Page 1 of 25
PH1.1-3 | PH1.1-3 | Core Pharmacology Terms and Therapeutic Reasoning — SDL Guide — SDL Guide
Learning Objectives
- Define pharmacology and its major sub-disciplines: pharmacokinetics, pharmacodynamics, pharmacognosy, pharmacotherapeutics, and toxicology.
- Explain the WHO criteria for rational drug use and identify consequences of irrational prescribing.
- Distinguish generic, brand, and chemical drug names; explain Indian drug schedules (H, H1, X) and the rationale for generic prescribing.
- Describe the hierarchy of evidence in evidence-based medicine and apply it to therapeutic decision-making.
INSTRUCTIONS
Every prescription you write as a clinician is an act of applied pharmacology. Whether you are choosing between two antibiotics, explaining why you prefer a generic tablet over a branded capsule, or evaluating a drug company's trial data, you are drawing on the vocabulary and reasoning framework built in this module. Pharmacology is not memorising drug lists — it is a systematic way of thinking about how drugs interact with the body and how best to use that interaction for patient benefit. This SDL lays that conceptual foundation.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 1 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 1 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old software engineer walks into your outpatient clinic with a sore throat. His father — also a physician — has already WhatsApp'd him a prescription for a combination antibiotic plus a vitamin C supplement 'for immunity.' You know from the swab that this is almost certainly viral pharyngitis. You reach for your prescription pad, then pause: Is this drug necessary? Is this dose evidence-based? Is the combination rational? Has the cost been considered? What you are about to decide in the next 60 seconds is pharmacotherapy — and every element of that decision has a name, a principle, and a body of evidence behind it. This module gives you that language.
WHY THIS MATTERS
Irrational drug use kills. The World Health Organization estimates that more than half of all medicines globally are prescribed, dispensed, or sold inappropriately. In India, antibiotic overuse has contributed directly to the emergence of multidrug-resistant organisms that now render previously curable infections untreatable. Understanding what pharmacology is, how drug names work, and what makes prescribing 'rational' is not an academic exercise — it is a professional obligation. The MCI/NMC mandates that every Indian graduate be able to prescribe rationally, report adverse drug reactions, and communicate drug information to patients. This SDL opens that clinical literacy.
RECALL
From your Year-1 biochemistry and physiology modules, you already know that biological systems respond to chemical signals through specific receptor proteins, that the liver harbours cytochrome P450 (CYP450) enzymes that transform xenobiotics, and that the kidney filters plasma and excretes water-soluble compounds. These three ideas — receptor binding, hepatic transformation, renal elimination — are the molecular underpinnings of virtually everything you will study in pharmacology. Keep them in mind as we now build the conceptual map of the discipline.
What Pharmacology Studies and Why It Matters Clinically
Pharmacology is the science of drugs — how they are derived, what they do to living systems, and what living systems do to them. The word comes from the Greek pharmakon (drug or poison) and logos (study), reflecting the ancient recognition that the same substance can heal or harm depending on dose, route, and context. For a Year-2 medical student, pharmacology is the bridge between the basic sciences of Year 1 and the clinical reasoning of Years 3–5.
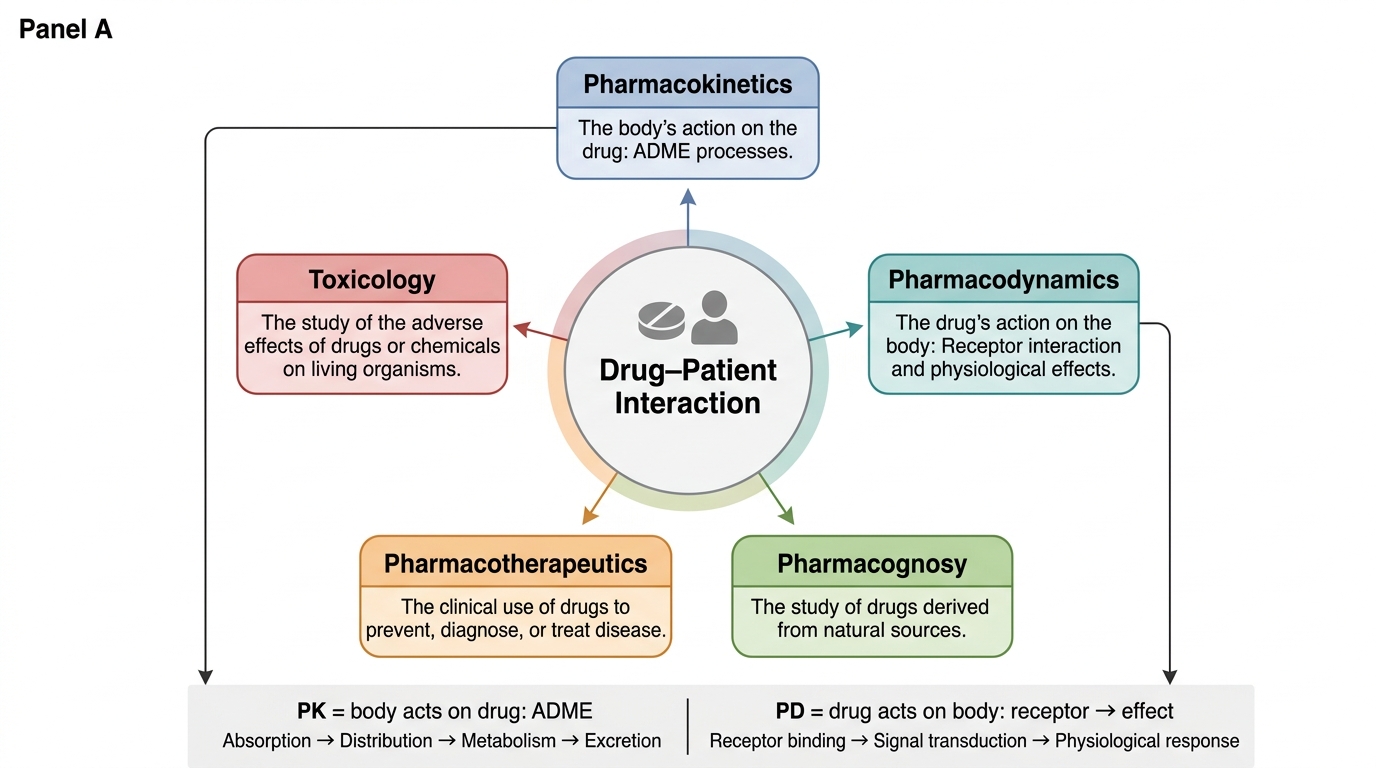
The discipline is structured into several inter-related sub-disciplines, each asking a distinct question about the drug–patient interaction:
- Pharmacokinetics (PK): What does the body do to the drug? This encompasses absorption, distribution, metabolism, and excretion (ADME) — the journey of a drug from the time it enters the body to the time it leaves.
- Pharmacodynamics (PD): What does the drug do to the body? This covers mechanism of action, receptor interactions, dose–response relationships, and the spectrum from therapeutic to toxic effects.
- Pharmacognosy: The study of drugs derived from natural sources — plants, fungi, marine organisms, and minerals. Digitalis from foxglove and morphine from the opium poppy are canonical examples.
- Pharmacotherapeutics: The clinical application of drugs to treat, prevent, or diagnose disease. It integrates PK and PD to answer: which drug, for which patient, at which dose?
- Toxicology: The study of adverse or poisonous effects of chemicals on living systems. Paracelsus' 16th-century principle applies here: "All things are poison, and nothing is without poison; only the dose makes a thing not a poison."
- Pharmacovigilance: The ongoing surveillance of drug safety after market approval — the discipline that detects rare ADRs that clinical trials, with their finite populations, cannot.
Understanding these sub-disciplines prevents a common student mistake: treating pharmacology as a synonym for 'drug lists.' Clinical pharmacology demands reasoning, not recitation.
Major Sub-disciplines of Pharmacology
SELF-CHECK
A textbook defines 'pharmacodynamics' as 'what the drug does to the body.' A student argues this means pharmacodynamics includes ADME — because changes in plasma concentration alter what the drug 'does.' Which response best addresses this confusion?
A. The student is correct: pharmacodynamics encompasses all drug effects including ADME.
B. ADME describes what the body does to the drug (pharmacokinetics); pharmacodynamics specifically studies drug-receptor interactions and resulting effects.
C. Pharmacodynamics only applies to agonist drugs; antagonist effects are studied under pharmacokinetics.
D. The distinction is only historical; modern pharmacology treats PK and PD as a single discipline.
Reveal Answer
Answer: B. ADME describes what the body does to the drug (pharmacokinetics); pharmacodynamics specifically studies drug-receptor interactions and resulting effects.
Pharmacokinetics and pharmacodynamics are complementary but distinct. PK = body acts on drug (absorption, distribution, metabolism, excretion, hence ADME). PD = drug acts on body (receptor binding, signal transduction, physiological effect). The confusion is common because PK parameters (e.g., Cmax, AUC) influence the magnitude of PD responses — but that interdependence doesn't erase the conceptual distinction.
Goals of Drug Therapy and Rational Drug Use
Every drug is prescribed with a therapeutic intention — to cure, to relieve symptoms, to prevent disease, or to diagnose a condition. Rational drug use is the framework that ensures that intention is realised safely and cost-effectively for the patient and society. The World Health Organization (1985) defined rational drug use as: "patients receive medications appropriate to their clinical needs, in doses that meet their own individual requirements, for an adequate period of time, and at the lowest cost to them and their community."
This definition sounds simple, but its implications are profound. Consider what happens when a prescription violates it: a drug prescribed without an appropriate indication exposes the patient to risk with no prospect of benefit; an incorrect dose leads to either therapeutic failure or toxicity; an unnecessarily prolonged course of antibiotics selects for resistant organisms. The WHO definition was drafted in 1985 precisely because irrational prescribing had become a global public health crisis, and it remains the internationally accepted standard against which every prescribing decision can be measured. Embedding this framework in your clinical reasoning from Year 2 means you graduate with the habits that prevent the commonest and costliest prescribing errors.
In practice, the WHO criteria distil rational prescribing into six verifiable conditions:
1. Right drug — selected from evidence-based guidelines, not habit, promotion, or patient pressure.
2. Right indication — the drug is actually needed for a confirmed diagnosis.
3. Right dose — titrated to the patient's weight, age, renal and hepatic function.
4. Right route — the most appropriate route for the indication and the patient's ability to take it.
5. Right duration — sufficient to achieve the therapeutic goal, not so long as to risk toxicity or resistance.
6. Right information — the patient understands the purpose, dose schedule, expected effects, and when to return.
The consequences of irrational drug use are not merely academic. Antibiotic over-prescription drives antimicrobial resistance. Polypharmacy in elderly patients multiplies drug interaction risk. Unnecessary injectable drugs raise costs and infection risk. Prescription without diagnosis — as in the opening clinical hook — deprives the patient of accurate information and exposes them to avoidable harm.
The WHO Model List of Essential Medicines operationalises rational use at the policy level: it is the minimum list of medicines that satisfy the priority health care needs of a population, selected with regard to disease prevalence, evidence of efficacy and safety, and comparative cost-effectiveness. Prescribing from the essential medicines list is a globally endorsed marker of rational practice.
Drug Nomenclature: Generic, Brand, and Scheduled Drugs
Every drug in clinical use carries multiple names, and the choice of which name to use on a prescription has legal, economic, and safety implications that every prescriber must understand.
The chemical name describes the molecular structure of the compound (e.g., (RS)-2-(4-(2-methylpropyl)phenyl)propanoic acid). It is precise but unwieldy and appears mainly in research contexts.
The generic name (international non-proprietary name, INN) is the globally standardised, non-proprietary name assigned by the World Health Organization. Examples: ibuprofen, paracetamol, metformin. The INN is the name on the WHO Model List, the name in standard references such as the British National Formulary and Tripathi, and — since MCI notifications in 2016, reiterated by NMC — the name every Indian prescriber is expected to use on prescriptions. Generic prescribing enables pharmacists to dispense any bioequivalent formulation, expanding patient access and reducing cost.
The brand name (proprietary name) is a trademarked commercial name given by a pharmaceutical manufacturer (e.g., Brufen, Crocin, Glucophage). Brand names are written with a capital letter. The same generic drug may have dozens of brand names from different manufacturers. There is no pharmacological difference between bioequivalent formulations of the same generic, but brand names generate price premiums that can be substantial.
Cost-effectiveness is the practical argument for generic prescribing: ibuprofen tablets cost a fraction of the same dose under a brand name, and for patients in resource-limited settings, that difference determines adherence.
In India, drugs are regulated under the Drugs and Cosmetics Act (1940) and its schedules:
| Schedule | Description | Prescription requirement | Examples |
|---|---|---|---|
| Schedule H | Prescription-only medicines | Prescription required; retained by pharmacist | Most antibiotics, antihypertensives, antidiabetics |
| Schedule H1 | Third-generation cephalosporins, fluoroquinolones, combination antibiotics — subject to enhanced monitoring | Prescription required; pharmacist records details in register; retained | Cefixime, ciprofloxacin, fixed-dose combination antibiotics |
| Schedule X | Narcotic and psychotropic substances | Special form prescription (triplicate); strictly regulated | Morphine, codeine, diazepam, barbiturates |
Schedule H1 was added specifically to combat antibiotic resistance: pharmacists must maintain a register of Schedule H1 dispensing. This directly connects drug nomenclature and scheduling to the rational use principle.
SELF-CHECK
A patient asks you why you wrote 'metformin 500 mg' on their prescription instead of 'Glucophage 500 mg.' Your best answer reflects which principle?
A. Brand-name drugs are less safe and should always be avoided.
B. Generic prescribing enables dispensing of any bioequivalent formulation, improving access and reducing cost while maintaining the same therapeutic effect.
C. The NMC prohibits brand-name prescriptions entirely for all drug classes.
D. Generic drugs are manufactured to lower quality standards than branded drugs.
Reveal Answer
Answer: B. Generic prescribing enables dispensing of any bioequivalent formulation, improving access and reducing cost while maintaining the same therapeutic effect.
Bioequivalent generic formulations contain the same active ingredient, dose, route, and release mechanism as the brand-name product and must meet the same regulatory standards. Generic prescribing is preferred because it widens access, reduces cost, and is mandated by the NMC for Indian prescribers. The claim that generics have lower quality is a common misconception — regulatory bioequivalence requirements are the same.