Page 19 of 36
PH7.6 | PH7.6 | Androgens and Erectile Dysfunction Drugs — SDL Guide — SDL Guide (Part 2)
Erectile Dysfunction Drugs: PDE5 Inhibitors and Alternatives
Erectile dysfunction is the inability to achieve or maintain a penile erection sufficient for satisfactory sexual performance. It is highly prevalent (affecting 40–70% of men over 40 to some degree) and is a recognised independent marker of cardiovascular disease. Its pharmacological management is built around the NO/cGMP pathway.
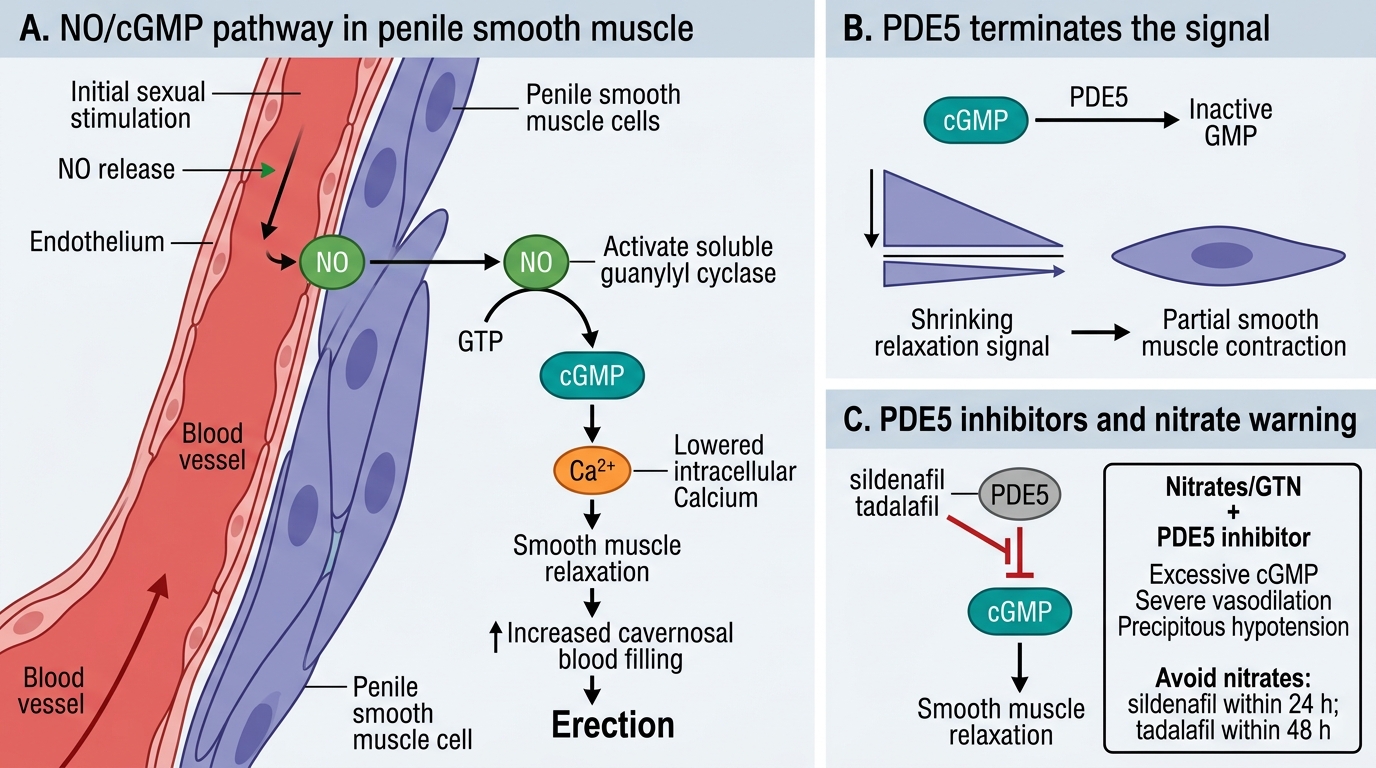
PDE5 Inhibitors (PDE5i): The first and dominant pharmacological class for ED. Sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra), avanafil (Stendra). Mechanism: These drugs selectively inhibit phosphodiesterase type 5 (PDE5), the enzyme that hydrolyses cGMP in cavernosal smooth muscle. By blocking cGMP breakdown, PDE5 inhibitors prolong and amplify the cGMP signal initiated by endogenous NO during sexual stimulation → sustained smooth muscle relaxation → prolonged erection. Key point: PDE5i are NOT pro-erectile in the absence of sexual stimulation — they amplify an existing NO signal, not create one from scratch. If the patient has no NO signalling (severe endothelial dysfunction, e.g. bilateral iliac artery disease), PDE5i may have limited effect.
Comparison of PDE5i agents:
- Sildenafil: 50–100 mg taken 30–60 minutes before sex; food (especially fatty meal) delays absorption; duration ~4–6 hours.
- Tadalafil: 10–20 mg on-demand, OR 5 mg daily (once-daily dosing — long half-life 17–36 hours allows spontaneous intercourse); taken with or without food. Also approved for BPH symptoms (combined ED+BPH indication).
- Vardenafil: 10–20 mg taken 25–60 minutes before sex; duration ~4–6 hours; slightly higher potency than sildenafil.
- Avanafil: Fastest onset (15 minutes); duration ~6 hours.
ADRs of PDE5i: headache, flushing (facial), nasal congestion, dyspepsia, visual disturbances (sildenafil — transient blue/green tinge — due to cross-inhibition of PDE6 in retinal photoreceptors), myalgia (tadalafil — more common due to long duration). Rare: priapism, non-arteritic anterior ischaemic optic neuropathy (NAION — caution in prior NAION).
CRITICAL CONTRAINDICATION — PDE5i + Nitrates: Organic nitrates (GTN, ISDN, isosorbide mononitrate) work by donating NO → increasing cGMP → vascular smooth muscle relaxation → vasodilation → reduced cardiac preload. PDE5i block cGMP breakdown. Together: massively elevated cGMP → profound vasodilation → severe, potentially fatal hypotension. ABSOLUTE CONTRAINDICATION — no exceptions: do NOT combine PDE5i with any nitrate (including short-acting GTN sprays or long-acting patches). If a patient on sildenafil needs GTN for angina, there must be a 24-hour washout (48 hours for tadalafil). This interaction is one of the most important drug-drug contraindications in clinical pharmacology.
Alternative ED drugs:
- Alprostadil (prostaglandin E1 analogue): intracavernosal injection (directly into corpora cavernosa) or intraurethral pellet (MUSE). Mechanism: PGE1 receptor activation → adenylyl cyclase → cAMP → smooth muscle relaxation. Effective even in patients with poor NO signalling. ADRs: local pain at injection site, penile fibrosis (injection), hypotension, priapism (prolonged painful erection — emergency if >4 hours).
- Apomorphine: Centrally acting dopamine D2/D3 agonist — sublingual; activates paraventricular nucleus in hypothalamus to initiate erection. Limited efficacy compared to PDE5i; ADRs: nausea, yawning. Rarely used.
NO-cGMP Pathway and PDE5 Inhibition
CLINICAL PEARL
The sildenafil-nitrate interaction is lethal and has a strict time rule. If a patient has taken sildenafil in the preceding 24 hours (or tadalafil in the preceding 48 hours) and presents with an acute coronary event requiring GTN, the nitrate is CONTRAINDICATED — the combination can cause precipitous hypotension that is unresponsive to vasopressors. This scenario is tested in clinical pharmacology OSCEs and written exams. The clinical corollary: always take a comprehensive drug history before prescribing nitrates in emergency — ask specifically about PDE5 inhibitor use. The reverse is equally important: before prescribing sildenafil, verify the patient is NOT on any chronic nitrate.
SELF-CHECK
A 55-year-old man on GTN spray (as needed) for stable angina requests sildenafil for erectile dysfunction. The correct response is:
A. A. Prescribe sildenafil 50 mg and advise him to take it 6 hours after GTN
B. B. Sildenafil is absolutely contraindicated with any nitrate — explain the hypotension risk and consider alternative ED treatment (alprostadil) or address cardiac status first
C. C. Use tadalafil instead — it has a longer half-life and less interaction with nitrates
D. D. It is safe if GTN is taken on alternate days
Reveal Answer
Answer: B. B. Sildenafil is absolutely contraindicated with any nitrate — explain the hypotension risk and consider alternative ED treatment (alprostadil) or address cardiac status first
Sildenafil (and all PDE5 inhibitors) are absolutely contraindicated with all nitrates (organic nitrates), including GTN spray, ISDN, and isosorbide mononitrate. The combination causes uncontrolled cGMP accumulation → profound vasodilation → severe hypotension that can be fatal. Tadalafil is equally contraindicated with nitrates — the class contraindication applies to all PDE5i. Alternative ED treatment that is safe in this patient: alprostadil (PGE1 mechanism, no NO/nitrate interaction). The underlying cardiac issue (requiring GTN) should also be optimally managed — revascularisation if possible may resolve both angina and the ED component related to endothelial dysfunction.
Clinical Decision-Making: Hypogonadism, BPH, and Erectile Dysfunction
Rational pharmacological management in androgen pharmacology requires integrating testosterone levels, organ involvement, comorbidities, and age.
Male hypogonadism (testosterone replacement therapy — TRT):
Indications: testosterone <300 ng/dL with symptoms (fatigue, libido loss, erectile dysfunction, reduced muscle mass, osteoporosis). Confirm on two morning measurements.
First-line: testosterone gel (transdermal) for stable levels and ease of use; IM testosterone for cost-effectiveness in India. Monitor: serum testosterone (target mid-normal range), haematocrit (polycythaemia — T stimulates erythropoietin), PSA (avoid in known prostate cancer — TRT is CONTRAINDICATED in active prostate cancer), liver enzymes, lipid profile. Bone density (DXA) baseline if osteoporosis risk.
Benign prostatic hyperplasia (BPH) pharmacotherapy:
Symptom relief: alpha-1 blockers (tamsulosin, alfuzosin, doxazosin) — relax smooth muscle in prostate and bladder neck → rapid symptom relief (1–2 weeks); ADR: postural hypotension, retrograde ejaculation. 5α-reductase inhibitors (finasteride 5 mg, dutasteride 0.5 mg) — reduce prostate volume (20–30%) after 3–6 months; best for large prostates (>40 mL); reduce PSA 50% (double PSA when screening). Combination (alpha-blocker + 5α-RI): superior to either alone in large prostates (MTOPS trial). Tadalafil 5 mg daily — also approved for BPH+ED combined indication.
Prostate cancer (androgen deprivation therapy — ADT):
GnRH agonist (leuprolide/goserelin) → chemical castration + bicalutamide for initial 4-week flare protection; then bicalutamide alone for combined blockade (combined androgen blockade/CAB). For castration-resistant prostate cancer (CRPC): enzalutamide (newer AR antagonist), abiraterone (CYP17 inhibitor blocks adrenal/intra-tumoral androgen synthesis).
ED management:
First-line: PDE5 inhibitor (sildenafil on-demand, or tadalafil 5 mg daily). Screen for organic causes (cardiovascular, diabetes, hypogonadism) and psychogenic overlay. If PDE5i fails (or contraindicated): alprostadil (intracavernosal or MUSE). If testosterone is low: testosterone replacement may partially restore erectile function. Vacuum erection device: non-pharmacological first option for some patients.
Self-Assessment: Androgen Pharmacology Scenarios
Test your applied pharmacology with these scenarios:
Scenario A: A 40-year-old man presents with fatigue, reduced libido, and BMI 32. Serum testosterone is 250 ng/dL (two morning readings). He has no prostate or cardiovascular disease. Would you prescribe TRT? What formulation and what monitoring?
Answer: Yes — symptomatic hypogonadism with confirmed low testosterone (<300 ng/dL on two readings) is an indication for TRT. Consider lifestyle modification first (weight loss improves testosterone). If TRT started: testosterone gel (daily application, steady levels) or IM testosterone enanthate (cost-effective in India). Monitor: testosterone at 3 months (target mid-normal 400–700 ng/dL), haematocrit (target <52%), PSA (baseline and 3 months), mood/libido, bone density if osteopenic.
Scenario B: A body-builder uses anabolic steroids (stanozolol) for 6 months. On examination: testicles soft and small, PSA low, testosterone low, LH/FSH undetectable. Explain the pharmacological mechanism.
Answer: Exogenous anabolic steroids provide negative feedback to hypothalamus/pituitary → GnRH/LH/FSH suppression → Leydig cells stop producing testosterone → testicular atrophy. Sertoli cells also lose FSH stimulation → impaired spermatogenesis. The paradox of anabolic steroid use: muscle grows (exogenous androgen direct effect) but endogenous testosterone drops and fertility is impaired. Recovery of the HPG axis after cessation may take 6–12 months; persistent hypogonadism may require monitoring.
SELF-CHECK
Which of the following is a correct statement about PDE5 inhibitors?
A. A. They cause erection independently of sexual stimulation
B. B. They act by blocking cGMP breakdown in cavernosal smooth muscle, thus amplifying NO-mediated relaxation during sexual stimulation
C. C. Tadalafil can be safely combined with organic nitrates due to its selectivity
D. D. Visual disturbances with sildenafil are due to CNS effects
Reveal Answer
Answer: B. B. They act by blocking cGMP breakdown in cavernosal smooth muscle, thus amplifying NO-mediated relaxation during sexual stimulation
PDE5 inhibitors block PDE5 enzyme that degrades cGMP — they amplify the cGMP signal generated by endogenous NO during sexual stimulation. They require an intact NO-triggering signal (sexual stimulation) — they do not cause erection in the absence of stimulation. Tadalafil is equally contraindicated with nitrates as sildenafil; the class contraindication applies to all PDE5i. Visual disturbances with sildenafil (blue/green tinge) are due to peripheral retinal effects — sildenafil cross-inhibits PDE6 in retinal photoreceptors, not CNS effects.