 | PH7.5 | Corticosteroid Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Classify corticosteroids by glucocorticoid and mineralocorticoid potency with comparative potency values
- Describe the mechanism of glucocorticoid action at the receptor and nuclear level
- Enumerate the systemic adverse effects of prolonged corticosteroid use across body systems
- Match the appropriate corticosteroid to specific clinical indications
- Communicate to a patient the appropriate use of corticosteroids including safe tapering and sick-day rules
INSTRUCTIONS
Corticosteroids are among the most powerful anti-inflammatory drugs available — and among the most misused. From asthma inhalers to IV methylprednisolone for SLE flares, from dexamethasone in cerebral oedema to hydrocortisone for adrenal crisis, steroids span every clinical specialty. Their adverse effects, when unrecognised, cause Cushingoid obesity, osteoporotic fractures, diabetes, and life-threatening adrenal insufficiency on abrupt withdrawal. Understanding their rational use and the patient communication required is a core NMC competency.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 20 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 42 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old woman with rheumatoid arthritis has been on prednisolone 10 mg daily for 3 years. She now presents with a vertebral fracture, new-onset type 2 diabetes, and a moon face. Her morning cortisol is undetectable. She forgot to take her prednisolone before a recent gastroenteritis episode and was brought to emergency with a hypotensive crisis. These four complications — osteoporosis, steroid diabetes, Cushing's syndrome, and adrenal insufficiency crisis — are all predictable, preventable consequences of long-term corticosteroid therapy. Do you know how to prescribe steroids with a plan to prevent them, and how to communicate the risk to your patients?
WHY THIS MATTERS
Corticosteroids are prescribed across virtually every clinical specialty — rheumatology, respiratory, nephrology, oncology, gastroenterology, dermatology, emergency medicine, and intensive care. Despite their ubiquity, steroid-related adverse effects generate enormous preventable morbidity. Every prescriber needs to know: the difference in potency between dexamethasone and prednisolone; why steroids should never be stopped abruptly after long-term use; how to prophylactically prescribe bisphosphonates and PPIs when initiating chronic steroids; and how to communicate the essential 'steroid card' information to a patient. NMC PH7.5 specifically mandates competency in patient communication about steroid use.
RECALL
The HPA (hypothalamic–pituitary–adrenal) axis maintains homeostasis of glucocorticoid levels. CRH (corticotropin-releasing hormone) from the hypothalamus stimulates ACTH release from pituitary corticotrophs → ACTH stimulates adrenal fasciculata to synthesise and release cortisol → cortisol exerts negative feedback on both the hypothalamus and pituitary. Normal cortisol secretion follows a circadian pattern: peak at 6–8 AM, nadir at midnight. Cortisol's physiological roles are broad: (1) metabolic: gluconeogenesis, lipolysis, protein catabolism; (2) anti-inflammatory: inhibits phospholipase A2 (via lipocortin/annexin A1), reduces cytokine production; (3) mineralocorticoid: sodium retention and potassium excretion (at high concentrations); (4) permissive: sensitises tissues to catecholamines (critical for cardiovascular response to stress). When exogenous glucocorticoids are administered long-term, the negative feedback suppresses endogenous ACTH production → adrenal cortex atrophies → on abrupt withdrawal, there is no cortisol reserve for stress → acute adrenal insufficiency.
Glucocorticoid Physiology: HPA Axis and Cortisol Effects
The fundamental pharmacological property of glucocorticoids — anti-inflammatory power — is an amplification of one of cortisol's physiological roles. In physiological concentrations, cortisol constrains the immune response, prevents overshooting inflammation during infection or injury, and maintains vascular tone. When administered pharmacologically at supraphysiological doses, this anti-inflammatory effect becomes therapeutic — suppressing pathological inflammation in autoimmune diseases, allergies, and organ transplant rejection.
Key pharmacological consequences of pharmacological GC use that reflect their physiological roles:
Metabolic effects (amplified gluconeogenesis): elevated blood glucose → steroid-induced diabetes. Protein catabolism → proximal myopathy (wasting of limb girdle muscles). Fat redistribution → central obesity, moon face, buffalo hump (Cushing's phenotype).
Anti-inflammatory mechanisms: GCs bind the intracellular glucocorticoid receptor (GR) in the cytoplasm → GR-GC complex translocates to the nucleus. Nuclear effects: (1) Transactivation — upregulates anti-inflammatory genes including lipocortin/annexin A1 (inhibits phospholipase A2 → blocks arachidonic acid cascade → less prostaglandins and leukotrienes); (2) Transrepression — blocks pro-inflammatory transcription factors NF-κB and AP-1, preventing cytokine gene transcription (IL-1, IL-6, TNF-α, COX-2).
Mineralocorticoid receptor cross-reactivity: Cortisol and hydrocortisone bind both GR and MR (mineralocorticoid receptor) — causing sodium and water retention, potassium excretion, hypertension, and oedema. Synthetic GCs (dexamethasone, betamethasone) have negligible MR affinity — no sodium retention, preferred where fluid retention is problematic.
Therapeutic Goals: Anti-inflammation, Replacement, and Targeted Use
Corticosteroid therapy serves two fundamentally different goals that require different drugs and doses: physiological replacement and pharmacological anti-inflammatory suppression.
Physiological replacement (Addison's disease, CAH, hypopituitarism): The goal is to replace the deficient cortisol at physiological doses — approximately 15–25 mg hydrocortisone equivalent per day. Both a glucocorticoid (hydrocortisone or prednisolone) and a mineralocorticoid (fludrocortisone, 0.1 mg/day) are needed for primary adrenal insufficiency (Addison's). Secondary adrenal insufficiency (ACTH deficiency) — only glucocorticoid needed (aldosterone is regulated by RAAS, not ACTH). Replacement doses do NOT cause Cushing's features, growth retardation, or HPA suppression because they mirror physiological levels.
Pharmacological (supraphysiological) use — anti-inflammatory, immunosuppressive: Doses many times higher than physiological: prednisolone 30–60 mg/day for autoimmune disease; IV methylprednisolone 500–1000 mg 'pulse' in SLE or MS relapse; dexamethasone 16 mg/day in cerebral oedema. The trade-off: potent therapeutic effect vs cumulative dose-dependent adverse effects.
Targeted/local use reduces systemic exposure: Inhaled corticosteroids (ICS — beclometasone, fluticasone, budesonide) for asthma; topical steroids for skin; intra-articular steroids for joints; epidural for radiculopathy. Local delivery achieves high drug concentration at the site with minimal systemic absorption — reducing systemic ADRs but not eliminating them (especially with high-potency topicals or swallowed ICS).
SELF-CHECK
A patient with cerebral oedema from a brain tumour needs a corticosteroid. Which drug is most appropriate and why?
A. A. Prednisolone — most commonly available steroid
B. B. Hydrocortisone — high anti-inflammatory potency
C. C. Dexamethasone — high glucocorticoid potency, negligible mineralocorticoid activity (no sodium/water retention)
D. D. Fludrocortisone — strongest mineralocorticoid available
Reveal Answer
Answer: C. C. Dexamethasone — high glucocorticoid potency, negligible mineralocorticoid activity (no sodium/water retention)
Dexamethasone is specifically preferred for cerebral oedema because: (1) very high glucocorticoid potency (~25–30× hydrocortisone equivalent), requiring a low dose; (2) negligible mineralocorticoid activity — does not cause sodium and water retention, which would worsen cerebral oedema; (3) excellent CNS penetration. Prednisolone has moderate mineralocorticoid activity. Hydrocortisone has the HIGHEST mineralocorticoid activity among common GCs — contraindicated where fluid retention is dangerous. Fludrocortisone is purely a mineralocorticoid used in Addison's disease, not for anti-inflammatory purposes.
Classification: Glucocorticoids and Mineralocorticoids
Corticosteroids are classified by their primary receptor activity (glucocorticoid vs mineralocorticoid) and by their duration of action — both determine drug selection for specific indications.
The reference standard is hydrocortisone (cortisol) = GC potency 1.0, MC potency 1.0. All other corticosteroids are compared to this reference. Increasing fluorination and other structural modifications enhance GC receptor affinity while reducing MC receptor affinity in synthetic agents.
Glucocorticoids (classified by duration):
- Short-acting (6–12 hours): Hydrocortisone (GC: 1, MC: 1), cortisone (GC: 0.8, MC: 0.8) — high mineralocorticoid activity; used in adrenal replacement and emergency IV dosing.
- Intermediate-acting (12–36 hours): Prednisolone (GC: 4, MC: 0.8) — most widely used for chronic inflammatory diseases; methylprednisolone (GC: 5, MC: 0.5) — available IV (pulse therapy in SLE/MS), less mineralocorticoid than prednisolone; triamcinolone (GC: 5, MC: 0) — predominantly local use (intra-articular, inhaled).
- Long-acting (36–54 hours): Dexamethasone (GC: 25–30, MC: negligible) — preferred for cerebral oedema, anti-emetic, dexamethasone suppression test (Cushing's diagnosis), COVID-19 (RECOVERY trial); betamethasone (GC: 25–30, MC: negligible) — prenatal lung maturation (promotes surfactant production in preterm fetus).
Mineralocorticoids:
- Fludrocortisone (GC: 10, MC: 125–150) — the most potent available MC; used as replacement in primary adrenal insufficiency (Addison's) and CAH (congenital adrenal hyperplasia). Not used for its weak GC activity.
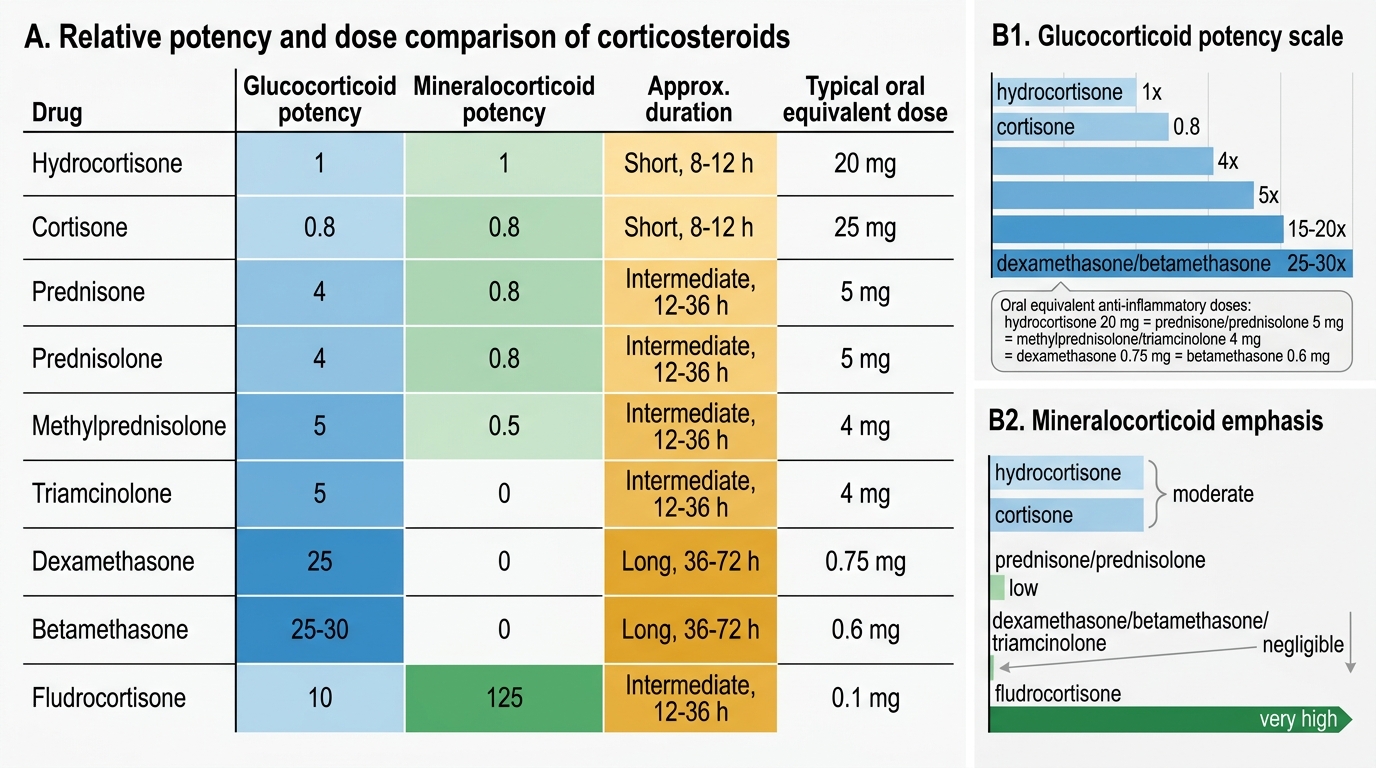
Relative Potency of Common Corticosteroids