Page 24 of 36
PH7.8 | PH7.8 | Uterine Relaxants and Stimulants — SDL Guide — SDL Guide
Learning Objectives
- Classify uterotonic drugs (oxytocin, ergot alkaloids, prostaglandins) and tocolytic drugs with their mechanisms
- Describe the pharmacokinetics, indications, and adverse effects of each drug class
- Identify the contraindications to ergometrine and carboprost in obstetric use
- Apply a pharmacological decision-making framework to postpartum haemorrhage management
- Select appropriate tocolytic therapy for preterm labour based on gestational age and maternal comorbidities
INSTRUCTIONS
Uterine pharmacology is applied obstetric pharmacology — drugs that initiate labour when it is delayed, control haemorrhage when it is catastrophic, and halt contractions when labour is premature. Postpartum haemorrhage (PPH) is the leading cause of maternal death globally, and its pharmacological management — the right uterotonic in the right sequence — can be life-saving. Preterm labour pharmacology aims to buy time for fetal lung maturation with corticosteroids. This guide covers the therapeutic rationale, mechanisms, and critical contraindications of uterine drugs.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 23 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 66 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman delivers a healthy baby after normal vaginal delivery. Five minutes post-delivery, she develops heavy vaginal bleeding — 700 mL and counting. BP is falling. The uterus is flabby and poorly contracted (uterine atony). The midwife calls for the emergency uterotonic kit. You are the duty doctor: What is your first drug? What route? If that fails, can you give ergometrine — and is her blood pressure a contraindication? If still bleeding, what third-line agent can you use, and what comorbidity in her history would make you reconsider it? This is postpartum haemorrhage management — pharmacologically choreographed to save a mother's life.
WHY THIS MATTERS
Postpartum haemorrhage (PPH — defined as blood loss >500 mL within 24 hours of delivery; >1000 mL after caesarean) is the leading cause of maternal death globally. Over 80% of PPH cases are due to uterine atony (failure of the uterus to contract after delivery). Uterotonics are the pharmacological solution — and knowing the sequence (oxytocin → ergometrine → misoprostol → carboprost → surgical) and the contraindications of each saves lives. Simultaneously, the ability to halt premature contractions (tocolysis) to allow steroid administration for fetal lung maturation can prevent neonatal death from respiratory distress syndrome.
RECALL
The myometrium (uterine smooth muscle) contracts via the same calcium-myosin mechanism as other smooth muscle. Rising intracellular Ca²⁺ activates calmodulin → activates myosin light chain kinase (MLCK) → phosphorylates myosin → actin-myosin cross-bridging → contraction. Drugs that increase intracellular Ca²⁺ or increase MLCK activity promote contraction (uterotonics). Drugs that reduce Ca²⁺ influx or activate cAMP/cGMP pathways reduce MLCK activity, promoting relaxation (tocolytics). Oxytocin receptor (OTR) is a GPCR (Gq-coupled) — oxytocin binding → IP3/DAG pathway → Ca²⁺ release from SR → contraction. OTRs are dramatically upregulated at term (up to 300×), making the uterus highly oxytocin-sensitive just before labour. Prostaglandins (PGE2, PGF2α) also stimulate uterine contractions and promote cervical ripening (softening and effacement) — key roles in the cascade of parturition. Beta-2 adrenergic stimulation → cAMP → PKA → MLCK inhibition → relaxation → tocolysis.
Uterine Smooth Muscle Physiology: Receptors and Regulation
The transition of the uterus from a quiescent organ during pregnancy to an actively contracting organ during labour is regulated by shifts in receptor expression and hormonal milieu. Understanding these shifts explains the pharmacological targets of both uterotonics and tocolytics.
Throughout pregnancy, the uterus is maintained in a quiescent state by: (1) progesterone dominance — progesterone reduces oxytocin receptor expression and inhibits gap junction formation between myometrial cells (prevents synchronised contractions); (2) NO production — from placenta and decidua; (3) prostacyclin (PGI2) — produced by decidua, relaxes myometrium. At term, falling progesterone, rising oestrogen, and increased corticotrophin-releasing hormone (CRH) from the placenta shift the balance: oxytocin receptor (OTR) density increases up to 300-fold on the myometrial cell surface; gap junctions form between myocytes (synchronising contractions); prostaglandin production by the amnion and decidua increases; and cortisol stimulates the fetal-placental CRH surge. The result: the uterus becomes exquisitely sensitive to low circulating levels of oxytocin — even a small oxytocin pulse triggers a coordinated contraction.
This physiological process has direct pharmacological implications: oxytocin for induction of labour is only effective at term (when OTRs are expressed) — attempting induction at 32 weeks may require much higher doses; prostaglandins (especially PGE2 for cervical ripening) exploit the natural parturition cascade; tocolytics work by opposing the contractile mechanisms (blocking oxytocin receptor, blocking Ca²⁺ influx via CCB, stimulating cAMP via β2 agonists, or inhibiting prostaglandin synthesis via NSAIDs).
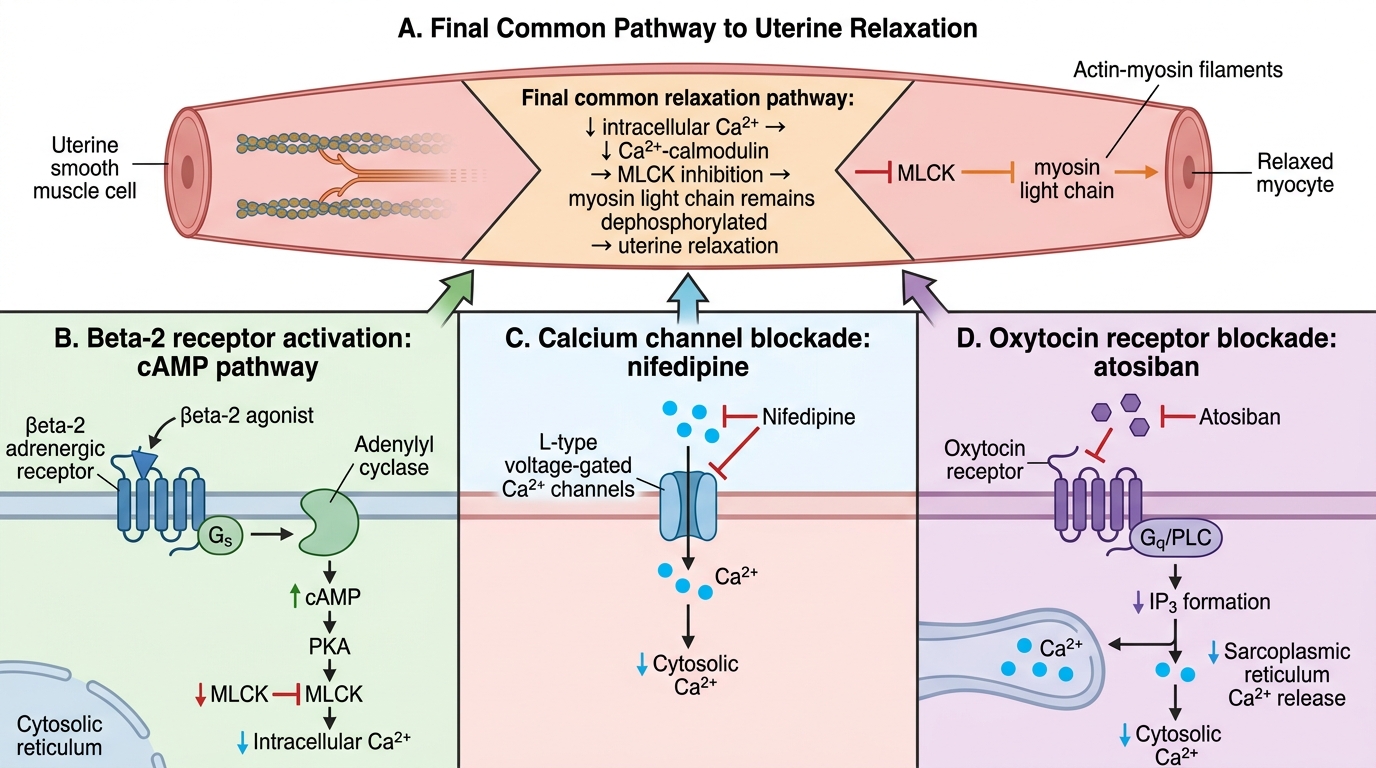
Tocolytic Pathways Converging on Uterine Relaxation
Therapeutic Goals: When to Stimulate vs Relax the Uterus
The therapeutic decision to stimulate or relax the uterus is driven by two primary clinical scenarios — each representing a life-threatening situation if pharmacologically mismanaged.
Indications for uterine stimulation (uterotonics):
- Induction of labour: medically indicated when continuation of pregnancy carries greater maternal or fetal risk than delivery (post-term pregnancy, pre-eclampsia, IUGR, ruptured membranes without contractions). Oxytocin IV (first-line for induction) or prostaglandins (PGE2/misoprostol for cervical ripening before oxytocin).
- Augmentation of labour: stimulation of inadequate spontaneous contractions in established labour. Oxytocin IV infusion titrated.
- Postpartum haemorrhage (PPH) prevention: routine administration of oxytocin at delivery of the anterior shoulder (active management of third stage of labour — AMTSL) reduces PPH incidence by 50–60%.
- PPH treatment: escalating uterotonic therapy for atonic PPH — oxytocin → ergometrine → misoprostol → carboprost (escalating options).
- Cervical ripening: unfavourable cervix before induction — PGE2 gel/pessary (dinoprostone) or misoprostol.
Indications for uterine relaxation (tocolytics):
- Preterm labour suppression (tocolysis): delay delivery by 24–48 hours to allow maternal corticosteroid (betamethasone/dexamethasone) administration for fetal lung maturation — the primary goal of tocolysis is NOT to prevent preterm birth indefinitely, but to gain time for this life-saving treatment.
- External cephalic version (ECV): uterine relaxation facilitates manual turning of a breech fetus.
- Tetanic uterine contractions: iatrogenic or spontaneous — tocolysis to prevent fetal asphyxia.
- Uterine surgery: relaxation to facilitate intrauterine procedures.
SELF-CHECK
Oxytocin IV infusion is used for induction of labour. What is the pharmacological explanation for why oxytocin given at 32 weeks gestation requires a much higher dose than at 40 weeks to produce equivalent uterine contractions?
A. A. Oxytocin is metabolised faster at 32 weeks by the immature kidney
B. B. Oxytocin receptor (OTR) expression on myometrial cells is dramatically lower at 32 weeks than at term — fewer receptors means a greater oxytocin concentration is needed for the same contractile effect
C. C. The myometrium is less responsive to Ca²⁺ at 32 weeks due to immature smooth muscle
D. D. Placental oxytocin metabolism increases with gestation
Reveal Answer
Answer: B. B. Oxytocin receptor (OTR) expression on myometrial cells is dramatically lower at 32 weeks than at term — fewer receptors means a greater oxytocin concentration is needed for the same contractile effect
Oxytocin receptor expression on myometrial cells increases up to 300-fold during the last weeks of pregnancy (rising oestrogen + CRH drive OTR upregulation). At 32 weeks, OTR density is substantially lower — the same oxytocin dose produces far fewer receptor-activated contractions. This is a classic example of receptor-dependent pharmacodynamics: drug potency in vivo depends on both drug concentration AND receptor expression level. The clinical implication: early induction attempts are often futile without cervical ripening agents; oxytocin dose requirements are much higher preterm.
Uterine Stimulants: Oxytocin, Ergot Alkaloids, and Prostaglandins
Uterotonic drugs stimulate myometrial contractions by activating oxytocin receptors, prostaglandin receptors, or ergot alkaloid receptors — each with distinct patterns of contractility, speed of onset, and clinical applications.
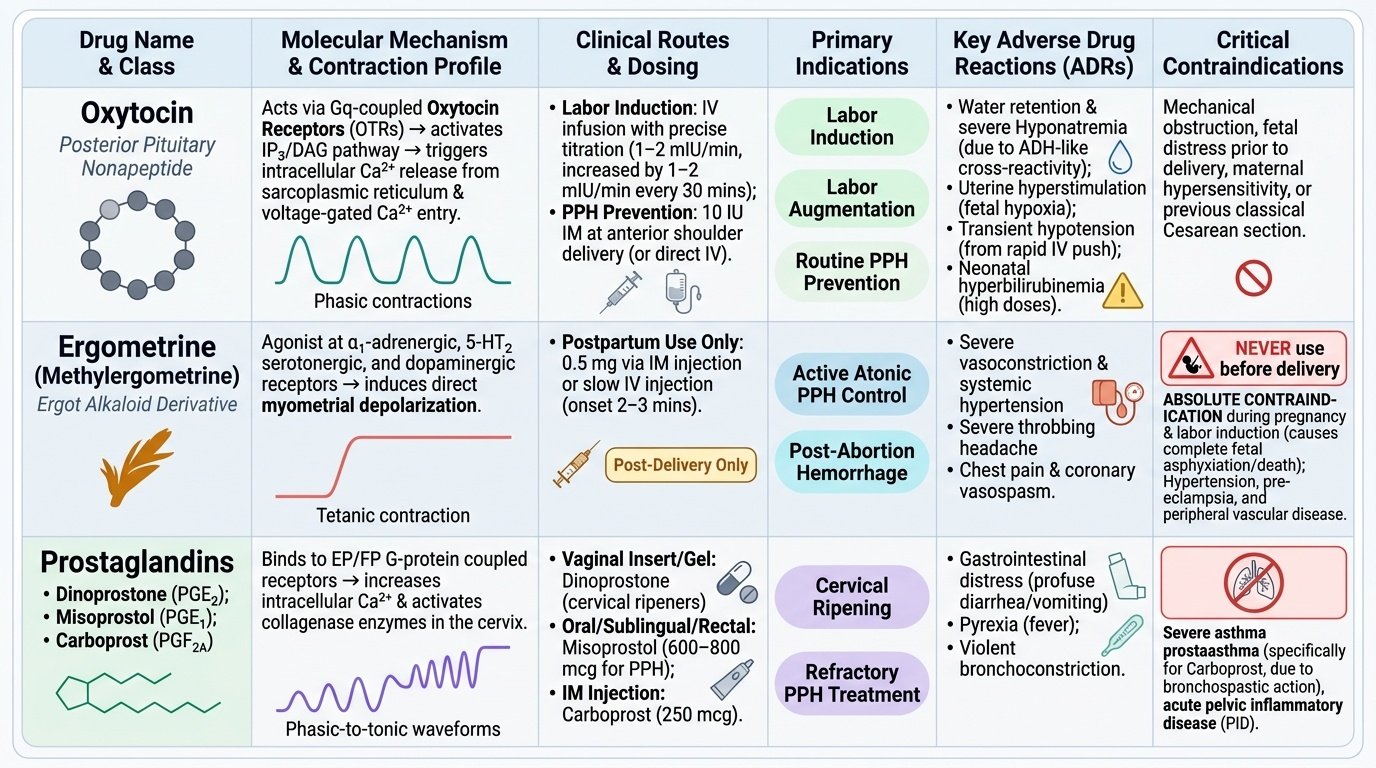
Oxytocin: Posterior pituitary nonapeptide (also produced by the hypothalamus). Activates Gq-coupled OTRs → IP3/DAG → SR Ca²⁺ release + voltage-gated Ca²⁺ channel activation → contractions. For labour induction and augmentation: IV infusion with careful titration (low-dose: 1–2 mIU/min, increase by 1–2 mIU/min every 30 minutes until adequate contractions). For PPH (routine prevention): 10 IU IM at delivery of the anterior shoulder — or IV if no IM access. ADRs: water retention/hyponatraemia (oxytocin has mild ADH-like action — risk with large volumes of 5% dextrose carrier; use normal saline); uterine hyperstimulation (too rapid infusion → fetal hypoxia); neonatal hyperbilirubinaemia (high doses); hypotension (rapid IV bolus). Short half-life (~5 min) — easily titratable.
Ergot Alkaloids — Ergometrine (Ergonovine) and Methylergometrine: Ergot alkaloids act on α-adrenergic, dopaminergic, and serotonin receptors; cause tetanic (sustained) uterine contraction — different from oxytocin's phasic (intermittent) contractions. For PPH: IM or slow IV ergometrine 0.5 mg — onset ~2–3 minutes (IM), effectively controls atonic PPH. CONTRAINDICATED IN LABOUR INDUCTION: sustained tetanic contraction → uteroplacental blood flow ceases → fetal asphyxia and fetal death. Only used POST-DELIVERY. Contraindications: hypertension, pre-eclampsia, cardiac/coronary disease (causes peripheral and coronary vasoconstriction — can precipitate angina/MI), Raynaud's phenomenon. ADRs: nausea/vomiting, hypertension, vasoconstriction.
Prostaglandins:
- Dinoprostone (PGE2): Intravaginal gel or slow-release pessary for cervical ripening (softens unfavourable cervix before oxytocin induction). Acts on EP receptors → cervical collagenase activation + myometrial stimulation. Onset: 30–60 minutes. Remove pessary (retrievable) if hyperstimulation occurs.
- Misoprostol (PGE1 synthetic analogue): Oral, sublingual, vaginal, or rectal. Versatile — used for cervical ripening, labour induction, PPH prevention and treatment. Thermostable (no cold chain needed) — important in low-resource settings. Contraindicated for induction if prior uterine scar (caesarean) — markedly increased uterine rupture risk. ADRs: diarrhoea, shivering, fever, uterine hyperstimulation.
- Carboprost (15-methyl-PGF2α): IM injection for refractory PPH — used when oxytocin and ergometrine have failed. Potent uterotonic. CONTRAINDICATED IN ASTHMA — PGF2α class causes bronchoconstriction; life-threatening bronchospasm in asthmatic patients. Also contraindicated in severe cardiovascular disease. ADRs: flushing, diarrhoea, vomiting, bronchoconstriction.
Provided image