Page 27 of 36
PH7.9 | PH7.9 | Infertility Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Describe the mechanism of action of clomiphene citrate and letrozole in ovulation induction
- Classify infertility drugs and match them to the appropriate level of HPO axis intervention
- Explain why exogenous testosterone should NOT be used in male infertility
- Describe the clinical features, risk factors, and management principles of ovarian hyperstimulation syndrome (OHSS)
- Apply the pharmacological ladder for PCOS-associated anovulatory infertility
INSTRUCTIONS
Infertility affects approximately one in six couples globally and is a major source of psychological distress. Pharmacological treatments — from the simple SERM clomiphene to complex IVF gonadotropin protocols — have enabled millions of couples to achieve pregnancy. This guide covers the mechanisms, clinical uses, and adverse effects of infertility drugs with emphasis on the PCOS algorithm, the OHSS hazard, and the critical misconception that testosterone helps male infertility.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 22 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 44 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A couple presents after two years of trying to conceive. The wife has irregular periods (cycles 40–60 days) with confirmed anovulation on progesterone assay. PCOS is diagnosed on ultrasound. The husband's semen analysis shows oligospermia (8 million/mL, motility 35%). The husband's brother-in-law has been prescribing him 'testosterone booster' injections from a gym supplement provider for the past three months. Today's LH, FSH, and testosterone check reveals: LH undetectable, FSH undetectable, testosterone elevated. The husband's problem is now pharmacologically compounded. Who needs which drug, and why did the testosterone injections make things worse for the couple — not better?
WHY THIS MATTERS
Infertility drug pharmacology sits at the intersection of endocrinology, reproductive medicine, and pharmacodynamics. Clomiphene citrate and letrozole — two drugs with entirely different mechanisms but overlapping indications — are among the most prescribed drugs in gynaecological practice. Understanding the difference between a SERM (clomiphene — acting at the hypothalamus) and an aromatase inhibitor (letrozole — acting peripherally to reduce oestrogen) reveals why letrozole is now preferred for PCOS. The testosterone trap in male infertility is a pharmacologically fundamental teaching point: anabolic hormones that should 'boost' spermatogenesis actually destroy it via HPG axis suppression.
RECALL
Female reproduction is governed by the HPO axis: pulsatile GnRH from the hypothalamus → FSH and LH from the pituitary → follicular development and oestrogen secretion by the ovaries. Rising oestrogen provides negative feedback on FSH/LH (keeping levels proportionate) — until the dominant follicle reaches maturation (~18 mm), when oestrogen switches to positive feedback triggering the LH surge → ovulation. After ovulation, the corpus luteum secretes progesterone for luteal phase support. Prolactin is tonically inhibited by dopamine from the hypothalamus. Excess prolactin inhibits GnRH pulsatility → anovulation. Aromatase in peripheral adipose tissue converts androgens (testosterone, androstenedione) → oestrogen. In PCOS: hyperandrogenism (from insulin-stimulated ovarian androgen production) → excess peripheral aromatisation → elevated oestrogen → excess negative feedback on FSH → arrested follicular development. In males: testosterone is produced by Leydig cells under LH stimulation; spermatogenesis in Sertoli cells requires FSH and high intratesticular testosterone from adjacent Leydig cells. Exogenous testosterone suppresses LH (and thus intratesticular testosterone from Leydig cells) → impaired spermatogenesis.
Causes of Infertility: Drug Targets
Understanding the cause of infertility is the prerequisite to pharmacological intervention — each aetiological category has a distinct pharmacological target.
Female infertility causes and drug targets:
- Anovulation (most common, ~35% of female factor): The most pharmacologically tractable — directly targeted by ovulation-inducing drugs. Sub-causes: (a) PCOS — hyperandrogenism + insulin resistance → arrested folliculogenesis → target with insulin sensitisers (metformin) + ovulation inducers (letrozole, clomiphene); (b) hyperprolactinaemia → GnRH inhibition → anovulation → target with dopamine agonists (bromocriptine/cabergoline); (c) hypogonadotropic hypogonadism (Kallmann syndrome, excessive exercise, eating disorders) — low FSH/LH → no follicular stimulation → target with pulsatile GnRH or exogenous gonadotropins.
- Tubal factor (20–30%): Pharmacologically managed (treat underlying PID) but primarily surgical.
- Uterine factor (10–15%): Pharmacologically managed (progesterone for luteal phase defect in ART).
- Unexplained infertility (20–25%): Empirical ovulation induction ± IUI.
Male infertility causes and drug targets:
- Hypogonadotropic hypogonadism (secondary): low LH/FSH → low testosterone → poor spermatogenesis → target with gonadotropins (hCG for testosterone, rFSH for spermatogenesis) or pulsatile GnRH.
- Hyperprolactinaemia: prolactin inhibits LH → low testosterone → target with dopamine agonists.
- Idiopathic oligospermia: empirical anti-oestrogens (clomiphene) — increases LH/FSH → increases intratesticular testosterone → may improve spermatogenesis; evidence modest.
- Obstructive azoospermia: surgical (sperm extraction for ICSI).
Therapeutic Goals: Restoring Fertility at the Right Level of the Axis
The pharmacological goal in infertility is to intervene at the specific pathological level of the reproductive axis — not to simply flood the system with gonadotropins. Matching drug to level prevents both under-treatment (no ovulation) and over-treatment (ovarian hyperstimulation syndrome).
The pharmacological ladder for female anovulatory infertility (PCOS):
1. Lifestyle + metformin: BMI reduction by 5–10% can restore spontaneous ovulation in obese PCOS. Metformin reduces insulin resistance → reduces androgen excess → may restore menstrual regularity without further drugs. 3–6-month trial before pharmacological ovulation induction.
2. Letrozole first-line (PCOSACT trial — NEJM 2014): 2.5–5 mg orally days 3–7 of cycle. Higher live birth rates than clomiphene in PCOS. Preferred because of superior endometrial receptivity (no anti-oestrogenic endometrial effect).
3. Clomiphene citrate: 50–150 mg days 3–7; second-line for PCOS; still widely used where letrozole access is limited.
4. Gonadotropins (rFSH ± LH): For clomiphene/letrozole-resistant PCOS or normogonadotropic anovulation; highest efficacy but highest OHSS risk; requires ultrasound monitoring.
5. ART (IVF/ICSI): For failed ovulation induction, tubal factor, severe male factor.
Male infertility pharmacological goals:
- Goal of restoring spermatogenesis requires ENDOGENOUS testosterone (high intratesticular concentration from Leydig cells), NOT exogenous testosterone (which suppresses LH → reduces intratesticular T → impairs spermatogenesis). This is the pharmacological trap.
- For hypogonadotropic male infertility: hCG (2500–5000 IU IM 3× weekly) stimulates Leydig cells → intratesticular testosterone ↑; then add rFSH to stimulate Sertoli cells → spermatogenesis. Continue for 6–18 months.
SELF-CHECK
A 32-year-old man with oligospermia visits a fertility clinic. He has been taking exogenous testosterone injections (prescribed by a gym trainer) for 6 months. His LH and FSH are undetectable. The most appropriate next step is:
A. A. Increase testosterone dose — his semen parameters haven't improved because the dose is too low
B. B. Stop exogenous testosterone immediately — the HPG suppression is directly causing azoospermia; recovery requires 6–18 months off testosterone
C. C. Add FSH injections while continuing testosterone
D. D. Start clomiphene while continuing testosterone to stimulate FSH production
Reveal Answer
Answer: B. B. Stop exogenous testosterone immediately — the HPG suppression is directly causing azoospermia; recovery requires 6–18 months off testosterone
Exogenous testosterone suppresses LH and FSH via negative feedback on the hypothalamus and pituitary. Low LH → Leydig cells stop producing intratesticular testosterone. Low FSH → Sertoli cells cannot support spermatogenesis. The result is exogenous-testosterone-induced azoospermia/severe oligospermia — paradoxical when testosterone appears elevated in serum (from the injection) but intratesticular levels are suppressed. Recovery after stopping testosterone may take 6–18 months as the HPG axis recovers. Adding FSH while continuing exogenous testosterone is ineffective (LH still suppressed → intratesticular T deficient). Clomiphene works by increasing endogenous LH/FSH — incompatible with continued exogenous testosterone (which will continue to suppress LH/FSH).
Drug Classification: Ovulation Inducers, Gonadotropins, and Adjuncts
Infertility drugs work at different levels of the HPO axis — from the central hypothalamus/pituitary (clomiphene, GnRH pump) to the ovary directly (gonadotropins) to peripheral tissues (letrozole, metformin).
Selective Oestrogen Receptor Modulators (SERMs) — Clomiphene Citrate: Acts as an anti-oestrogen at the hypothalamus and pituitary — blocks oestrogen negative feedback → hypothalamus increases GnRH pulse frequency → pituitary releases more FSH (and LH) → ovarian follicular recruitment and development → ovulation. Think of clomiphene as 'unblocking the brake' on FSH secretion. It does NOT directly stimulate the ovary — the ovary responds to the now-higher FSH. Dose: 50–150 mg/day orally days 3–7 of cycle. Anti-oestrogenic effects on the endometrium and cervical mucus (disadvantages vs letrozole): thinner endometrium (reduced implantation potential) and thicker, less favourable cervical mucus.
Aromatase Inhibitors — Letrozole: Inhibits aromatase enzyme in peripheral adipose tissue (and the ovary) → reduces oestrogen synthesis from androgen precursors → reduced oestrogen-mediated negative feedback on FSH → FSH rises → follicular recruitment. Key advantages over clomiphene for PCOS: (1) no anti-oestrogenic endometrial effect — endometrium is receptive; (2) shorter half-life → cleared before the implantation window; (3) PCOSACT trial (NEJM 2014): higher live birth rate (27.5% vs 19.1%) and fewer multiple gestations than clomiphene in PCOS. Dose: 2.5–5 mg days 3–7.
Gonadotropins: Recombinant FSH (follitropin alpha/beta), recombinant LH, urinary-derived FSH (urofollitropin), and hCG (human chorionic gonadotropin — LH-like activity). Used when clomiphene/letrozole fail or for controlled ovarian stimulation in ART. hCG (5000–10,000 IU IM/SC) — triggers the LH surge equivalent to mature follicle release — given when dominant follicle ≥18 mm on ultrasound. OHSS risk — highest with gonadotropins.
Dopamine Agonists — Bromocriptine/Cabergoline: For hyperprolactinaemia-induced anovulation — reducing prolactin restores GnRH pulsatility → FSH/LH recover → ovulation resumes. Effective in 70–80% of patients. For most women with hyperprolactinaemia-related anovulation, bromocriptine/cabergoline alone restores fertility without additional ovulation inducers.
Metformin: In PCOS — reduces insulin resistance → reduces LH-stimulated ovarian androgen production → reduces androgen excess → may restore menstrual regularity. As adjunct to letrozole/clomiphene in insulin-resistant PCOS — may improve response. Not an ovulation inducer per se — corrects the metabolic substrate.
Pulsatile GnRH (subcutaneous pump): For hypogonadotropic hypogonadism in women — pulsatile GnRH mimics physiological hypothalamic release → stimulates FSH/LH → follicular development. Risk of OHSS lower than gonadotropin protocols but technically demanding.
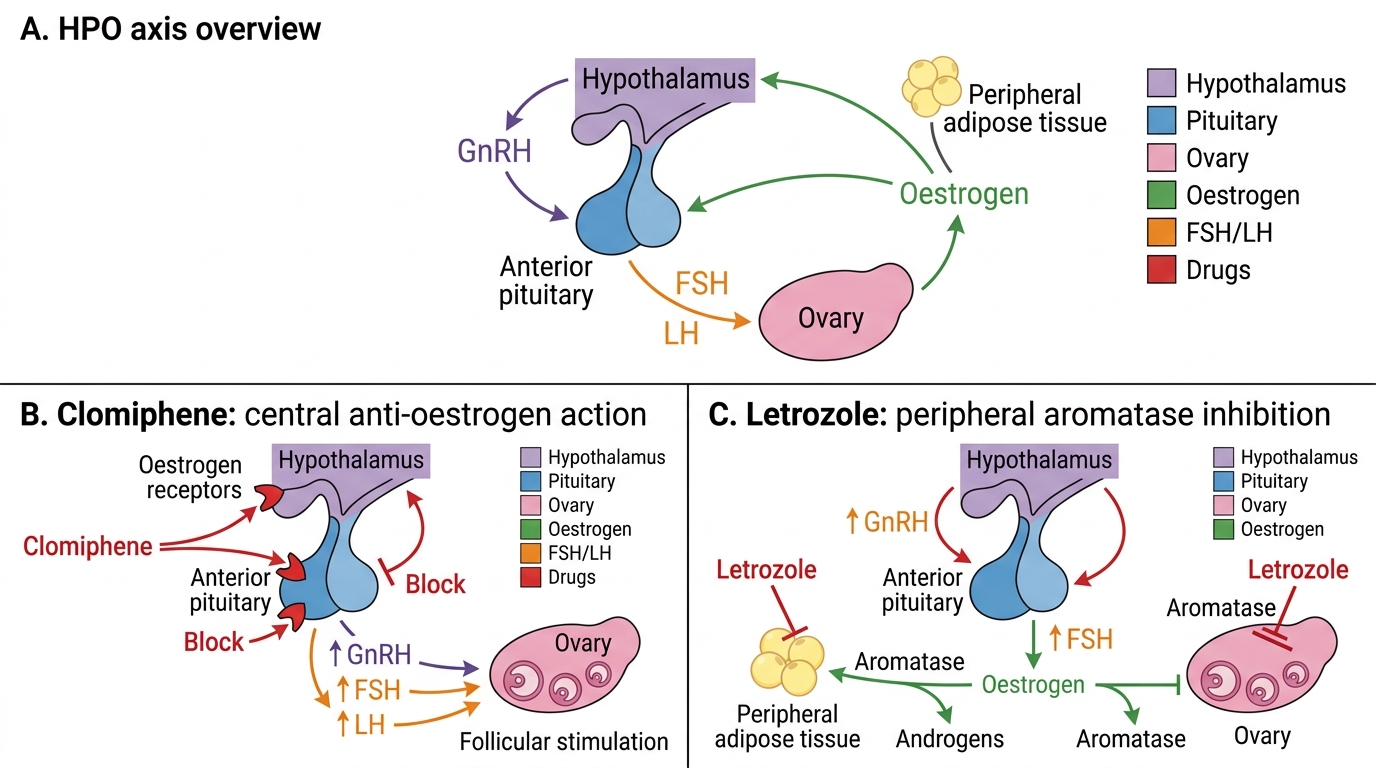
Clomiphene versus Letrozole in the HPO Axis