Page 25 of 36
PH7.8 | PH7.8 | Uterine Relaxants and Stimulants — SDL Guide — SDL Guide (Part 2)
Uterine Relaxants: Beta-2 Agonists, Nifedipine, Atosiban, Magnesium
Tocolytic agents suppress uterine contractions in preterm labour to gain time for fetal maturation. The goal of tocolysis is primarily to delay delivery by 24–48 hours (time for corticosteroid administration) — not to prevent preterm birth indefinitely. No tocolytic has been shown to significantly reduce perinatal mortality when used for prolonged periods.
Beta-2 Adrenergic Agonists — Ritodrine and Terbutaline: Ritodrine (IV) and terbutaline (SC/oral) stimulate β2 adrenergic receptors on myometrial cells → cAMP → PKA → phosphorylation and inactivation of MLCK → reduced Ca²⁺ sensitivity of myosin → relaxation. Effective tocolytics but significant cardiovascular ADRs (result of β1 receptor activation even with β2 selectivity): maternal tachycardia, palpitations, tremor, hypokalemia, hyperglycaemia, pulmonary oedema (at high doses). Terbutaline is preferred (less expensive, SC route) but must be used cautiously. Contraindicated in maternal cardiac disease, uncontrolled diabetes (hyperglycaemia), and pre-eclampsia (cardiac stress). IV fluids restricted to avoid pulmonary oedema.
Nifedipine (Calcium Channel Blocker): Preferred first-line oral tocolytic in many countries including India (cost-effective, oral, well-tolerated). Blocks L-type Ca²⁺ channels in myometrial smooth muscle → reduced Ca²⁺ influx → less MLCK activation → reduced contraction. ADRs: flushing, headache, maternal hypotension, peripheral oedema. Drug interaction: nifedipine + magnesium sulphate — enhanced hypotension and neuromuscular blockade (use together cautiously).
Atosiban (Oxytocin Receptor Antagonist): Competitive antagonist of oxytocin (and vasopressin V1a) receptors. Parenteral (IV bolus then infusion). Effective tocolysis with fewer maternal ADRs than β2 agonists (no tachycardia, no metabolic effects) — preferred in patients with cardiac disease. Disadvantage: high cost limits use in Indian public health settings; not easily available.
Indomethacin (NSAID — COX Inhibitor): Inhibits cyclooxygenase (COX) → reduces prostaglandin synthesis (PGE2, PGF2α) → reduces prostaglandin-driven uterine contractions. Effective tocolytic especially before 32 weeks gestation. Fetal risks with prolonged use: premature closure of the ductus arteriosus (PGE2 keeps it patent — NSAID blocks this → DA constriction → pulmonary hypertension in neonate); reduced fetal urine output → oligohydramnios. Restricted to short-term use (<48–72 hours) and before 32 weeks; contraindicated in renal dysfunction, platelet disorders.
Magnesium Sulphate (MgSO₄): Mechanism as tocolytic: Mg²⁺ competes with Ca²⁺ at voltage-gated channels and at the Ca²⁺-calmodulin interface → reduces Ca²⁺-dependent MLCK activation → myometrial relaxation. Also acts as a NMDA receptor antagonist — basis for neuroprotection (reduces cerebral palsy risk in preterm infants <32 weeks). Used in preterm labour (<32 weeks) primarily for neuroprotection; tocolysis is a secondary benefit. Also used for eclampsia/severe pre-eclampsia (antiseizure mechanism — NMDA receptor block, cerebral vasodilation). Toxicity spectrum: loss of deep tendon reflexes (DTR) → respiratory depression → cardiac arrest (at very high serum Mg²⁺). Antidote: calcium gluconate 10% IV (10 mL slow IV) — competes with Mg²⁺ at Ca²⁺ channels; must be immediately available at bedside during MgSO₄ infusion.
CLINICAL PEARL
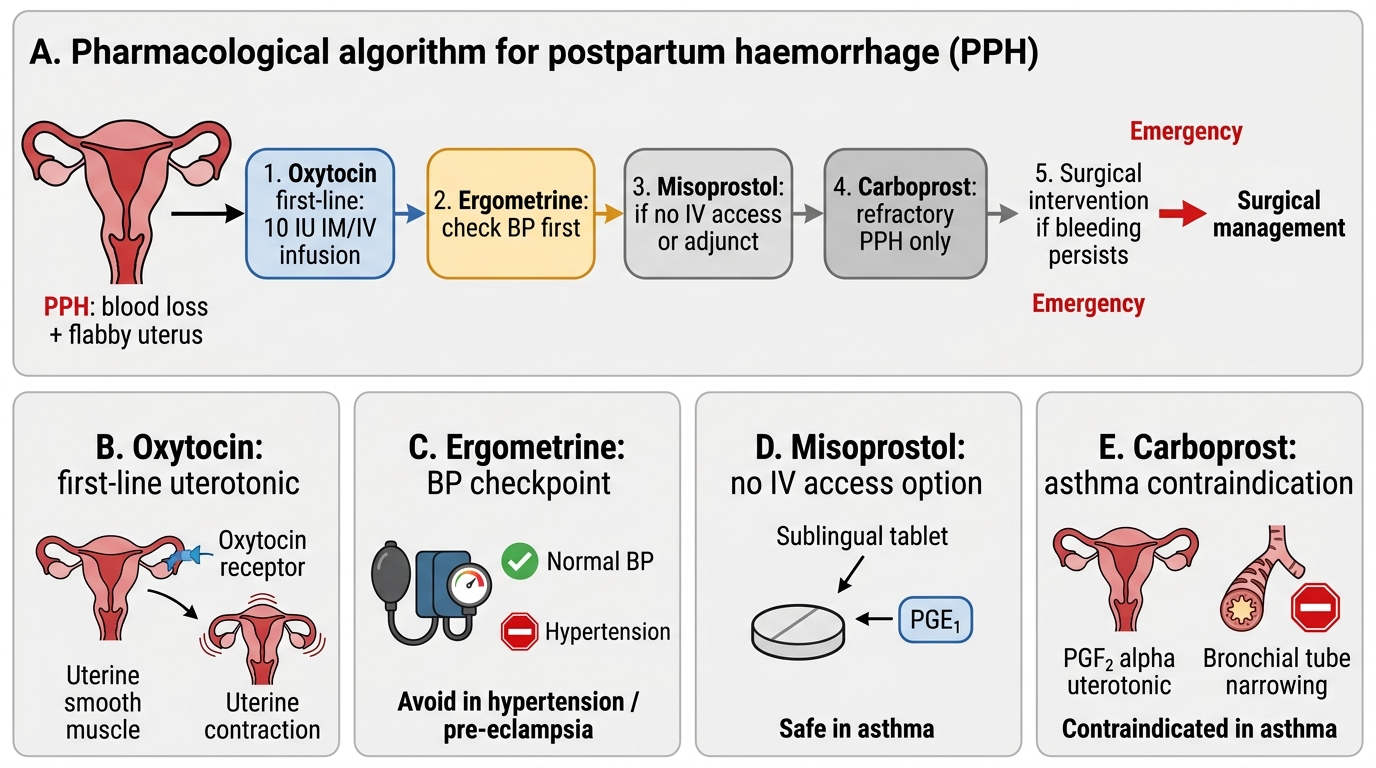
The PPH uterotonic escalation sequence has pharmacological logic in each step: (1) Oxytocin first — rapid onset, titratable, safe; (2) Ergometrine if oxytocin fails — tetanic contraction provides stronger hemostasis, but CHECK blood pressure first (vasoconstriction in hypertension = life-threatening); (3) Misoprostol (SL or rectal) — can be given when IV access is lost and no cold chain (thermostable), effective in low-resource settings; (4) Carboprost (PGF2α) — LAST pharmacological resort before surgical; check for asthma history BEFORE every dose — life-threatening bronchospasm in asthmatic patients is a documented cause of maternal death from carboprost. The carboprost-asthma contraindication is non-negotiable.
SELF-CHECK
A woman with a history of asthma develops refractory PPH that has not responded to oxytocin or ergometrine. Which of the following drugs should be avoided?
A. A. Misoprostol (sublingual)
B. B. Carboprost (15-methyl-PGF2α)
C. C. Tranexamic acid (antifibrinolytic)
D. D. IV oxytocin infusion (higher rate)
Reveal Answer
Answer: B. B. Carboprost (15-methyl-PGF2α)
Carboprost (15-methyl-PGF2α) is CONTRAINDICATED in asthma. PGF2α class prostaglandins cause bronchoconstriction — in asthmatic patients, carboprost can trigger severe, life-threatening bronchospasm. This is an absolute contraindication. Misoprostol (PGE1 analogue) does not cause bronchoconstriction and is generally safe in asthma (PGE1 class may even bronchodilate). Tranexamic acid (antifibrinolytic, reduces fibrinolysis in PPH haemorrhage) is safe in asthma. IV oxytocin (higher rate) is safe in asthma. The correct next step in this asthmatic patient with refractory PPH after oxytocin + ergometrine: misoprostol, tranexamic acid, uterine balloon tamponade, or surgical intervention.
Clinical Decision-Making: Choosing Uterotonics and Tocolytics
Rational drug selection in obstetric uterine pharmacology requires integrating the clinical scenario (PPH vs preterm labour), the patient's comorbidities (asthma, hypertension, cardiac disease), and the drug's specific contraindications.
PPH pharmacological management (stepwise):
Step 1: Oxytocin 10 IU IV bolus (slow) or IM — first-line for all PPH (universal, no contraindications in PPH except hypernatraemia from hypotonic fluids); continue IV infusion (20–40 IU in 500 mL normal saline at 250 mL/hour) for ongoing tone.
Step 2: Ergometrine 0.5 mg IM (or slow IV) — CHECK blood pressure first; if hypertensive or pre-eclamptic: SKIP or use with extreme caution.
Step 3: Misoprostol 800–1000 mcg (sublingual or rectal) — can be administered without IV access; safe in asthma, hypertension; no cold chain.
Step 4: Carboprost 250 mcg IM every 15–90 minutes (max 8 doses) — highly effective for atonic PPH; CONTRAINDICATED in asthma. Check history before each administration.
Step 5: Surgical/interventional — uterine balloon tamponade, B-Lynch suture, uterine artery ligation, hysterectomy.
Note: Tranexamic acid (antifibrinolytic) 1 g IV should be administered early in PPH (within 3 hours of delivery) regardless of the uterotonic sequence — reduces mortality from haemorrhage (WOMAN trial).
Tocolytic selection for preterm labour:
| Drug | Preferred in | Avoid in | Route |
|---|---|---|---|
| Nifedipine | Most patients, first-line | Severe hypotension | Oral |
| Atosiban | Cardiac disease, β2 ADR intolerance | Cost-limited settings | IV |
| Terbutaline | Short-term (SC), bridge | Cardiac disease, diabetes | SC/oral |
| Indomethacin | <32 weeks, short course | >32 weeks, renal disease | Oral/rectal |
| Magnesium sulphate | <32 weeks (neuroprotection) | Myasthenia gravis, renal failure | IV infusion |
Remember: concurrent betamethasone (12 mg IM × 2 doses, 24 hours apart) or dexamethasone for fetal lung maturation is the primary treatment goal — tocolysis is the adjunct.
PPH Pharmacological Management Algorithm
Self-Assessment: Uterine Drug Clinical Scenarios
Test your uterine pharmacology decision-making with these scenarios:
Scenario A: A 30-year-old G2P1 woman delivers vaginally. Post-delivery, she has a blood loss of 800 mL and a flabby uterus. She is known to have mild asthma (well-controlled, on salbutamol PRN). BP is 110/70 mmHg. She has already received oxytocin 10 IU IM at delivery. The uterus remains poorly contracted. What is your next uterotonic and why? What would you specifically NOT give and why?
Answer: Ergometrine 0.5 mg IM — BP is normal (110/70), no hypertension contraindication; ergometrine's tetanic action may arrest the haemorrhage. If no response: misoprostol 1000 mcg sublingual (safe in asthma — PGE1 does not cause bronchoconstriction). Do NOT give carboprost (PGF2α) — asthma is an absolute contraindication; PGF2α causes bronchoconstriction; life-threatening bronchospasm risk.
Scenario B: A 26-year-old woman at 30 weeks gestation presents with regular uterine contractions every 7 minutes, cervix 2 cm dilated. Fetal wellbeing is normal. She has no prior medical history. You decide to start tocolytic therapy. Which drug is first-line and what is the goal of tocolysis?
Answer: Nifedipine — first-line oral tocolytic, most commonly used globally (cost-effective, oral, well-tolerated). Loading dose 20–30 mg oral, then 10–20 mg TDS–QDS. Goal: delay delivery by 24–48 hours to allow betamethasone 12 mg IM × 2 doses (24 hours apart) to reduce fetal RDS risk and neonatal mortality. Tocolysis is not used to prevent preterm birth indefinitely — its primary purpose is steroid window. Add magnesium sulphate (IV infusion) for fetal neuroprotection at 30 weeks (reduces cerebral palsy risk — MRC Magnet trial).
SELF-CHECK
Which tocolytic agent also provides fetal neuroprotection and reduces the risk of cerebral palsy in preterm infants <32 weeks gestation?
A. A. Nifedipine (calcium channel blocker)
B. B. Atosiban (oxytocin receptor antagonist)
C. C. Magnesium sulphate
D. D. Indomethacin (NSAID)
Reveal Answer
Answer: C. C. Magnesium sulphate
Magnesium sulphate has a dual role in preterm labour: tocolysis AND fetal neuroprotection. At the neurological level, Mg²⁺ acts as an NMDA receptor antagonist, reducing excitotoxic injury to the preterm brain during the vulnerable period of delivery. Multiple RCTs and meta-analyses confirm that magnesium sulphate reduces the risk of cerebral palsy and serious motor dysfunction in infants born <32 weeks. This neuroprotective indication (typically 4 g IV loading dose, then 1 g/hour infusion) is now WHO-recommended for preterm birth at <32 weeks. Nifedipine, atosiban, and indomethacin are tocolytics only — no established neuroprotective benefit.