Page 17 of 26
PH6.5 | PH6.5 | Chronic Lower-GI Symptom Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Distinguish Inflammatory Bowel Disease (IBD) from Irritable Bowel Syndrome (IBS) in terms of pathophysiology and pharmacological approach
- Classify IBD drugs (aminosalicylates, corticosteroids, thiopurines, biologics, JAK inhibitors) and explain why each class is appropriate for its clinical indication
- Identify the critical pre-treatment safety requirements for azathioprine (TPMT testing) and anti-TNF biologics (TB screening)
- Select appropriate pharmacotherapy for IBS by subtype (IBS-D, IBS-C, IBS with pain)
- Construct a stepwise management plan for mild-moderate UC and for moderate-severe Crohn's disease
INSTRUCTIONS
Inflammatory Bowel Disease and Irritable Bowel Syndrome are among the most important chronic lower gastrointestinal conditions you will encounter in clinical practice — and they are frequently confused by students (and sometimes by clinicians). IBD requires anti-inflammatory and immunosuppressive therapy targeting real mucosal inflammation and immune dysregulation; IBS is a functional disorder requiring symptom management without immunosuppression. Confusing the two leads to under-treatment of IBD (with serious complications — strictures, colorectal cancer) and over-treatment of IBS (with unnecessary immunosuppression). This module keeps the two disease pharmacologies strictly separated while building a coherent clinical framework for each.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 50 (Inflammatory Bowel Disease) + Ch. 49 (IBS management) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch. 47 (IBD Pharmacotherapy) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients sit in the gastroenterology outpatient clinic, both complaining of 'chronic stomach pain and diarrhoea' for the past year. The first is a 24-year-old woman with bloody diarrhoea, 10 stools per day, fever, and a CRP of 85 mg/L — colonoscopy shows continuous mucosal inflammation from rectum to splenic flexure. The second is a 32-year-old man with intermittent loose stools and cramping that worsen with stress, no blood, normal colonoscopy, normal CRP, and bloating that fluctuates with diet. The first patient has ulcerative colitis — she needs mesalazine and possibly a corticosteroid for her flare, with thiopurines or biologics for maintenance. The second has IBS-D — he needs mebeverine for cramps, loperamide on demand, and a low-FODMAP dietary assessment. Same presenting symptoms, completely different pharmacology. By the end of this module, you will confidently manage both.
WHY THIS MATTERS
IBD (Crohn's disease and ulcerative colitis) is rising in prevalence in India — historically thought to be a Western disease, India is now experiencing an epidemiological transition with increasing incidence, particularly in urban populations. Undertreated IBD causes hospitalisation, bowel resection, colorectal cancer (especially in long-standing UC), and reduced quality of life. The advent of biological therapies (anti-TNF antibodies, vedolizumab, ustekinumab) has transformed outcomes for patients who were previously steroid-dependent or required surgery — but these drugs carry serious risks (opportunistic infections, reactivation of latent TB) that require pre-treatment screening, which you must know. IBS affects 10–15% of the global population and is the most common reason for GI specialist referral. While less acutely dangerous than IBD, it causes significant disability and healthcare utilisation. Understanding both conditions — and confidently distinguishing them — is essential for managing the enormous burden of lower GI complaints you will encounter in every clinical setting.
RECALL
From your Year-1 immunology and physiology, recall that the gut mucosa is under constant immune surveillance — innate immunity (macrophages, Paneth cells, defensins) and adaptive immunity (T-cell subsets, IgA) maintain a tolerant equilibrium with the normal commensal flora while defending against pathogens. IBD represents a failure of this equilibrium: in genetically susceptible individuals (NOD2 mutations in CD, others), mucosal immune dysregulation leads to chronic, sustained activation of pro-inflammatory pathways — particularly TNF-α (activates NF-κB → cytokine cascade), IL-12/23 (drives Th1 and Th17 responses), and lymphocyte homing via integrins (α4β7 on gut-homing T-cells). IBS involves no such organic inflammation — instead, there is altered gut-brain axis signalling, visceral hypersensitivity (lowered pain threshold to luminal distension), altered serotonin signalling in the gut (enterochromaffin cells), and dysbiosis (altered microbiome composition without macroscopic mucosal damage). Recall that serotonin (5-HT) plays a key role in both intestinal motility regulation (5-HT4 → prokinetic; 5-HT3 → pain/secretion) and gut-brain communication — the pharmacological basis of antidepressant use in IBS.
Pathophysiology of IBD and IBS — Two Distinct Diseases
The fundamental distinction between Inflammatory Bowel Disease and Irritable Bowel Syndrome is the presence or absence of organic mucosal inflammation — a distinction with direct and profound pharmacological consequences that must be established before any prescription is written. Treating IBD as if it were IBS (symptomatic management without addressing the underlying mucosal inflammation) leads to disease progression, stricture formation, fistula development, and ultimately surgery or colorectal cancer. Treating IBS as if it were IBD (immunosuppression without organic inflammation) exposes the patient to serious drug toxicities — corticosteroid osteoporosis, thiopurine myelosuppression, biologic-induced opportunistic infections — without any therapeutic benefit. This pathophysiological distinction is the pharmacological fork in the road that every management decision in this module follows.
The fundamental distinction between IBD and IBS is the presence or absence of organic mucosal inflammation — a distinction with direct and profound pharmacological consequences. Treating IBD as if it were IBS (symptomatic management without addressing inflammation) leads to disease progression, complications, and ultimately surgery or colorectal cancer. Treating IBS as if it were IBD (immunosuppression without organic inflammation) exposes the patient to serious drug toxicities without benefit. Every prescribing decision in this module flows from correctly making this distinction first.
Inflammatory Bowel Disease (IBD): A group of chronic, relapsing-remitting inflammatory conditions of the GI tract driven by immune dysregulation:
- Ulcerative colitis (UC): Inflammation confined to the colonic mucosa (never transmural, never small bowel), continuous from the rectum proximally to varying extents — proctitis (rectum only), left-sided colitis (to splenic flexure), or pancolitis (entire colon). Hallmarks: bloody diarrhoea, rectal urgency, tenesmus; colonoscopy shows loss of vascular pattern, granularity, friability, pseudopolyps. Complications: toxic megacolon, colorectal cancer (risk rises with duration and extent; 20 years of pancolitis → 8% absolute risk). UC is never in the small bowel.
- Crohn's disease (CD): Transmural inflammation (full thickness of gut wall) that can affect any part of the GI tract from mouth to anus, characteristically with skip lesions (diseased segments separated by normal mucosa), cobblestone mucosa, fistulae (between gut segments, gut and skin, gut and bladder), and granulomas on histology. Complications: strictures (from transmural fibrosis), fistulae, abscesses, perianal disease, malabsorption (especially terminal ileal CD → B₁₂ deficiency, fat-soluble vitamin malabsorption).
Irritable Bowel Syndrome (IBS): A functional gastrointestinal disorder characterised by recurrent abdominal pain associated with defaecation or changes in stool frequency/consistency, with no structural or biochemical abnormality identifiable by investigation (colonoscopy normal, CRP normal, faecal calprotectin negative). The pathophysiology involves altered gut-brain axis, visceral hypersensitivity (lowered pain threshold to luminal distension, likely via upregulated TRPV1 channels and sensitised submucosal sensory neurones), altered serotonin signalling (abnormal enterochromaffin cell 5-HT release), and gut microbiome dysbiosis.
IBS subtypes: IBS-D (diarrhoea-predominant — loose, frequent stools, urgency, no blood); IBS-C (constipation-predominant — infrequent hard stools, bloating); IBS-M (mixed — alternating diarrhoea and constipation); IBS-U (unspecified).
The pharmacological fork: IBD → anti-inflammatory/immunosuppressive drugs. IBS → symptom-targeted drugs (motility, pain, microbiome) with NO immunosuppression.
Therapeutic Goals — IBD and IBS
The therapeutic goals for IBD and IBS differ fundamentally, reflecting their different pathophysiologies. Setting the correct goal is not semantic — it drives drug choice, duration, and the definition of treatment success.
For IBD, the modern therapeutic goals have shifted from purely symptom-based relief (clinical remission) to objective mucosal-level targets: mucosal healing (endoscopic remission) is now the primary treatment endpoint, because patients who achieve mucosal healing have lower rates of hospitalisation, surgery, and colorectal cancer than those who achieve only symptom remission. The therapeutic strategy is therefore 'treat-to-target' — escalate therapy until endoscopic healing is confirmed, not just until symptoms improve.
Specific goals: (1) induce clinical remission (reduce diarrhoea, rectal bleeding, pain); (2) achieve mucosal healing (endoscopic); (3) maintain steroid-free remission — avoiding long-term corticosteroids (ADR profile including bone loss, infection risk, metabolic effects); (4) prevent complications (strictures, fistulae, colorectal cancer); (5) improve quality of life and maintain nutritional status.
For IBS, there is no structural lesion to heal and no inflammatory target to suppress. The goal is symptom control — reducing abdominal pain, normalising stool consistency and frequency, and improving quality of life. Because IBS is a chronic, fluctuating condition and symptoms are subjective, treatment success is defined as improvement in the patient's own symptom scores over ≥4-week periods. The Rome IV composite endpoint (abdominal pain reduction ≥30% + stool abnormality improvement ≥50%) is the regulatory standard for IBS drug trials. The key philosophical difference from IBD: there is no disease progression or cancer risk in IBS — so the goal is improving daily functioning, not preventing structural damage.
SELF-CHECK
A 28-year-old woman with recently diagnosed ulcerative colitis (left-sided, moderate severity) is started on mesalazine. After 8 weeks, her symptoms have improved significantly — she reports normal stool frequency and no bleeding. Colonoscopy is scheduled. What is the CORRECT interpretation of 'treatment success' in this setting?
A. Symptom remission is sufficient — colonoscopy is not needed if she feels better
B. Symptom remission is necessary but not sufficient — colonoscopy must confirm mucosal healing for optimal long-term outcomes
C. She should be stepped up to azathioprine regardless, as mesalazine is only for induction
D. She has achieved the treatment goal — discontinue mesalazine and monitor
Reveal Answer
Answer: B. Symptom remission is necessary but not sufficient — colonoscopy must confirm mucosal healing for optimal long-term outcomes
The modern 'treat-to-target' approach to IBD requires mucosal healing as the primary endpoint, not just clinical symptom remission. Patients with UC who achieve only symptom remission but not endoscopic mucosal healing have higher rates of relapse, hospitalisation, surgery, and colorectal cancer risk compared to those with confirmed mucosal healing. Colonoscopy to confirm mucosal healing is standard practice after induction therapy. Mesalazine is used for both induction and maintenance in mild-moderate UC — it is not just for induction. Discontinuing mesalazine in a patient with UC who has achieved remission risks relapse (maintenance mesalazine halves the relapse rate).
Classification of IBD and IBS Pharmacotherapy
The pharmacological landscapes for IBD and IBS consist of two entirely distinct drug sets that must never be cross-applied or blurred in clinical practice. This classification section maintains strict separation between the two disease drug classes, because the single most dangerous error in chronic lower GI pharmacotherapy is prescribing an IBD immunosuppressant for a patient who actually has IBS (or vice versa — failing to use anti-inflammatory therapy for a patient with true IBD). Mapping every drug to its disease (IBD vs IBS), its mechanistic class, and its specific indication within that disease is the pharmacological competency that this module is designed to build.
The pharmacological landscape for IBD and IBS consists of two entirely distinct drug sets that must never be cross-applied. Because PH6.5 requires both conditions to be covered in one SDL, the risk of blurring their pharmacological boundaries is real — and it is the most important structural discipline to maintain throughout this module. Below, the two drug landscapes are presented separately and will remain separate through every subsequent section.
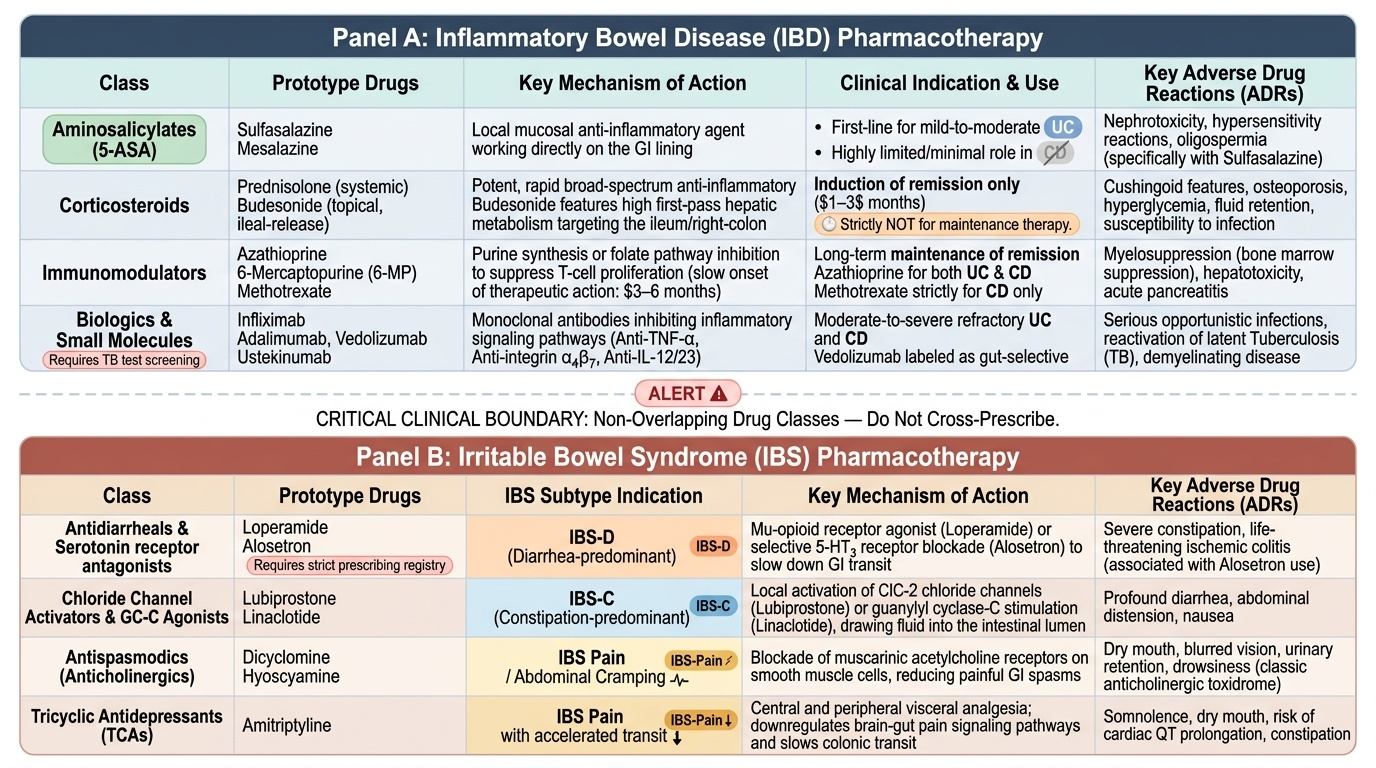
IBD pharmacotherapy — five mechanistic classes:
1. Aminosalicylates (5-ASA drugs): Sulfasalazine, mesalazine. Local mucosal anti-inflammatory agents. First-line for mild-moderate UC; limited role in CD.
2. Corticosteroids: Prednisolone (systemic, acute flares), budesonide (high first-pass metabolism, ileal/right-colonic CD). Induction only — not for maintenance.
3. Immunomodulators: Azathioprine/6-mercaptopurine (thiopurines), methotrexate (CD). Maintenance of remission; slow onset (3–6 months).
4. Biologics: Anti-TNF-α (infliximab, adalimumab), anti-integrin (vedolizumab), anti-IL-12/23 (ustekinumab). Moderate-severe disease unresponsive to conventional therapy.
5. JAK inhibitors: Tofacitinib (JAK1/3), upadacitinib (JAK1). Oral small molecules; UC and CD.
IBS pharmacotherapy — mechanism-by-subtype:
- IBS-D: Loperamide (anti-motility), low-dose amitriptyline (TCA — reduces bowel frequency + visceral pain), rifaximin (non-absorbable antibiotic, targets microbiome in SIBO-associated IBS-D).
- IBS-C: Linaclotide (GC-C agonist — secretory + analgesic), lubiprostone (ClC-2 activator — secretory). [Cross-reference: PH6.4 module.]
- IBS pain/spasm: Mebeverine (direct smooth muscle relaxant, first-line), hyoscine butylbromide (anticholinergic), peppermint oil (colonic 5-HT3 + calcium channel effect), low-dose TCA or SSRI.
Provided image