Page 18 of 26
PH6.5 | PH6.5 | Chronic Lower-GI Symptom Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Aminosalicylates and Corticosteroids — IBD
Aminosalicylates (5-ASA drugs) are the foundation of pharmacotherapy for mild-to-moderate ulcerative colitis, providing local anti-inflammatory effects at the colonic mucosa where they are most needed. Their discovery as effective IBD agents followed the observation that sulfasalazine — originally developed as a rheumatological anti-inflammatory — reduced UC symptoms; subsequent pharmacological analysis revealed that the active moiety was not the sulphonamide carrier but the 5-aminosalicylic acid (5-ASA) component released in the colon.
Sulfasalazine: An azo-bond conjugate of 5-aminosalicylic acid (5-ASA) linked to sulphapyridine (a sulphonamide). The azo bond is cleaved by colonic bacteria → free 5-ASA is released in the colon (the active anti-inflammatory site) + sulphapyridine is absorbed. Mechanism of 5-ASA: local inhibition of NF-κB signalling (reduces cytokine production in colonic epithelium and lamina propria macrophages), inhibition of 5-lipoxygenase (reduces leukotriene B₄ production — a potent neutrophil chemoattractant), inhibition of COX-2 in the mucosa, and free-radical scavenging. The 5-ASA component acts locally in the colon; minimal systemic absorption. ADRs from sulphapyridine: nausea, headache, malaise (most common, dose-related), haemolytic anaemia (particularly in G6PD-deficient patients), rarely agranulocytosis. Male infertility (reversible oligospermia from sulphapyridine — recovers within 2 months of stopping) — inform male patients of reproductive age. Inhibits folate absorption → folic acid 5 mg/day supplementation required (important for pregnant patients with UC on sulfasalazine).
Mesalazine (mesalamine = pure 5-ASA): Eliminates the sulphapyridine carrier, retaining only the active 5-ASA moiety — better tolerated with fewer ADRs. Available in formulations that deliver 5-ASA to different GI segments (pH-dependent release for ileum + colon; slow-release matrix for colon; rectal suppositories/enemas for distal disease). ADRs: generally well tolerated; rare: interstitial nephritis (renal function monitoring recommended during treatment), acute intolerance reaction (mimicking IBD flare).
Corticosteroids in IBD: Prednisolone (systemic) is used for acute flares of both UC and CD at 40 mg/day, tapering over 8–12 weeks. It rapidly suppresses intestinal inflammation but is not for maintenance — long-term steroid use causes well-known systemic toxicity (osteoporosis, hyperglycaemia, adrenal suppression, immunosuppression). Patients who require >2 steroid courses/year are considered steroid-dependent and should be offered thiopurines or biologics for maintenance. Budesonide is a corticosteroid with high first-pass hepatic metabolism (>90% extracted on first pass through the liver after absorption from the gut), dramatically reducing systemic steroid exposure compared to prednisolone. It is available in oral formulations that release in the terminal ileum and right colon — making it particularly suited for ileal/right colonic Crohn's disease. Fewer systemic ADRs than prednisolone at equivalent local anti-inflammatory doses. Not appropriate for left-sided UC or pancolitis (the drug does not reach these sites in sufficient concentration).
Immunomodulators — Thiopurines and Methotrexate
Immunomodulators are the backbone of long-term maintenance therapy for steroid-dependent IBD — the bridge between the acute anti-inflammatory effect of corticosteroids and the more potent (but more expensive and infection-risky) biologic therapies. They are not interchangeable with steroids and they do not work quickly: thiopurines take 3–6 months to reach full therapeutic effect because they act by gradually altering T-cell DNA synthesis rather than acutely suppressing cytokine production. This delayed onset is both a pharmacological reality that clinicians must communicate to patients (who may feel the drug is not working) and a practical prescribing principle: thiopurines should be started early, during a steroid course rather than as crisis rescue, to allow time to achieve effect before the steroid is tapered.
Immunomodulators are the backbone of maintenance therapy for steroid-dependent IBD — used when patients relapse on stopping corticosteroids or require >2 steroid courses per year. They do not work quickly (thiopurines take 3–6 months to reach therapeutic effect), which is why they are started alongside a steroid course rather than as rescue mono-therapy for acute flares. Their delayed onset is a common source of clinical confusion and a practical point worth understanding mechanistically.
Azathioprine (AZA) and 6-mercaptopurine (6-MP): Azathioprine is a prodrug that is converted in the gut to 6-MP by non-enzymatic hydrolysis. 6-MP is then metabolised along three competing pathways:
- TPMT (thiopurine methyltransferase) pathway → 6-methyl-MP (inactive) — the main inactivation route.
- Hypoxanthine-guanine phosphoribosyltransferase (HGPRT) pathway → 6-thioguanine nucleotides (6-TGN) — the active immunosuppressive metabolites. 6-TGN are incorporated into T-cell DNA, inhibiting de novo purine synthesis and inducing T-cell apoptosis.
- Xanthine oxidase → thiouric acid (inactive, minor).
The critical pharmacogenomic fact: TPMT activity must be measured before starting azathioprine. Patients with low/absent TPMT activity (3:300 have homozygous deficiency, ~10% are heterozygous with intermediate activity) cannot adequately inactivate 6-MP → excessive 6-TGN accumulates → severe myelosuppression (leukopenia, thrombocytopenia). TPMT-normal patients start at 2–2.5 mg/kg/day azathioprine; intermediate metabolisers start at lower doses.
ADRs: Myelosuppression (most important — requires FBC monitoring every 3 months); hepatotoxicity (LFTs monitoring); pancreatitis (rare, idiosyncratic, requires drug withdrawal); long-term: increased risk of non-melanoma skin cancers and lymphoma (especially EBV-driven hepatosplenic T-cell lymphoma in young males). Drug interaction: Allopurinol inhibits xanthine oxidase → dramatically increases 6-TGN levels → severe myelosuppression if azathioprine dose is not reduced by 75% (reduce AZA to 25% of the usual dose when used with allopurinol, or avoid co-prescription).
Methotrexate (MTX): Used for maintenance of Crohn's disease (evidence is weaker for UC). Given SC (subcutaneous) 15–25 mg weekly for CD maintenance. Mechanism: folate antagonism (inhibits DHFR) + induction of adenosine release (anti-inflammatory). ADRs: hepatotoxicity (hepatic fibrosis with cumulative dose — monitor LFTs, avoid alcohol; baseline liver biopsy if risk factors), mucositis, nausea, myelosuppression. Teratogenic (category X in pregnancy) — requires contraception during treatment AND for 3 months after stopping in both males and females. Folic acid 5 mg daily supplementation required to reduce mucositis/myelosuppression (does not reduce anti-inflammatory efficacy).
SELF-CHECK
Before starting a 30-year-old man with steroid-dependent Crohn's disease on azathioprine, which pre-treatment assessment is MOST critical for preventing a potentially fatal adverse effect?
A. Colonoscopy to confirm mucosal inflammation before starting immunosuppression
B. TPMT (thiopurine methyltransferase) activity measurement — TPMT-deficient patients accumulate toxic 6-thioguanine nucleotides causing severe myelosuppression
C. Serum infliximab level — to check whether a biologic has already been used
D. Liver biopsy — to assess baseline hepatic fibrosis before hepatotoxic drug
Reveal Answer
Answer: B. TPMT (thiopurine methyltransferase) activity measurement — TPMT-deficient patients accumulate toxic 6-thioguanine nucleotides causing severe myelosuppression
TPMT genotype/activity testing is mandatory before starting azathioprine (and 6-mercaptopurine). TPMT is the enzyme responsible for inactivating 6-thioguanine nucleotides (6-TGN), the active immunosuppressive metabolites of azathioprine. Patients with homozygous TPMT deficiency (~1 in 300 people) cannot inactivate 6-TGN, leading to accumulation and severe, potentially fatal myelosuppression (profound leukopenia and thrombocytopenia) even at standard doses. Heterozygous patients (~10% of the population, intermediate activity) require dose reduction. TPMT testing is a pharmacogenomic safety test — its omission has caused deaths. Colonoscopy is not required before starting immunosuppression. Liver biopsy is required for high-risk patients before long-term methotrexate, not azathioprine.
Biologics and JAK Inhibitors — IBD
Biological therapies represent the most transformative pharmacological advance in IBD management over the past 25 years, providing the first treatments capable of inducing and maintaining true mucosal healing in moderate-to-severe IBD that is refractory to conventional immunomodulators. Before biologics, patients with severe Crohn's disease or steroid-dependent UC faced an inevitable progression toward surgery; infliximab and subsequent biologics changed that trajectory. However, their potent immunosuppressive mechanisms carry genuine and serious risks — most critically, reactivation of latent infections including tuberculosis and hepatitis B — that require mandatory pre-treatment screening that is non-negotiable and that you must know as a prescribing clinician. In India, where latent TB prevalence approaches 28% in adults, this screening requirement is not a theoretical protocol — it is an immediate clinical imperative every time you consider prescribing an anti-TNF biologic.
Biological therapies have fundamentally transformed IBD management over the past two decades, providing the first treatments capable of inducing and maintaining mucosal healing in moderate-to-severe IBD that is refractory to conventional immunomodulators. However, their potent immunosuppressive mechanisms carry genuine risks — most critically, reactivation of latent infections — that require mandatory pre-treatment screening. Understanding these screening requirements is as important as knowing the drug mechanisms.
Anti-TNF-α monoclonal antibodies:
- Infliximab (Remicade): Chimeric (25% murine, 75% human) IgG1 monoclonal antibody against TNF-α. Given by IV infusion (5 mg/kg at 0, 2, and 6 weeks for induction, then every 8 weeks for maintenance). Approved for moderate-severe UC and CD.
- Adalimumab (Humira): Fully human IgG1 anti-TNF-α antibody. Given SC (160 mg, then 80 mg, then 40 mg every 2 weeks). Advantage: self-injection, no infusion centre needed.
Mechanism: TNF-α is a central pro-inflammatory cytokine in IBD. Anti-TNF antibodies neutralise soluble TNF-α and bind membrane-bound TNF-α, inducing apoptosis of activated T-cells and macrophages expressing membrane TNF-α.
Pre-treatment screening (mandatory):
- Latent tuberculosis: IGRA (interferon-gamma release assay, preferred) or tuberculin skin test + chest X-ray. If positive: treat with isoniazid for 9 months BEFORE starting anti-TNF (or at least 4–8 weeks before). Reactivation of latent TB is the most serious infection risk — presenting as disseminated or extrapulmonary TB.
- Viral hepatitis: Screen for hepatitis B (HBsAg, anti-HBc) — anti-TNF can reactivate HBV, sometimes fatally; treat with entecavir/tenofovir prophylactically if HBsAg+ or anti-HBc+. Screen for hepatitis C.
- Varicella (VZV): Ensure vaccination before starting if seronegative (live vaccines are contraindicated on biologic therapy).
ADRs: Infusion reactions (infliximab — pre-medicate with antihistamine/hydrocortisone if history), injection site reactions (adalimumab), opportunistic infections (reactivated TB, fungal infections — histoplasmosis, Pneumocystis), demyelinating disease (rare — avoid in MS), worsening heart failure (avoid in NYHA class III/IV), formation of anti-drug antibodies (particularly with infliximab — co-prescribe with low-dose azathioprine to reduce immunogenicity).
Vedolizumab: A humanised anti-α4β7 integrin monoclonal antibody. α4β7 is a gut-selective adhesion molecule expressed on gut-homing lymphocytes that mediates their trafficking into the intestinal mucosa. Blocking α4β7 prevents lymphocyte migration into the gut wall, reducing intestinal inflammation. Crucially, because α4β7 is gut-selective, vedolizumab does not significantly affect lymphocyte trafficking to other organs → lower systemic immunosuppression, fewer opportunistic infections than anti-TNF. It is approved for moderate-severe UC and CD. TB and hepatitis screening is still required, but the systemic infection risk profile is more favourable than anti-TNF.
Ustekinumab: A human anti-IL-12/IL-23 p40 subunit monoclonal antibody. IL-12 drives Th1 responses (IFN-γ, TNF); IL-23 drives Th17 responses (IL-17, IL-22) — both central to IBD pathogenesis. Approved for moderate-severe CD and UC.
JAK inhibitors (tofacitinib, upadacitinib): Oral small molecules that inhibit Janus kinases (JAK1/2/3), blocking signal transduction from multiple cytokine receptors simultaneously (IL-6, IFN-γ, IL-4, IL-12, IL-23 and others all signal via JAK-STAT). Rapid onset compared to biologics. ADRs: increased infection risk (herpes zoster reactivation is common — vaccinate against zoster before starting), dyslipidaemia, possible increased cardiovascular risk (based on post-marketing data with tofacitinib in rheumatoid arthritis — more caution in IBD context).
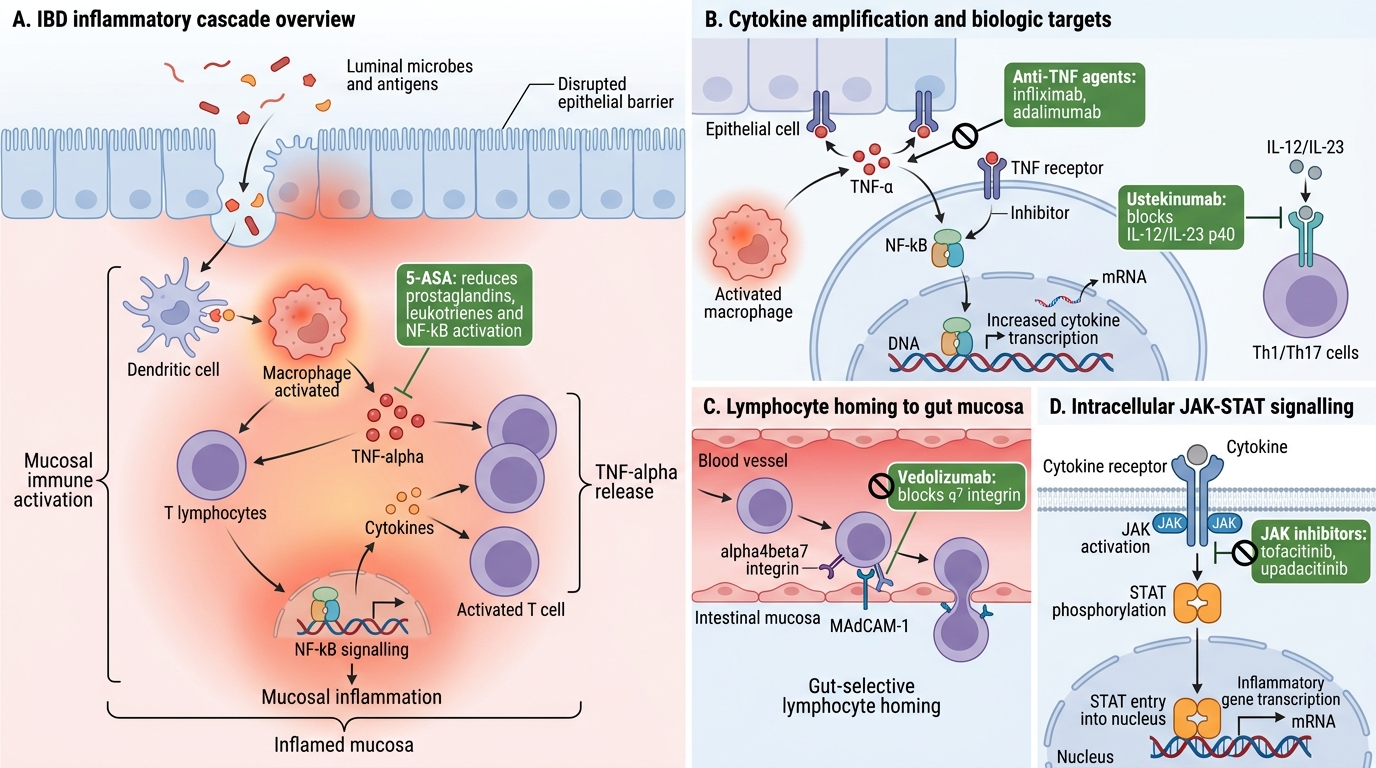
IBD Inflammatory Cascade and Drug Targets