Page 21 of 36
PH7.7 | PH7.7 | Contraceptive Pharmacology — SDL Guide — SDL Guide
Learning Objectives
- Classify contraceptive methods into hormonal, non-hormonal, barrier, and emergency categories
- Describe the pharmacological mechanisms, pharmacokinetics, and adverse effects of combined oral contraceptives and progestin-only methods
- Explain the mechanism and correct timing of emergency contraceptives
- Counsel a patient on the use of female and male contraceptives including key instructions for use
- Identify absolute contraindications to combined oral contraceptive use
INSTRUCTIONS
Family planning is a cornerstone of reproductive health and maternal mortality reduction. India's National Family Planning Programme depends on clinicians who can counsel patients across the full spectrum of contraceptive options — from the daily combined pill to the 3-monthly DMPA injection and the post-coital emergency contraceptive. Understanding the pharmacological mechanisms behind each method — and the evidence-based contraindications — equips you to provide personalised, safe contraceptive counselling.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 22 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 44 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman comes for contraceptive counselling. She smokes 10 cigarettes/day and is 35 years old — she asks for the combined pill she has heard about from her friend. She is breastfeeding a 4-month-old infant. You need to advise her: Can she take the combined oral contraceptive? Why might it affect her breast milk? What is the safest alternative for a breastfeeding woman who smokes? The answers lie in the pharmacology of hormonal contraceptives — their mechanisms, their risks, and the patient-centred counselling that accompanies them.
WHY THIS MATTERS
India has over 1.3 billion people and family planning remains a national health priority. Unintended pregnancy contributes to maternal mortality through unsafe abortion and high-parity complications. Hormonal contraceptives are among the most pharmacologically sophisticated everyday drugs — combining precise mechanisms (LH surge suppression, cervical mucus modification, endometrial thinning) with a complex risk-benefit profile. The NMC competency PH7.7 explicitly requires you to explain contraceptive instructions to patients — both for female contraceptives (OCP, emergency pills, implants) and male contraceptives (condom, vasectomy). Knowing the pharmacology makes the counselling credible and safe.
RECALL
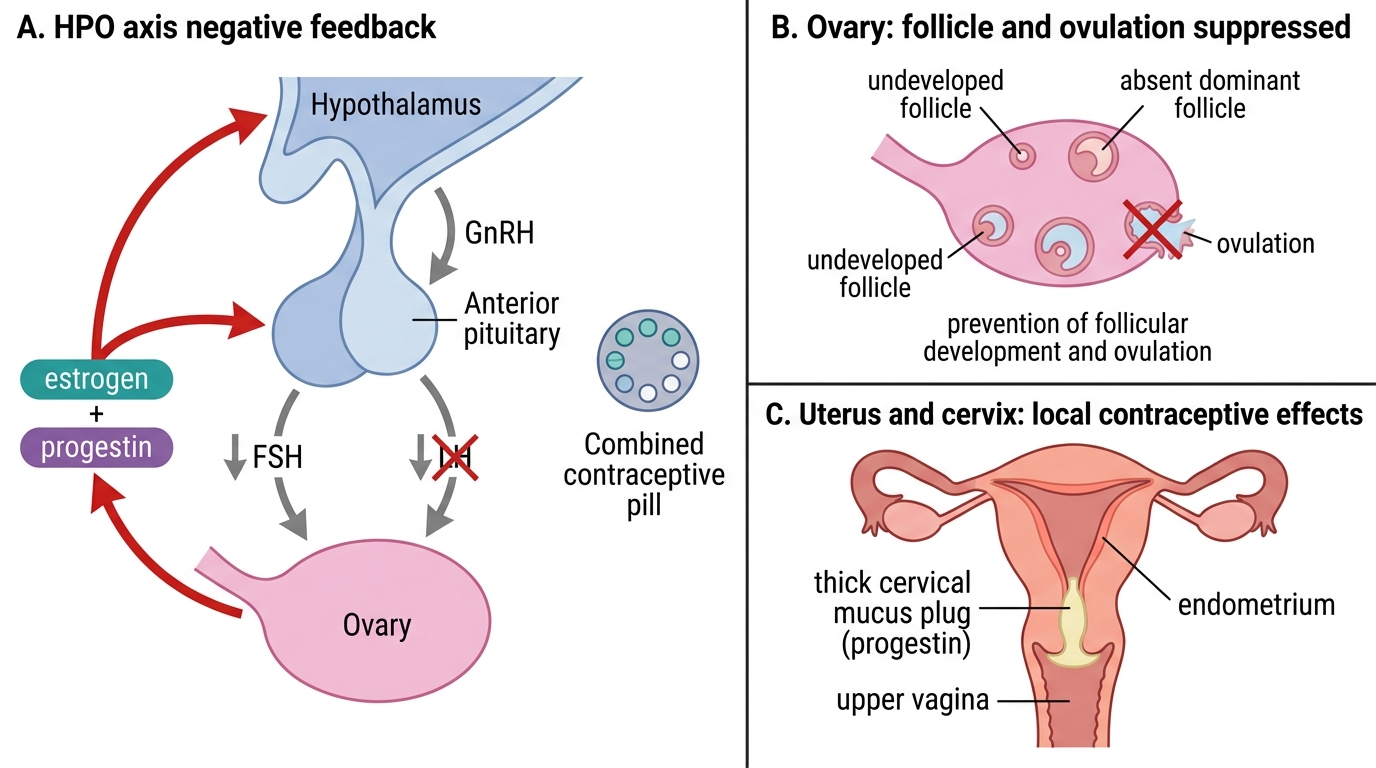
The hypothalamic-pituitary-ovarian (HPO) axis regulates the female menstrual cycle. GnRH (pulsatile from hypothalamus) → pituitary releases FSH (follicular stimulation) and LH (luteinising hormone). FSH drives follicular development and oestrogen production in the early follicular phase. Oestrogen initially provides negative feedback on FSH/LH (keeping levels appropriate). As the dominant follicle matures, rising oestrogen switches to positive feedback on LH → mid-cycle LH surge → ovulation (day 14). The ruptured follicle becomes the corpus luteum, which produces progesterone (and oestrogen) for the remaining 14 days of the cycle. Progesterone: thickens cervical mucus (blocks sperm passage), promotes decidualisation of the endometrium (prepares for implantation), and exerts negative feedback on LH/FSH. If no implantation: corpus luteum regresses → progesterone drops → menstruation. This cycle is the pharmacological target of all hormonal contraceptives.
Reproductive Hormone Physiology: The Target of Contraceptive Drugs
Hormonal contraceptives exploit the negative-feedback physiology of the HPO axis to prevent ovulation, sperm penetration, and/or implantation — depending on the method. Understanding which step of the reproductive process each drug targets is the key to explaining efficacy, failure modes, and patient counselling.
Three pharmacological targets of hormonal contraceptives:
- Prevention of ovulation (most important mechanism for COC and DMPA): exogenous oestrogen + progestogen suppress FSH and LH via negative feedback on the hypothalamus and pituitary → follicular development arrested, no dominant follicle → no LH surge → no ovulation. This is the primary contraceptive mechanism when hormonal levels are adequate (consistent pill-taking).
- Cervical mucus thickening (dominant mechanism for progestin-only methods): progesterone induces thick, viscous cervical mucus that is impenetrable to sperm — provides reliable contraception even in cycles where ovulation is not fully suppressed. The mini-pill (progestin-only oral) primarily relies on this mechanism.
- Endometrial modification (contributes to all hormonal methods): progestogens thin the endometrium and alter its secretory characteristics → even if ovulation occurs and fertilisation happens, implantation is impaired. This is a secondary mechanism — not the primary contraceptive effect for most methods.
Emergency contraception (EC) works mainly by delaying or preventing ovulation when taken early (before or around the time of the LH surge). Levonorgestrel EC is NOT abortifacient — it does not disrupt established implantation. Copper IUD EC works by copper ions impairing sperm function and potentially preventing implantation.
Mechanism of Combined Oral Contraceptive Action
Therapeutic Goals: Contraception, Emergency Prevention, and Patient Choice
The primary goal of contraception is preventing unintended pregnancy. However, modern contraceptive counselling encompasses far more than efficacy — it includes reversibility (temporary vs permanent), non-contraceptive benefits, patient values, and safety screening based on medical history.
Efficacy measurement — Pearl Index: number of pregnancies per 100 woman-years of use. Lower Pearl Index = more effective. Combined OCP: ~0.3 with perfect use, ~9 with typical use (missed pills reduce efficacy significantly). Copper IUD/hormonal implant: <0.1 (most effective reversible methods). DMPA injection: ~0.3 with perfect use. Condom alone: ~2–3 perfect use, ~15 typical use. Emergency contraceptive (levonorgestrel): ~75–89% reduction in pregnancy risk — NOT 75% efficacy overall.
Non-contraceptive benefits of combined OCP:
- Regulation of menstrual cycles, treatment of dysmenorrhoea
- Reduced risk of ovarian cancer (by 30–50% after ≥5 years) and endometrial cancer
- Treatment of endometriosis and polycystic ovary syndrome (PCOS) — reduces androgen excess, regulates cycle
- Reduced acne (anti-androgenic progestogens like cyproterone acetate/co-cyprindiol)
- Reduced iron-deficiency anaemia (lighter, regulated bleeding)
Patient medical history screening (before OCP): The WHO Medical Eligibility Criteria (MEC) system classifies contraceptive safety for specific conditions in 4 categories (1=always use, 2=benefits outweigh risks, 3=risks outweigh benefits, 4=unacceptable risk). Conditions where COC is WHO MEC Category 4 (absolute contraindication): personal history of VTE, current ischaemic heart disease, cerebrovascular accident/stroke, migraine with aura (focal neurological symptoms), breast cancer, uncontrolled hypertension, liver disease, smoking in women ≥35 years old.
SELF-CHECK
A 38-year-old woman has migraine with aura and wants to start the combined oral contraceptive pill. She asks if it is safe. The most appropriate response is:
A. A. COC is safe for migraines — it may even reduce headache frequency
B. B. COC is absolutely contraindicated in migraine with aura — the oestrogen component increases stroke risk in women with focal neurological symptoms
C. C. COC is safe if she does not have a family history of stroke
D. D. Switch to a lower-dose oestrogen OCP
Reveal Answer
Answer: B. B. COC is absolutely contraindicated in migraine with aura — the oestrogen component increases stroke risk in women with focal neurological symptoms
Migraine with aura (focal neurological symptoms preceding headache) is a WHO MEC Category 4 absolute contraindication to combined oral contraceptives. The oestrogen component increases the prothrombotic risk, and women with migraine with aura already have approximately 2× higher baseline stroke risk. The combination may cause ischaemic stroke. This is NOT dose-dependent — even low-dose oestrogen COC is contraindicated. Safe alternatives: progestin-only pill (mini-pill), DMPA, implant, copper IUD (non-hormonal) — progestin-only methods do not carry the same oestrogen-related thrombotic risk.
Classification of Contraceptive Methods and Drugs
Contraceptive methods span hormonal and non-hormonal modalities, each with different efficacy, convenience, reversibility, and ADR profiles.
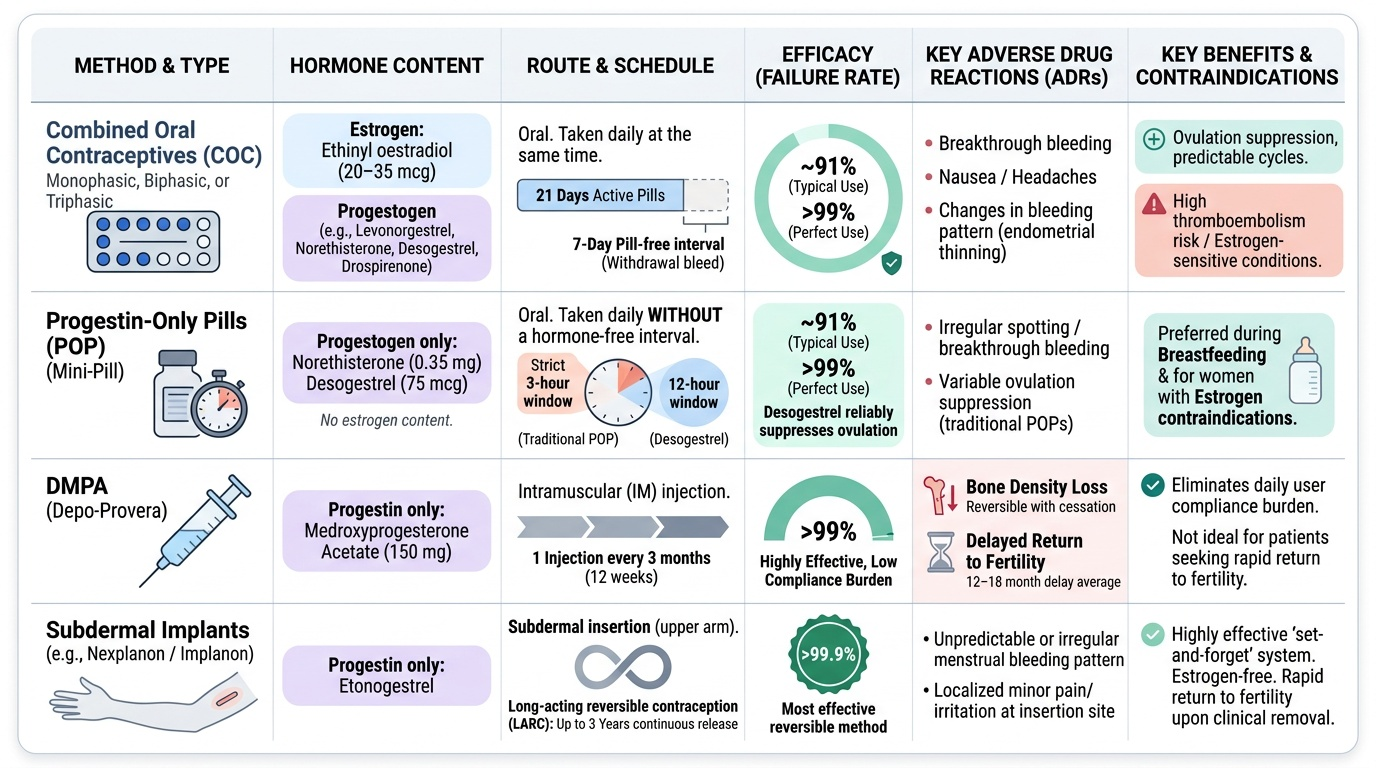
Combined Oral Contraceptives (COC): Monophasic (fixed-dose oestrogen + progestogen throughout), biphasic (variable progestogen), or triphasic (variable both). Modern low-dose pills contain ethinyl oestradiol 20–35 mcg (3rd generation contains less oestrogen) + a progestogen (levonorgestrel, norethisterone, desogestrel, drospirenone). Mechanisms: ovulation suppression (primary) + cervical mucus thickening + endometrial thinning. Taken daily × 21 days, then 7-day pill-free interval (withdrawal bleed) — or 24/4 or continuous.
Progestin-Only Pills (POP / mini-pill): Norethisterone 0.35 mg (Micronor), desogestrel 75 mcg — taken daily WITHOUT a hormone-free interval. Primary mechanism: cervical mucus thickening; may or may not suppress ovulation (desogestrel more reliably suppresses ovulation). Taken at the same time every day (narrow 3-hour window for traditional POP; 12 hours for desogestrel). Preferred in breastfeeding women (no oestrogen to suppress lactation) and women with oestrogen contraindications.
Depot Medroxyprogesterone Acetate (DMPA — Depo-Provera): 150 mg IM every 3 months. Highly effective (>99%); suppresses ovulation. Bone density may decrease with prolonged use (reversible). Return to fertility may be delayed up to 12–18 months. Useful when daily pill compliance is an issue.
Subdermal Implants: Etonogestrel implant (Implanon/Nexplanon) — small rod implanted subdermally in upper arm; releases etonogestrel 60–70 mcg/day for 3 years; most effective reversible contraception; primary mechanism: ovulation suppression + cervical mucus. ADR: irregular bleeding (common), insertion site complications.
Hormonal IUD (Mirena — Levonorgestrel IUD): 52 mg levonorgestrel; releases 20 mcg/day locally; 5-year efficacy >99%; primarily acts by local endometrial changes and cervical mucus. Reduces menstrual bleeding (useful in menorrhagia). Systemic hormone levels very low.
Copper IUD: Copper ions are toxic to sperm (impair motility and penetration). Non-hormonal; T-shaped device; efficacy >99% long-term (5–10 years); can be used as emergency contraception up to 120 hours (5 days) post-coitus — most effective EC. ADR: heavier, more painful periods.
Emergency Contraception (EC):
- Levonorgestrel 1.5 mg (Plan B, I-pill): single dose; most effective if taken within 72 hours (effective up to 120 hours with reduced efficacy); primarily delays/prevents ovulation; NOT abortifacient.
- Ulipristal acetate 30 mg (ellaOne): selective progesterone receptor modulator (SPRM); effective up to 120 hours; slightly more effective than levonorgestrel at 72–120 hours; inhibits or delays ovulation (even near LH surge).
- Copper IUD: most effective EC — up to 5 days post-coitus, failure rate <1%.
- Mifepristone (RU-486): antiprogestogen — used for medical termination of pregnancy (with misoprostol), NOT as regular emergency contraceptive in India in its standard formulation.
Barrier Methods: Male condom (external condom) — only method that also prevents STIs — critical counselling point. Female condom (internal condom). Diaphragm + spermicide. No systemic ADRs.
Permanent Methods: Tubal ligation (female sterilisation — bilateral salpingotomy/occlusion); vasectomy (male — simpler, safer procedure, equally effective).
Provided image