Page 2 of 25
PH1.1-3 | PH1.1-3 | Core Pharmacology Terms and Therapeutic Reasoning — SDL Guide — SDL Guide (Part 2)
Evidence-Based Medicine and Its Hierarchy of Evidence
Evidence-based medicine (EBM) integrates the best available research evidence with clinical expertise and patient values to inform therapeutic decisions. The term was formalised by Sackett and colleagues at McMaster University in the 1990s, but the underlying principle — that clinical decisions should be grounded in empirically validated data rather than tradition, anecdote, or pharmaceutical promotion — is as old as clinical epidemiology. Before EBM became formalised, prescribing practices were shaped largely by senior physician habits, pharmaceutical detailing, and individual case experience — all of which are vulnerable to systematic biases. EBM provides a structured antidote: it asks what is the quality and quantity of evidence supporting this choice? and demands that the answer be grounded in publicly reported, reproducible research rather than personal authority.
Not all research is equally trustworthy, however. A single case report may suggest a drug benefit that a large RCT later refutes. The hierarchy of evidence (often depicted as a pyramid) ranks study designs by their susceptibility to bias and confounding, allowing prescribers to assign appropriate weight to different information sources when making decisions:
- Expert opinion and case reports (base): lowest confidence; subject to recall bias, selection bias, and authority bias. Useful for hypothesis generation, not treatment decisions.
- Case-control and cohort studies (observational): useful for rare outcomes and long time horizons but vulnerable to confounding. Cohort studies (prospective) rank higher than case-control (retrospective).
- Randomised controlled trials (RCTs): the gold standard for establishing causality. Random allocation eliminates selection bias; blinding reduces ascertainment bias. A well-designed RCT provides the strongest evidence for drug efficacy.
- Systematic reviews and meta-analyses (apex): synthesise multiple RCTs, increasing statistical power and generalisability. The Cochrane Collaboration is the canonical source.
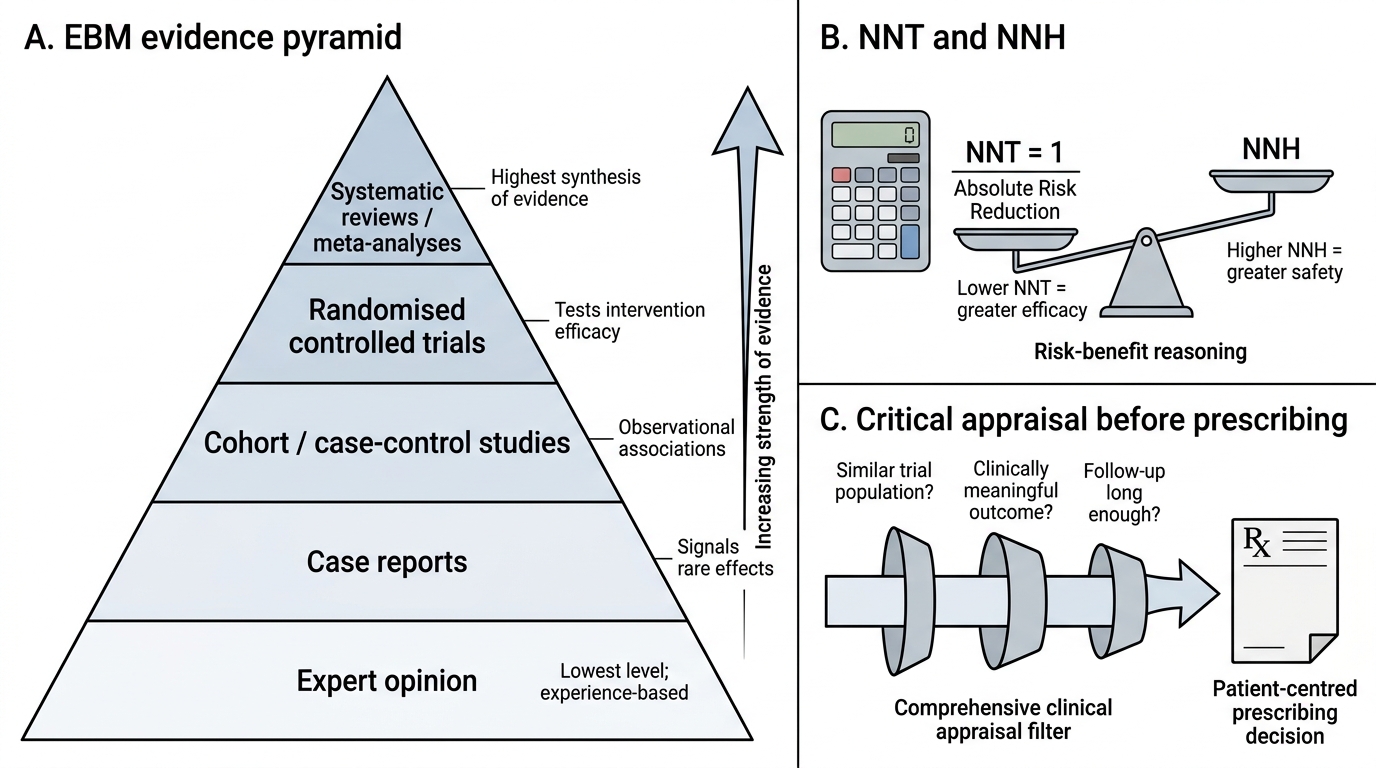
Evidence-Based Medicine Pyramid for Prescribers
Two quantitative tools from EBM are essential for prescribers:
- Number Needed to Treat (NNT): the number of patients who must be treated to prevent one additional bad outcome. A lower NNT indicates greater efficacy. NNT = 1 / (Absolute Risk Reduction).
- Number Needed to Harm (NNH): the number of patients who must be treated before one additional harm event occurs. A higher NNH indicates greater safety. The NNT-to-NNH ratio informs risk-benefit reasoning.
EBM is not the same as 'always following the largest trial.' It requires critical appraisal: Was the trial population similar to your patient? Was the outcome clinically meaningful or merely a surrogate marker? Was the follow-up long enough? The physician who prescribes from an RCT whose population excludes elderly patients is misapplying the evidence, not practising EBM.
Applying Therapeutic Reasoning in Practice
Therapeutic reasoning is the clinical skill of synthesising pharmacological knowledge to reach a prescribing decision that is simultaneously effective, safe, rational, and patient-centred. It is not a checklist — it is a habit of thought that improves with practice. This section uses the opening case to demonstrate how the terms and principles introduced in this module integrate in real clinical time.
Return to the 28-year-old with viral pharyngitis and the WhatsApp prescription for a combination antibiotic plus vitamin C:
Step 1 — Define the indication. The swab strongly suggests viral aetiology. Antibiotics act on bacteria, not viruses. The right indication criterion of rational drug use is not met. Prescribing an antibiotic here is irrational prescribing regardless of how 'safe' the antibiotic is.
Step 2 — Consult the evidence. What does the systematic review literature say about antibiotic use in uncomplicated viral pharyngitis? Cochrane reviews consistently show no benefit in symptom duration vs placebo, while documenting risks (GI side effects, candidiasis, disruption of microbiome, contribution to resistance). NNT for antibiotic use in viral pharyngitis approaches infinity (no benefit), while NNH is finite. The evidence hierarchy argues against.
Step 3 — Apply drug nomenclature and cost-effectiveness. If a symptomatic treatment such as paracetamol (generic name) is appropriate, it should be prescribed by its generic name. The brand-name equivalent costs 3–5 times more for identical efficacy. The Schedule H designation of the combination antibiotic means it requires a prescription — reinforcing that it should not have been self-recommended.
Step 4 — Communicate the decision. Rational drug use includes giving the patient the right information. Explaining why you are not prescribing the antibiotic — using accessible language, addressing the father's recommendation respectfully — is itself a therapeutic act that preserves the patient's trust and adherence to future evidence-based treatment.
This four-step reasoning loop maps onto the pharmacology sub-disciplines: PD (does this drug affect the causative agent?), EBM (what does the evidence show?), nomenclature and scheduling (what is the correct name and legal status?), and rational use (does this meet WHO criteria?). These are not separate subjects — they are one integrated clinical skill.
CLINICAL PEARL
The 'brand-name halo' trap: Studies consistently show that physicians and patients perceive brand-name drugs as superior to generics, even when bioequivalence has been demonstrated. This perception is reinforced by pharmaceutical marketing and has no pharmacological basis. Regulators (US FDA, India CDSCO) require generic manufacturers to demonstrate that their product produces the same Cmax and AUC within 80–125% of the reference brand (the standard bioequivalence acceptance criterion) under controlled conditions — a strict standard that ensures therapeutic equivalence. When a patient insists on a brand-name drug, explain bioequivalence, the cost differential, and the WHO rational use framework. Prescribing a more expensive brand because of perceived (not demonstrated) superiority is itself a form of irrational drug use.
SELF-CHECK
In a meta-analysis of 12 RCTs, the drug showed an absolute risk reduction (ARR) of 2% for the primary endpoint. The NNT is therefore:
A. 2
B. 12
C. 50
D. 200
Reveal Answer
Answer: C. 50
NNT = 1 / ARR = 1 / 0.02 = 50. This means 50 patients must be treated for one additional patient to benefit. Whether NNT = 50 is 'good' or 'poor' depends on the severity of the outcome (a NNT of 50 for preventing fatal MI is excellent; for preventing a headache it is poor) and should always be weighed against the NNH.