Page 15 of 36
PH7.5 | PH7.5 | Corticosteroid Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Pharmacology: Mechanisms, PK, and Clinical Uses
The glucocorticoid receptor (GR) belongs to the nuclear receptor superfamily of transcription factors. In the resting state, GR is sequestered in the cytoplasm bound to heat shock proteins (HSP90). Drug entry into the cell (GCs are lipophilic — passive diffusion through cell membrane) → binding to cytoplasmic GR → conformational change → GR-GC complex dissociates from HSP90 → translocates to the nucleus. In the nucleus: (1) Transactivation: GR-GC complex binds glucocorticoid response elements (GREs) in DNA → upregulates anti-inflammatory proteins including lipocortin-1 (annexin A1), which inhibits phospholipase A2 — the key enzyme releasing arachidonic acid from cell membranes (the starting material for prostaglandins and leukotrienes). Also upregulates IκB (inhibitor of NF-κB). (2) Transrepression: GR-GC tethers to and prevents the DNA binding of NF-κB and AP-1 → blocks transcription of pro-inflammatory genes: IL-1, IL-2, IL-6, TNF-α, COX-2, iNOS, chemokines. This dual nuclear mechanism explains the broad anti-inflammatory and immunosuppressive spectrum of GCs.
Pharmacokinetics: Oral bioavailability is generally high (>80% for prednisolone, methylprednisolone). Hepatic first-pass: prednisone → prednisolone (active) by 11β-HSD. Hepatic metabolism (CYP3A4) — rifampicin/phenytoin induce metabolism → dose increase needed. Protein binding: cortisol binds cortisol-binding globulin (CBG). Renal excretion of metabolites.
Major clinical uses:
- Replacement: Addison's disease — hydrocortisone 15–25 mg/day (given AM) + fludrocortisone 0.1 mg/day; adrenal crisis — IV hydrocortisone 100 mg stat then infusion.
- Rheumatology/Autoimmune: SLE, RA, dermatomyositis, polymyalgia rheumatica — prednisolone oral; SLE flare — IV methylprednisolone pulse.
- Respiratory: Asthma (inhaled ICS daily; systemic for severe attack); COPD exacerbation (prednisolone 40 mg × 5 days).
- Neurology: Cerebral oedema — dexamethasone 4 mg 6-hourly; MS relapse — methylprednisolone IV; meningitis — dexamethasone reduces neurological sequelae.
- Oncology: Anti-emetic (dexamethasone); lymphoma/leukaemia (cytotoxic component).
- Obstetrics: Betamethasone IM at 24–34 weeks gestation to accelerate fetal lung maturation (surfactant induction).
- Organ transplant: Immunosuppression.
- COVID-19 (RECOVERY trial): Dexamethasone 6 mg daily × 10 days reduces mortality in patients on respiratory support.
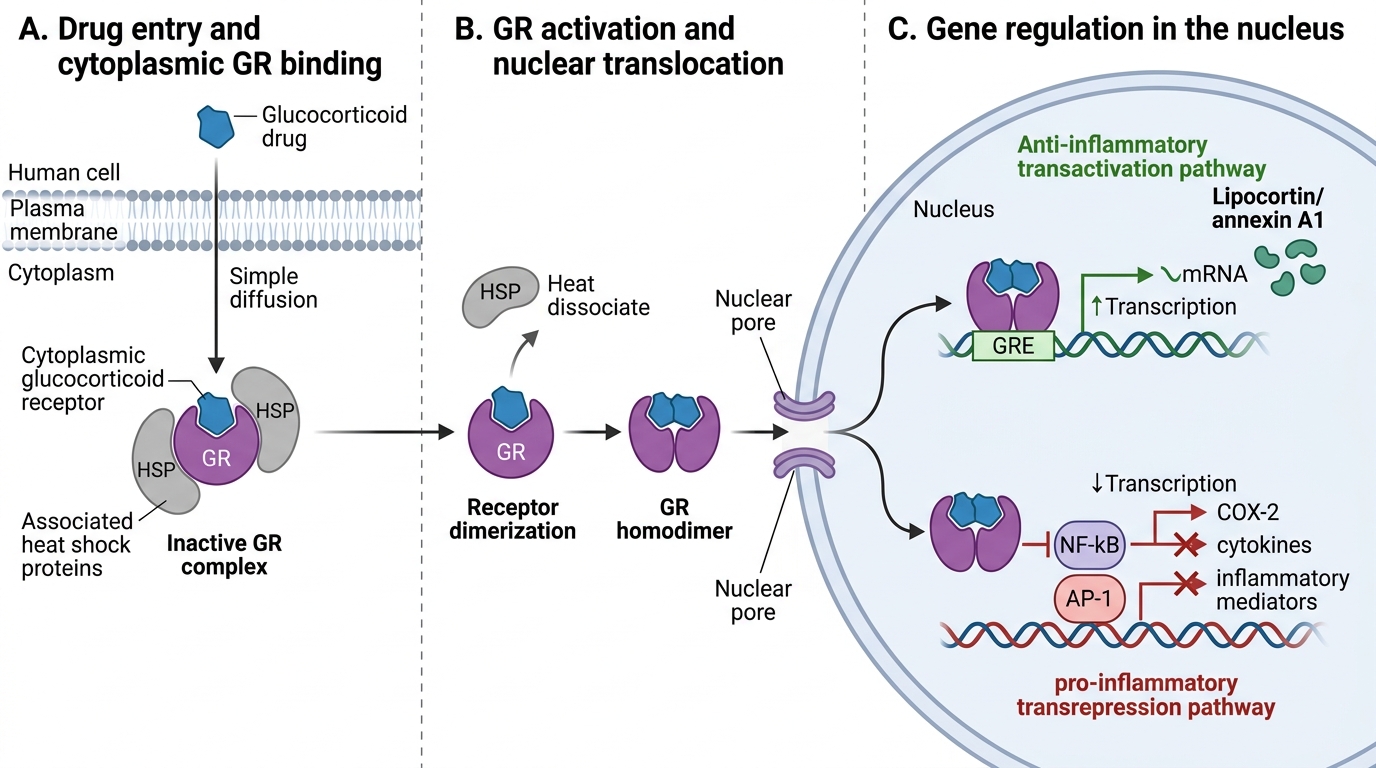
Glucocorticoid Receptor Nuclear Pathway
Adverse Effects, Contraindications, and Patient Communication
Long-term systemic corticosteroid use produces a characteristic syndrome of adverse effects across multiple organ systems. Recognition, prevention, and monitoring of these effects are as important as the therapeutic use itself.
Metabolic: Hyperglycaemia (steroid-induced diabetes) — due to GC-stimulated gluconeogenesis and insulin resistance; monitor fasting glucose and HbA1c; manage with oral agents or insulin if needed. Dyslipidaemia — elevated triglycerides, LDL. Weight gain and central obesity.
Musculoskeletal: Glucocorticoid-induced osteoporosis (GIO) — most common preventable ADR of chronic steroid use; prednisolone >7.5 mg/day for >3 months: initiate bisphosphonate (alendronate) + calcium + vitamin D prophylaxis. Proximal myopathy — wasting of shoulder and pelvic girdle muscles (difficulty climbing stairs, rising from chair); reversed on dose reduction. Avascular necrosis of femoral head (rare but serious).
Endocrine: HPA axis suppression — after >3 weeks of systemic steroids, the hypothalamus and pituitary cannot mount an ACTH response to stress; abrupt withdrawal → adrenal insufficiency crisis (Addisonian crisis). Taper any course >3 weeks. Patients on long-term steroids need 'stress dosing' (double/triple dose) during surgery, fever, or serious illness. Cushing's syndrome (iatrogenic) — moon face, central obesity, striae, easy bruising, buffalo hump. Growth retardation in children on long-term systemic steroids.
Immune: Increased susceptibility to infections — bacterial, fungal (especially oral candidiasis with inhaled steroids), viral (reactivation of TB, herpes zoster, strongyloidiasis). Screen for latent TB before starting long-term steroids. Impaired wound healing.
GI: Peptic ulcer disease — steroids alone have modest ulcerogenic risk, but combined with NSAIDs the risk is substantially higher; prescribe PPI prophylaxis. Pancreatitis (rare).
Ocular: Posterior subcapsular cataracts (bilateral, with prolonged use). Raised intraocular pressure → steroid-induced glaucoma; patients on topical or systemic steroids need IOP monitoring.
CNS/Psychiatric: Euphoria, insomnia, mood swings, psychosis (especially at high doses). Pseudotumour cerebri on withdrawal.
Patient communication: Every patient on steroids >2 weeks should receive a steroid card (or bracelet) stating: 'Do not stop this medication suddenly. In illness or before surgery, tell your doctor you are on steroids.' Counsel on: taking with food (reduces GI effects), not missing doses, recognising infection symptoms, and what to do in emergency (double dose during fever/stress, go to hospital for adrenal crisis symptoms — weakness, dizziness, vomiting).
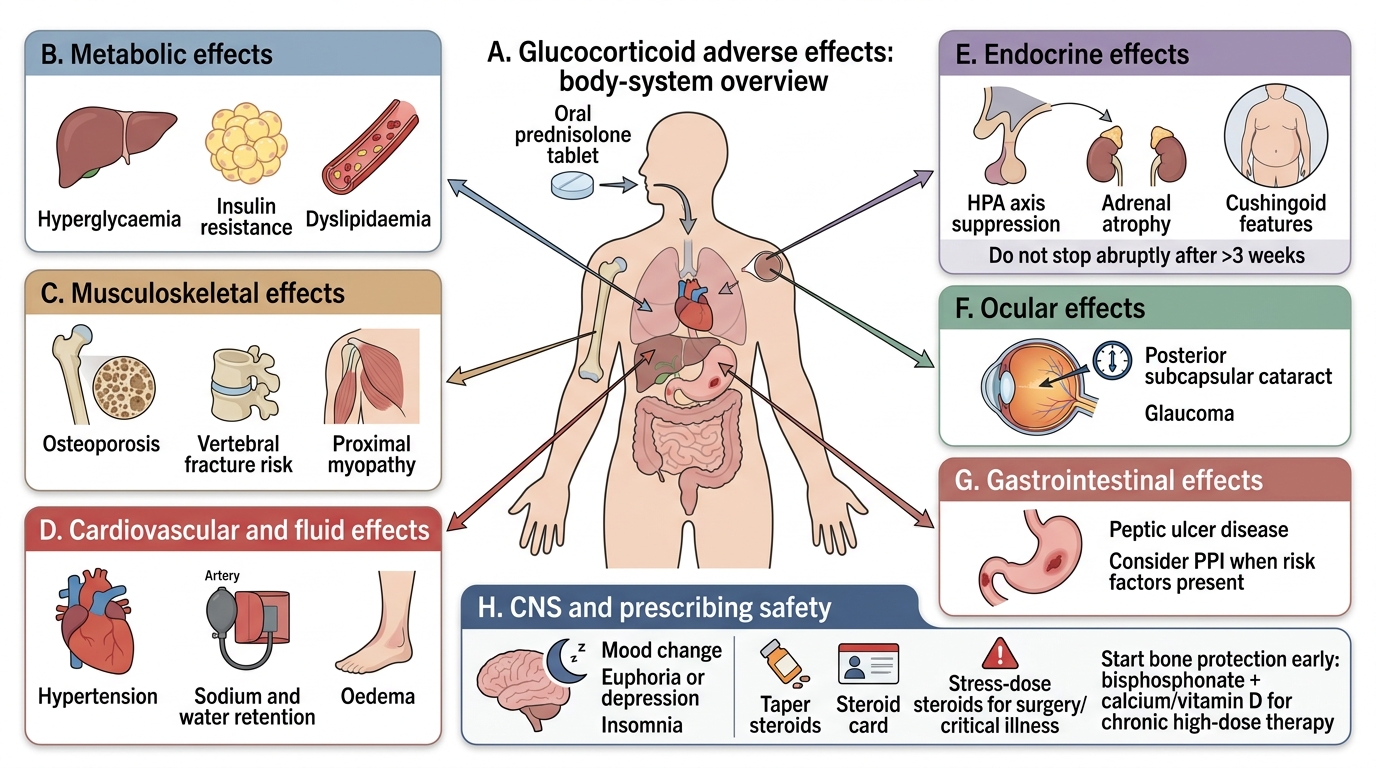
Systemic Adverse Effects of Glucocorticoids
CLINICAL PEARL
Two preventable disasters from corticosteroid prescribing: First: never stop prednisolone abruptly after >3 weeks of use — the adrenal gland has atrophied under suppression and cannot mount a cortisol stress response. A patient who stops steroids before emergency surgery and is not given stress doses can die from Addisonian crisis. Always taper, and always give a steroid card. Second: initiate bisphosphonate prophylaxis from day one of chronic steroid prescriptions (prednisolone >7.5 mg/day, intended for >3 months) — GIO develops quickly (first 3–6 months) and is preventable. Waiting until a fracture occurs is a prescribing failure.
SELF-CHECK
A 40-year-old patient with SLE is started on prednisolone 30 mg daily. Which of the following preventive measures should be initiated concurrently?
A. A. Bisphosphonate, PPI, and calcium/vitamin D supplementation
B. B. PPI alone (main risk is peptic ulcer)
C. C. Calcium/vitamin D alone (no bisphosphonate at this age)
D. D. No prophylaxis needed until adverse effects appear
Reveal Answer
Answer: A. A. Bisphosphonate, PPI, and calcium/vitamin D supplementation
When initiating long-term high-dose steroids: (1) bisphosphonate (alendronate) + calcium/vitamin D — prevent glucocorticoid-induced osteoporosis (GIO); bone loss is fastest in the first 6 months, so prophylaxis must start at initiation, not after fracture. Age 40 is NOT a barrier to bisphosphonate prophylaxis in GIO — the fracture risk from 30 mg prednisolone is significant regardless of age. (2) PPI prophylaxis — steroid alone has modest GI risk, but the combination with any NSAID or aspirin (common in SLE/RA patients) substantially increases peptic ulcer risk. (3) Monitor glucose (steroid diabetes), BP, and IOP. No preventive measures is a prescribing error.
Clinical Decision-Making: Selecting the Right Steroid for the Right Indication
Rational corticosteroid prescribing matches the drug's potency, mineralocorticoid activity, and duration to the clinical need, while minimising systemic exposure.
Acute severe scenarios:
- Adrenal crisis (Addisonian crisis): IV hydrocortisone 100 mg immediately (stat), then 50–100 mg 6-hourly; switch to oral once stable; add fludrocortisone 0.1 mg/day for primary adrenal insufficiency. Do not delay treatment — this is life-threatening.
- Anaphylaxis: IV hydrocortisone 200 mg as secondary drug (slow onset; adrenaline is the first-line drug).
- Acute severe asthma: IV/IM hydrocortisone 100–200 mg stat; oral prednisolone 40 mg/day for 5–7 days.
- Cerebral oedema: Dexamethasone 8–16 mg loading dose → 4 mg 6-hourly; chosen specifically for negligible mineralocorticoid activity.
Chronic inflammatory disease management:
- Rheumatology (SLE, RA, polymyalgia): Prednisolone — starting dose 15–60 mg/day depending on severity; taper by 10–20% every 2–4 weeks once disease controlled. Aim for the minimum effective dose. Add DMARD (methotrexate, hydroxychloroquine) as steroid-sparing agents.
- Organ transplant: Prednisolone as part of triple immunosuppression regimen (+ tacrolimus + mycophenolate).
Tapering protocols: No single protocol, but key principles: (1) do not taper faster than the rate of disease remission; (2) rates <2.5–5 mg prednisolone per week are safer to avoid adrenal suppression; (3) check AM cortisol before the last taper steps to confirm adrenal recovery.
Inhaled corticosteroids (ICS) for asthma: Beclometasone, fluticasone, budesonide, ciclesonide. Reduce systemic exposure vs oral. Key ADRs: oral candidiasis (advise rinse mouth after inhaler), dysphonia (hoarse voice). At very high ICS doses or with oral/intranasal combination — HPA suppression possible. Step up or down ICS dose per asthma control.
Drug interactions to monitor: Rifampicin/phenytoin/carbamazepine → CYP3A4 induction → accelerated steroid metabolism → dose increase may be needed. Steroids + NSAIDs → increased PUD risk. Steroids + fluoroquinolones → increased Achilles tendon rupture risk. Steroids + SSRIs → increased psychiatric ADR risk.