Page 22 of 36
PH7.7 | PH7.7 | Contraceptive Pharmacology — SDL Guide — SDL Guide (Part 2)
Mechanisms, PK, Uses, and ADRs of Hormonal Contraceptives
The pharmacology of hormonal contraceptives centres on the oestrogen-progestogen combination and the specific progestogen used, which determines both efficacy and the adverse effect profile.
Combined OCP Pharmacokinetics: Ethinyl oestradiol (EE) is well-absorbed orally; high first-pass metabolism; half-life ~6–20 hours; hepatic metabolism via CYP3A4. Drug interaction critical warning: Enzyme inducers (rifampicin, phenytoin, carbamazepine, St John's Wort) accelerate EE/progestogen metabolism → contraceptive failure → use condoms or alternative method during and for 28 days after enzyme inducer course. Progestogens vary: 1st-gen (norethisterone, norgestrel) → moderate androgenic activity; 2nd-gen (levonorgestrel) → moderate androgenic, less VTE risk; 3rd-gen (desogestrel, gestodene) → anti-androgenic, possibly slightly higher VTE risk than 2nd-gen; 4th-gen (drospirenone) — anti-mineralocorticoid (reduces water retention, BP), anti-androgenic (useful in PCOS/acne).
VTE (Venous Thromboembolism) Risk with COC: Oestrogen stimulates hepatic production of coagulation factors (II, VII, X) and reduces antithrombin III → increased thrombus risk. COC users have 3–4× relative increased VTE risk vs non-users, but absolute risk is still low (~3–9 per 10,000 woman-years depending on progestogen type). VTE risk is higher with higher oestrogen dose and in women with inherited thrombophilias, obesity, immobility, or family history. Progestin-only methods do NOT significantly increase VTE risk — preferred in women with thrombotic risk factors.
ADRs of COC: Nausea, breast tenderness, breakthrough bleeding, mood changes, headache, reduced libido, weight gain (minimal with modern low-dose pills). Serious: VTE, ischaemic stroke (especially in smokers ≥35 and migraine with aura), hypertension, hepatic adenoma (rare), reduced milk production in breastfeeding (oestrogen suppresses prolactin).
Progestin-only oral — specific ADRs: Irregular bleeding (spotting, amenorrhoea), narrow dosing window (traditional POP: 3-hour window — if late, use backup method for 48 hours).
DMPA-specific ADRs: Irregular bleeding initially → amenorrhoea in many after 12 months; delayed return to fertility (12–18 months); decreased bone density with long-term use (reversible); weight gain; mood changes.
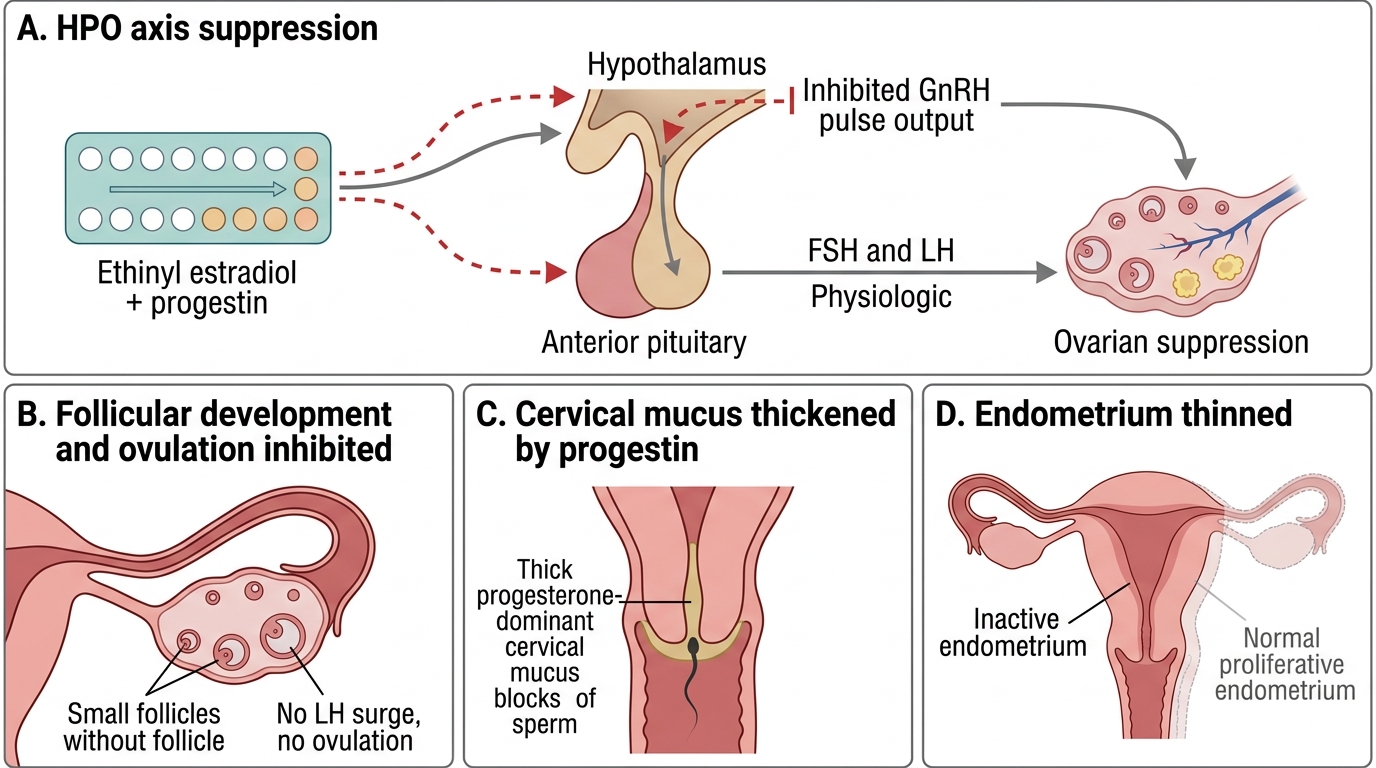
Mechanism of Combined Oral Contraceptive Action
CLINICAL PEARL
Three critical patient instructions for different contraceptive methods: (1) COC 'missed pill' rule: If ONE pill is missed (<24 hours late): take it as soon as remembered, continue the pack — no backup needed. If TWO or more consecutive pills missed: take the most recent missed pill immediately, use condom backup for 7 days; if in week 3 of the pack, skip the pill-free interval and start the next pack immediately (prevents ovarian escape during the pill-free period). (2) Emergency contraceptive timing: Levonorgestrel is most effective within 72 hours — tell patients 'the sooner the better.' Ulipristal acetate extends the window to 120 hours with maintained efficacy. Copper IUD up to 120 hours — most effective option. (3) Condom is the ONLY STI prevention method — hormonal and IUD methods do not protect against HIV, gonorrhoea, or chlamydia. Dual method use (condom + hormonal) is recommended in new relationships.
SELF-CHECK
A woman has unprotected intercourse. It is now 84 hours later (3.5 days). Which emergency contraceptive is most appropriate?
A. A. Levonorgestrel 1.5 mg — still effective at this time
B. B. Ulipristal acetate 30 mg — effective up to 120 hours, more reliable at 72–120 hours than levonorgestrel
C. C. Copper IUD — effective up to 120 hours but requires an invasive procedure
D. D. Either B or C — both are appropriate at 84 hours; choice depends on patient preference and STI risk
Reveal Answer
Answer: D. D. Either B or C — both are appropriate at 84 hours; choice depends on patient preference and STI risk
At 84 hours (3.5 days), both ulipristal acetate and copper IUD are appropriate. Levonorgestrel is less effective beyond 72 hours compared to ulipristal acetate — option A is not optimal. Ulipristal acetate (30 mg, single dose, up to 120 hours) is more effective than levonorgestrel at 72–120 hours and remains the preferred oral EC in this window. Copper IUD remains the most effective EC option at any time point up to 120 hours (failure rate <1%) AND provides ongoing contraception — preferred if the patient wants long-term coverage and is at STI risk (condom for STI separately). Both B and C are correct — patient preference, access, and clinical context guide the choice.
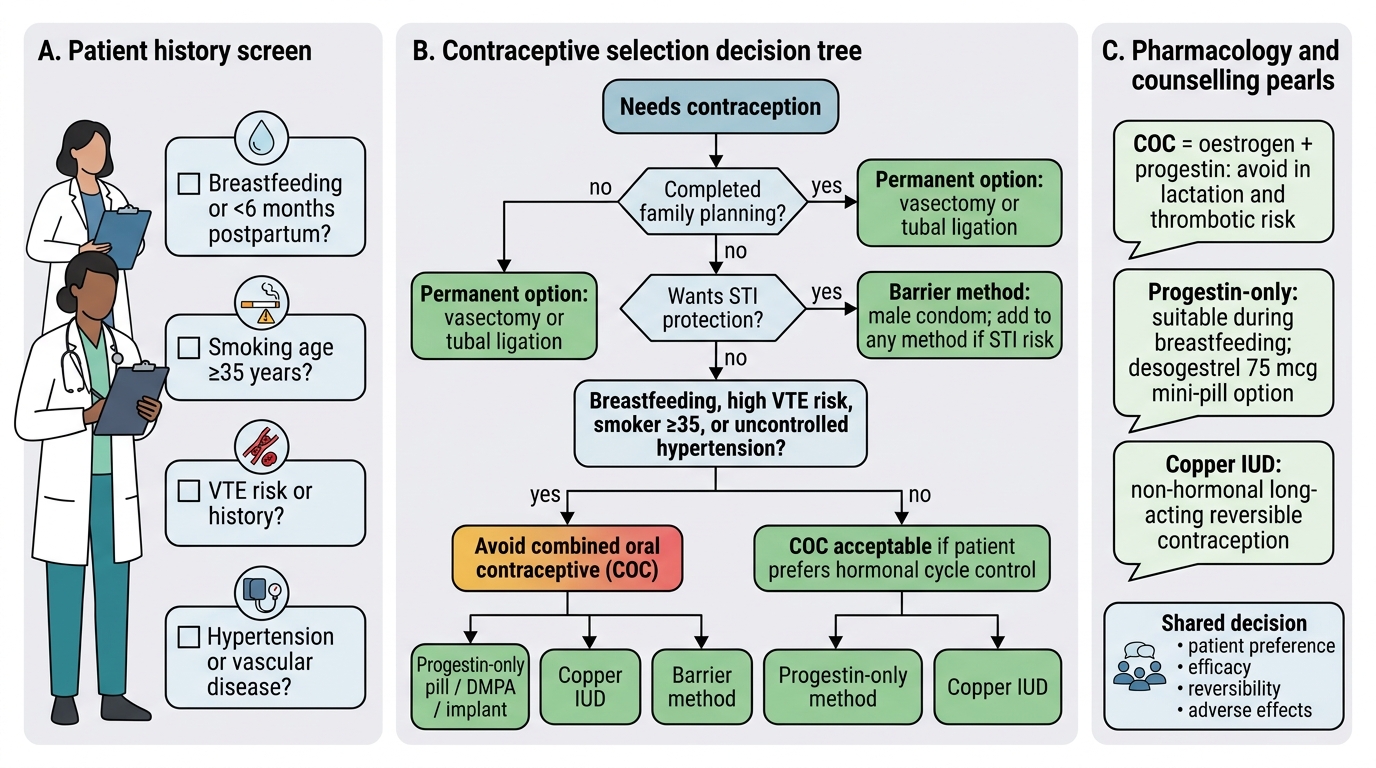
Clinical Decision-Making: Instructions for Use and Contraindications
Contraceptive selection is a shared decision informed by the patient's medical history, lifestyle, fertility intentions, and values. The following clinical frameworks guide rational selection.
Female contraceptive counselling framework:
For a healthy young woman with no contraindications: COC first-line (highly effective, regular periods, non-contraceptive benefits). Counsel on daily adherence, missed pill rules, and enzyme-inducer interactions. If compliance is a concern: DMPA (3-monthly), implant (3-yearly), or hormonal IUD.
For a breastfeeding woman: oestrogen suppresses prolactin → COC reduces milk supply. Use progestin-only methods — mini-pill, DMPA, or implant. Copper IUD also safe and non-hormonal.
For a woman who smokes and is ≥35 years old: COC is WHO MEC Category 4 (unacceptable risk) — smoking + age + oestrogen creates excessive cardiovascular/VTE risk. Use progestin-only or non-hormonal methods.
For a woman with VTE history/thrombophilia/migraine with aura/uncontrolled hypertension/breast cancer: COC contraindicated. Use progestin-only (safe for most) or copper IUD.
For women with heavy periods or endometriosis: levonorgestrel IUD (Mirena) reduces menstrual bleeding and provides contraception — dual benefit.
For PCOS/acne: COC with anti-androgenic progestogen (drospirenone or co-cyprindiol/Diane-35 in some countries).
Male contraceptive counselling:
- Male condom (external condom): Latex or polyurethane. Place on erect penis before any genital contact (pre-ejaculatory fluid contains sperm). Use water-based lubricant with latex (oil-based breaks latex). Leave space at tip. Dispose after each use. Only method preventing STIs. Failure: user error (incorrect placement, breakage, not used consistently) — typical-use Pearl Index ~15%.
- Vasectomy: Permanent, highly effective (>99%). Outpatient procedure under local anaesthetic; vas deferens cut/ligated bilaterally. Not immediately effective — sperm present in reproductive tract for 12–20 ejaculations post-procedure; use backup until azoospermia confirmed by semen analysis at 3 months. Reversal technically possible but unreliable — counsel as permanent.
Instructions for COC use:
1. Start on day 1 of period (no backup needed) OR any day (use condom for 7 days).
2. Take one pill daily at the same time. 21 pills → 7-day break (period occurs) → restart.
3. If vomiting within 2 hours of pill: take another pill.
4. If taking rifampicin or enzyme-inducers: use condoms PLUS another method.
5. If surgery planned (immobility risk): stop COC 4 weeks before elective surgery (VTE prevention).
Decision Tree for Contraceptive Selection
Self-Assessment: Contraceptive Counselling Scenarios
Apply your contraceptive pharmacology knowledge to counsel these patients:
Scenario A: A 26-year-old breastfeeding mother (4 months postpartum) wants a reversible contraceptive. She is otherwise healthy. What do you recommend and why?
Answer: Progestin-only pill (mini-pill) — desogestrel 75 mcg preferred (more reliable ovulation suppression, wider dosing window). Reason: oestrogen in COC suppresses prolactin and reduces breast milk production — contraindicated in breastfeeding women. Progestin-only methods do not affect milk supply. DMPA or etonogestrel implant are also good progestin-only options. Copper IUD is another option if she wants non-hormonal long-term contraception.
Scenario B: A newly married couple asks about contraception. The husband asks: 'Do I need to do anything, or is it only for my wife?' What do you say about male contraception options?
Answer: Male condoms are the primary male contraceptive method — highly important because they are the only method preventing STIs. Consistent and correct use (on before any contact, correct size, water-based lubricant, check expiry) is essential for efficacy. Vasectomy is an option if the couple has completed family planning. Hormonal male contraceptives (testosterone-based) are under investigation but not approved for clinical use. Dual method use (condom + female hormonal) provides the highest protection against both pregnancy and STIs.
SELF-CHECK
A woman on combined oral contraceptive pills is prescribed rifampicin for tuberculosis treatment. The correct advice is:
A. A. Continue the OCP unchanged — rifampicin has no effect on OCP efficacy
B. B. Stop the OCP and use a copper IUD instead permanently
C. C. Continue the OCP but add condom use as a backup method during rifampicin treatment and for 28 days after completing the course
D. D. Double the OCP dose while on rifampicin
Reveal Answer
Answer: C. C. Continue the OCP but add condom use as a backup method during rifampicin treatment and for 28 days after completing the course
Rifampicin is a potent CYP3A4 inducer — it markedly accelerates hepatic metabolism of ethinyl oestradiol and the progestogen in OCP, potentially reducing plasma levels to sub-contraceptive concentrations. This is a well-documented drug interaction causing OCP failure (pregnancies reported). The recommendation: continue OCP AND use condom as additional backup during rifampicin treatment AND for 28 days after the last rifampicin dose. Doubling the OCP dose is not standard practice and not recommended. Stopping OCP is not required — adding a barrier method provides adequate safety.