Page 28 of 36
PH7.9 | PH7.9 | Infertility Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Mechanisms, PK, and Clinical Uses of Each Drug Class
The pharmacokinetic properties of infertility drugs determine their timing relative to the menstrual cycle and their adverse effect profiles.
Provided image
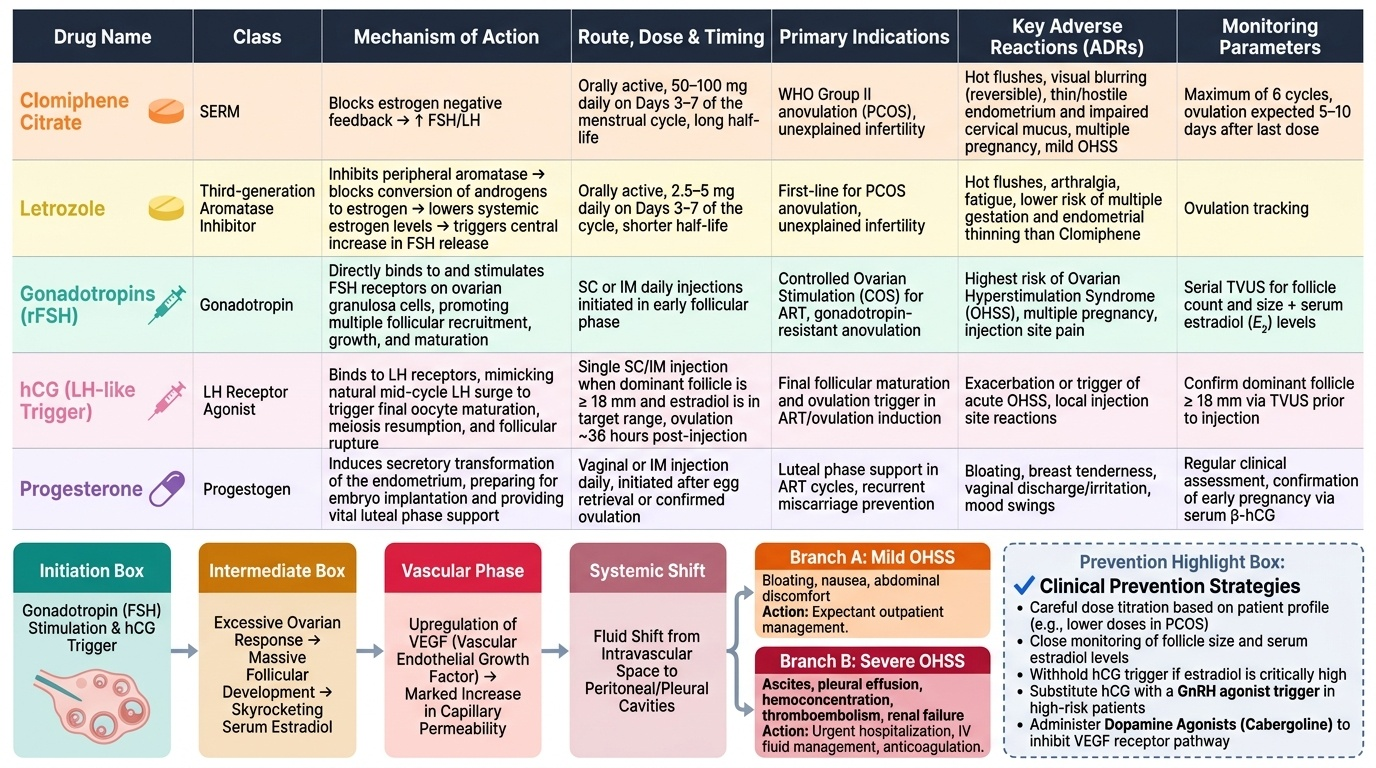
Clomiphene citrate PK: Orally active; long half-life (~5–7 days for the zuclomiphene isomer); taken days 3–7 of cycle; ovulation expected 5–10 days after the last dose. The long half-life contributes to its anti-oestrogenic endometrial and cervical mucus effects throughout the cycle (negative side effects vs letrozole). Maximum 6 cycles (debated risk of ovarian cancer with longer use).
Letrozole PK: Orally active; shorter half-life (~2 days) — cleared before the implantation window. No cumulative anti-oestrogenic effect on endometrium. Days 3–7 of cycle. Ovulation 5–10 days after last dose.
Gonadotropin protocols (ART): Daily SC or IM injections. Monitoring: transvaginal ultrasound (follicle count and size every 2–3 days) + serum oestradiol levels. hCG trigger when dominant follicle ≥18 mm AND oestradiol within acceptable range. Progesterone supplementation after ovulation/egg retrieval for luteal phase support (vaginal micronised progesterone or IM progesterone). OHSS (Ovarian Hyperstimulation Syndrome): complication of gonadotropin (and clomiphene) therapy — excessive ovarian response to FSH stimulation → multiple follicle development → high oestradiol → vascular permeability increases (via VEGF) → fluid shifts from intravascular to peritoneal space. Mild (bloating, nausea, abdominal discomfort): expectant management. Severe (ascites, pleural effusion, haemoconcentration, thromboembolism, renal failure): hospitalisation, careful IV fluids, anticoagulation. Prevention: careful dose titration, ultrasound monitoring, withhold hCG trigger if OHSS risk high, use GnRH agonist trigger instead of hCG in high-risk cycles, dopamine agonists (cabergoline) reduce OHSS in high-risk patients.
| Drug | Class | Mechanism | Indication | ADR |
|---|---|---|---|---|
| Clomiphene | SERM (anti-oestrogen) | Blocks oestrogen −ve feedback → ↑FSH/LH | PCOS anovulation, unexplained | OHSS, visual blurring, thin endometrium, multiple pregnancy |
| Letrozole | Aromatase inhibitor | ↓ Peripheral oestrogen → ↑FSH centrally | PCOS (preferred), unexplained | OHSS (less than clomiphene), arthralgia, hot flushes |
| rFSH | Gonadotropin | Directly stimulates follicular development | ART, gonadotropin-resistant cases | OHSS (highest risk) |
| hCG | LH-like trigger | Triggers ovulation of mature follicle | ART (trigger) | OHSS risk (worsens if overstimulated) |
| Bromocriptine | Dopamine agonist (D2) | ↓ Prolactin → restores GnRH pulsatility | Hyperprolactinaemia anovulation | Nausea, postural hypotension |
| Metformin | AMPK activator | ↓ Insulin resistance in PCOS | PCOS (adjunct) | GI, lactic acidosis (rare) |
CLINICAL PEARL
Letrozole has dethroned clomiphene as first-line for PCOS anovulation. The PCOSACT trial (NEJM 2014) demonstrated that letrozole achieves significantly higher live birth rates (27.5% vs 19.1%) and fewer multiple gestations than clomiphene in women with PCOS. The mechanistic advantage: letrozole has a short half-life (cleared by the implantation window), produces no anti-oestrogenic endometrial thinning, and does not impair cervical mucus. Clomiphene's anti-oestrogenic peripheral effects — while stimulating the ovary centrally — simultaneously impair the uterine environment needed for implantation. However, clomiphene remains widely used in India and is the first ovulation inducer most students will encounter clinically. Know both, but know which is now preferred.
SELF-CHECK
Why is letrozole preferred over clomiphene citrate for ovulation induction in PCOS according to current evidence?
A. A. Letrozole is cheaper and more widely available than clomiphene
B. B. Letrozole directly stimulates ovarian follicles without requiring FSH
C. C. Letrozole has a shorter half-life and no anti-oestrogenic effect on the endometrium, resulting in better implantation rates and higher live birth rates (PCOSACT trial)
D. D. Letrozole is safer in multiple gestation — fewer twins than clomiphene
Reveal Answer
Answer: C. C. Letrozole has a shorter half-life and no anti-oestrogenic effect on the endometrium, resulting in better implantation rates and higher live birth rates (PCOSACT trial)
Letrozole is preferred over clomiphene in PCOS for mechanistic reasons confirmed by the PCOSACT trial (NEJM 2014): (1) short half-life — cleared before implantation, no sustained anti-oestrogenic effect; (2) endometrial receptivity is preserved — oestrogen is allowed to act on the endometrium during the implantation window (unlike clomiphene, which blocks ER throughout); (3) cervical mucus is not impaired. The result: higher live birth rates in the PCOSACT trial. Option D is partly correct (fewer multiple gestations) but not the primary pharmacological reason for preference. Letrozole is NOT cheaper — it is actually more expensive than generic clomiphene. Letrozole does not directly stimulate the ovary — it reduces oestrogen → increases FSH → follicular response.
Clinical Decision-Making: Tailoring Infertility Pharmacotherapy
Rational infertility pharmacotherapy integrates the diagnosis (which level of axis is disrupted?) with the patient's age, ovarian reserve, BMI, and access to monitoring resources.
PCOS-associated anovulatory infertility (most common clinical scenario):
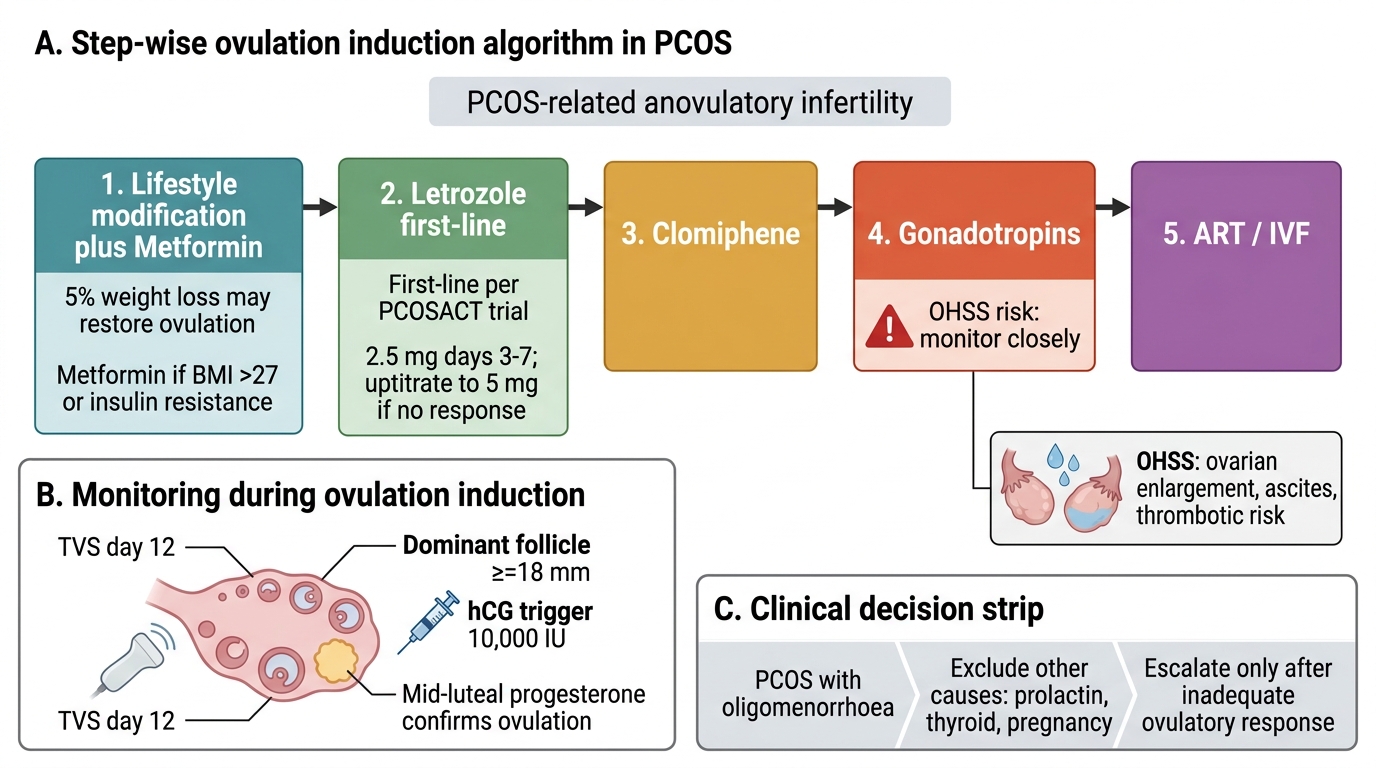
Step 1: Lifestyle modification (3–6 months) — 5–10% weight loss in overweight/obese PCOS restores spontaneous ovulation in ~55% of women. Concurrent metformin 500–1500 mg/day: reduces insulin resistance, lowers androgens, may restore menstrual regularity.
Step 2: Letrozole 2.5–5 mg days 3–7 (first-line per PCOSACT trial). Monitor with ultrasound. If no dominant follicle by day 12: consider increasing to 5 mg (next cycle). If follicle ≥18 mm: administer hCG 5000–10,000 IU to trigger ovulation.
Step 3: Clomiphene 50–150 mg (second-line or where letrozole is unavailable). Monitor similarly. Combine with IUI in unexplained infertility.
Step 4: Gonadotropins (FSH injections) — for clomiphene/letrozole-resistant PCOS. Requires intensive ultrasound + oestradiol monitoring. OHSS risk highest here — start with low dose ('low-and-slow' protocol).
Step 5: IVF — for failed ovulation induction, tubal factor, severe male factor.
Hyperprolactinaemia-induced anovulation:
First-line: Cabergoline 0.5–3 mg weekly (preferred — higher efficacy, fewer ADRs, weekly dosing). Prolactin normalisation in >80% → GnRH pulsatility restored → spontaneous ovulation resumes in most women. No ovulation inducers needed in most cases. Stop cabergoline after confirmed pregnancy (safety in early pregnancy: extensive data support, but consult specialist).
Hypogonadotropic hypogonadism (female):
Pulsatile GnRH pump (SC, 60–90 min intervals) OR gonadotropin injections (FSH + LH). Goal: mono-follicular development (LH/FSH levels carefully titrated — less OHSS risk with GnRH pump).
Male infertility management:
- Hypogonadotropic hypogonadism: hCG 2500–5000 IU SC 3× weekly × 3–6 months → intratesticular testosterone rises → then add rFSH 75–150 IU SC 3× weekly → spermatogenesis. Treatment duration: 6–18 months.
- Idiopathic oligospermia: empirical clomiphene (anti-oestrogen → increases LH/FSH → increases intratesticular T → may improve sperm parameters). Evidence modest. CRITICAL: never use exogenous testosterone — it worsens spermatogenesis.
- Hyperprolactinaemia: dopamine agonist (cabergoline) → LH/FSH restored → testosterone and spermatogenesis recover.
PCOS Anovulatory Infertility: Step-wise Pharmacologic Algorithm
Self-Assessment: Infertility Pharmacology Scenarios
Consolidate your infertility pharmacology understanding with these scenarios:
Scenario A: A 28-year-old woman with PCOS has been trying to conceive for 18 months. BMI 29. She ovulates infrequently (cycles 45–60 days). AMH is elevated (PCOS marker). What is your first-line ovulation induction drug, and what monitoring is required?
Answer: Letrozole 2.5 mg days 3–7 — first-line for PCOS ovulation induction per PCOSACT trial. If no response: uptitrate to 5 mg next cycle. Monitoring: transvaginal ultrasound day 12 (dominant follicle ≥18 mm triggers hCG 10,000 IU); mid-luteal progesterone to confirm ovulation. Offer metformin concurrently (500 mg BD increasing to 1500 mg/day) if BMI >27 or insulin resistance markers present. Lifestyle modification counselling — 5% weight loss may itself restore ovulation.
Scenario B: A 34-year-old woman has oligomenorrhoea, galactorrhoea, and serum prolactin of 142 ng/mL (normal <25 ng/mL). MRI shows a microprolactinoma. She wants to conceive. What do you prescribe?
Answer: Cabergoline 0.5 mg twice weekly — first-line for prolactinoma and hyperprolactinaemia-induced anovulation. Cabergoline is preferred over bromocriptine (higher prolactin normalisation rate, weekly dosing, fewer ADRs). Prolactin should normalise within 4–8 weeks → menstrual cycles restored → spontaneous ovulation returns in most patients. Additional ovulation inducers (letrozole/clomiphene) are usually NOT needed once prolactin is normalised. Monitor: monthly prolactin until normal, then 6-monthly; annual MRI for tumour response. Once pregnant, cabergoline is typically stopped (specialist decision).
SELF-CHECK
Which statement correctly describes clomiphene citrate's mechanism of action in ovulation induction?
A. A. Clomiphene directly stimulates ovarian follicles to produce oestrogen and mature
B. B. Clomiphene blocks oestrogen receptors at the hypothalamus and pituitary, reducing negative feedback and increasing endogenous FSH secretion
C. C. Clomiphene inhibits aromatase, reducing peripheral oestrogen and increasing FSH
D. D. Clomiphene stimulates the posterior pituitary to release FSH and LH directly
Reveal Answer
Answer: B. B. Clomiphene blocks oestrogen receptors at the hypothalamus and pituitary, reducing negative feedback and increasing endogenous FSH secretion
Clomiphene is a SERM (selective oestrogen receptor modulator) that acts as an anti-oestrogen at the hypothalamus and anterior pituitary. By blocking oestrogen receptors at these sites, it prevents oestrogen from exerting its normal negative feedback on GnRH/FSH/LH secretion. The result: FSH and LH rise → follicular recruitment and development → ovulation in anovulatory women. Clomiphene does not act directly on the ovary — it acts centrally, and the ovary responds to the elevated FSH. Option C describes letrozole's mechanism (aromatase inhibition). Clomiphene does not stimulate the posterior pituitary (which produces oxytocin and ADH, not FSH/LH — FSH/LH are anterior pituitary products).