Page 4 of 25
PH1.4-5 | PH1.4-5 | Drug Formulations, Delivery Systems and Administration Routes — SDL Guide — SDL Guide
Learning Objectives
- Identify common drug formulations (tablets, capsules, solutions, suspensions, inhalers, patches) and explain their advantages and disadvantages.
- Describe the major routes of drug administration and compare their onset of action, bioavailability, and clinical suitability.
- Explain the concept of first-pass hepatic metabolism and identify which routes bypass it.
- Demonstrate correct technique for sublingual, inhaler (MDI/DPI), and injection (SC, IM, IV) administration.
INSTRUCTIONS
A drug in the wrong formulation or delivered by the wrong route can be completely ineffective — or dangerously toxic. Nitroglycerin swallowed as an oral tablet is destroyed by first-pass metabolism before it ever reaches the coronary arteries; given sublingually, it relieves angina within two minutes. Insulin given orally is digested as a protein; given subcutaneously, it controls blood glucose for hours. The choice of formulation and route is not a logistical afterthought — it is a core pharmacological decision that directly determines whether a prescribed drug will work. This SDL gives you the conceptual framework and practical vocabulary to make that decision deliberately.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 1-2 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 2 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 65-year-old man with ischaemic heart disease arrives at the emergency department clutching his chest. His daughter hands you a bottle of isosorbide dinitrate tablets he has been swallowing whole. You know nitrates work — but not when taken orally at full dose. The sublingual form of the same compound, placed under the tongue, would have acted within two minutes. Instead, he is in the ED with ongoing ischaemia. One route. One formulation difference. Two completely different clinical outcomes. How did this happen, and how do you prevent it from happening to your patients?
WHY THIS MATTERS
Prescribing a drug is a two-part decision: what molecule to use, and how to deliver it. A drug that cannot reach its target site at an adequate concentration will not work, regardless of its pharmacodynamic potency. Drug formulation and route of administration determine the speed of onset, peak plasma concentration, duration of action, and whether the drug survives the gastrointestinal tract and hepatic first-pass metabolism. For the practicing clinician, this knowledge translates directly into the ability to select the right formulation for a patient who cannot swallow tablets, to counsel a patient on inhaler technique, and to recognise when parenteral administration is necessary for life-threatening emergencies.
RECALL
From Year-1 physiology, you know that the gastrointestinal tract absorbs nutrients through epithelial cells via passive diffusion, active transport, and carrier-mediated mechanisms. The portal venous system drains the gut and carries absorbed substances directly to the liver before they enter the systemic circulation — the anatomical basis of first-pass metabolism. From biochemistry, recall that the liver contains CYP450 enzymes that oxidise, reduce, and conjugate lipophilic xenobiotics to make them water-soluble for renal excretion. These two concepts — GI epithelial absorption and hepatic first-pass transformation — determine why some drugs must be given parenterally and why formulation engineers work so hard to protect drugs from the GI environment.
Why Formulation and Route Shape Drug Therapy
Drug formulation refers to the physical and chemical form in which an active pharmaceutical ingredient (API) is presented for administration — whether as a tablet, solution, inhaled aerosol, or transdermal patch. Route of administration refers to the pathway by which that formulation is introduced into or onto the body. These two factors jointly determine three critical pharmacokinetic parameters: the rate at which the drug reaches its target tissue, the peak concentration it achieves there, and the duration of its action.
The clinical relevance of these choices is not theoretical. Consider four presentations of the same drug, morphine: given intravenously it acts within seconds to minutes, making it the route of choice for acute post-operative pain or trauma; given intramuscularly it acts in 15–30 minutes; given orally as an immediate-release tablet it acts in 30–60 minutes; given as a sustained-release oral formulation it provides pain control for 8–12 hours with a smooth plasma concentration curve, avoiding the peaks of euphoria and troughs of breakthrough pain associated with repeated short-acting doses. The choice among these options is not a matter of convenience alone — it requires integrating the patient's clinical condition, the acuity of the symptom, whether the oral route is accessible, and the pharmacokinetic properties of the formulation.
Understanding formulation and route also protects against a class of serious clinical errors: giving a sustained-release tablet crushed through a nasogastric tube delivers the entire 24-hour dose in minutes, potentially causing fatal toxicity. Giving an enteric-coated tablet with a high-fat meal that delays gastric emptying can delay the drug's absorption unpredictably. These are not exotic edge cases — they are everyday ward hazards that pharmacological literacy prevents.
Therapeutic Goals of Drug Delivery Systems
A drug delivery system is designed to achieve four overarching therapeutic goals, each of which motivates a distinct class of formulation strategies. Grasping these goals transforms the memorisation of formulation names into a coherent engineering logic.
The first goal is reliable delivery to the target tissue at a therapeutic concentration. This requires that the drug survive the route of delivery (acid in the stomach, enzymes in the gut lumen, first-pass metabolism in the liver), be absorbed in adequate quantity, and distribute to the correct compartment. Enteric coatings, prodrug strategies, and parenteral formulations all serve this goal.
The second goal is controlled release — delivering drug at a rate that maintains plasma concentrations within the therapeutic window (above minimum effective concentration, below toxic threshold) for as long as clinically needed. Sustained-release (SR), extended-release (XR), and controlled-release (CR) formulations achieve this by embedding the API in polymer matrices, using osmotic pumps, or layering drug with release-controlling membranes. The clinical benefit is reduced dosing frequency, smoother plasma levels, and fewer peak-related side effects.
The third goal is minimising first-pass hepatic metabolism for drugs with high first-pass extraction. When absorbed from the gut, drugs travel via the portal vein to the liver before reaching the systemic circulation; a drug with 90% first-pass extraction reaches systemic circulation at only 10% of the absorbed dose. Sublingual, buccal, transdermal, rectal (upper rectum drains into the portal system, but lower rectum drains into the systemic circulation directly), inhaled, and intravenous routes all bypass part or all of hepatic first-pass metabolism, thereby increasing bioavailability — defined as the fraction of the administered dose that reaches the systemic circulation in active form.
The fourth goal is patient convenience and adherence. Once-daily formulations, oral liquid preparations for patients who cannot swallow tablets, and pre-filled auto-injectors for self-administration all exist to remove barriers to adherence — because the most pharmacologically perfect drug is ineffective if the patient does not take it.
Common Drug Formulations: Types and Their Advantages and Disadvantages
Drug formulations span a wide range of physical forms, each with distinct properties suited to particular routes, patient populations, and therapeutic requirements. Understanding their advantages and disadvantages is essential for both prescribing and counselling patients.
Solid formulations are the most commonly prescribed oral dosage forms. Plain tablets are compressed powders of API plus excipients; they are stable, precise in dose, and convenient, but must be swallowed whole and are unsuitable for patients with dysphagia. Enteric-coated tablets are covered with an acid-resistant polymer (e.g., cellulose acetate phthalate) that prevents dissolution in the acidic stomach (pH 1–3) and releases drug in the alkaline duodenum (pH 5–7); used for acid-labile drugs (omeprazole, enteric-coated aspirin) and drugs that irritate the gastric mucosa. Sustained-release (SR/XR/CR) tablets embed the API in a polymer matrix or use osmotic technology to release drug gradually over 8–24 hours; advantages include reduced dosing frequency and smoother plasma levels, but crushing destroys the controlled-release mechanism and is potentially dangerous. Capsules (hard gelatin for powders/granules, soft gelatin for oils/liquids) are easier to swallow than tablets for some patients and mask unpleasant tastes.
Liquid formulations include solutions, suspensions, syrups, and elixirs. They are suitable for paediatric patients and those with swallowing difficulties, allow flexible dosing, and have faster gastric emptying and faster onset than solid forms. Disadvantages include shorter shelf life, measurement imprecision, and the need for accurate dosing devices. Suspensions require thorough shaking before use because the API settles; failure to shake gives an incorrect dose.
Semi-solid formulations — ointments, creams, gels, and pastes — are applied topically. Ointments have an oil base (greater occlusion, moisturising, better drug penetration), creams are oil-in-water emulsions (less greasy, cosmetically preferable), gels are aqueous polymers (fastest absorption, suitable for hairy areas). Their advantage is local action with minimal systemic absorption; limitation is variable penetration through intact versus broken skin.
Aerosol/inhaler formulations deliver drug directly to the bronchial tree. Metered-dose inhalers (MDI) use a propellant to deliver a fixed drug dose; require coordination between actuation and inhalation (a spacer device removes this requirement for children and elderly patients). Dry-powder inhalers (DPI) are propellant-free and breath-activated; require a minimum inspiratory flow rate. Nebulisers convert liquid drug into a fine mist for inhalation; used in acute severe asthma and COPD when the patient cannot coordinate MDI use.
Specialised delivery systems include transdermal patches (slow, continuous systemic delivery — useful for fentanyl, nitroglycerin, nicotine; avoids oral first-pass), implants (subdermal rods — contraceptive implants release etonogestrel over 3 years), depot injections (IM formulations of drug in oil or polymer microspheres providing sustained release over weeks to months — used for antipsychotics, contraceptives, hormonal therapy), and liposomal/nanoparticle formulations (encapsulate drug in lipid vesicles or nanocarriers to improve targeting, reduce toxicity — liposomal amphotericin B, nanoparticle paclitaxel).
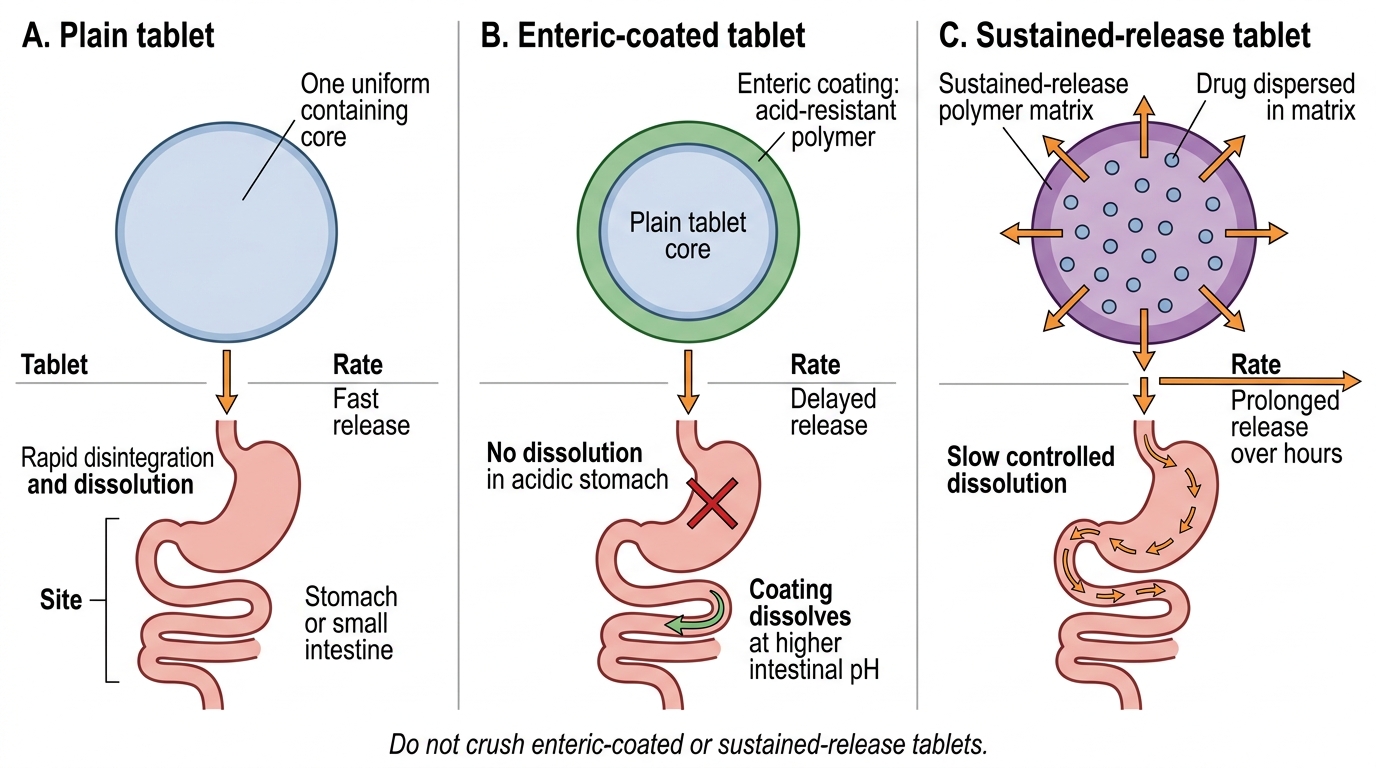
Tablet Formulations: Site and Rate of Dissolution
| Formulation type | Key examples | Main advantages | Main disadvantages |
|---|---|---|---|
| Plain tablet | Paracetamol, metformin | Stable, precise dose, convenient | Cannot crush SR; unsuitable for dysphagia |
| Enteric-coated | Omeprazole, EC aspirin | Protects acid-labile drugs; reduces gastric irritation | Cannot be crushed; delayed onset |
| Sustained-release | Metformin XR, diltiazem SR | Reduced dosing frequency; smoother plasma levels | MUST NOT crush; higher cost |
| Hard/soft gelatin capsule | Amoxicillin caps, fish oil | Easy to swallow; masks taste | Hygroscopic; soft gel may leak |
| Oral solution/syrup | Paracetamol syrup | Suitable for children, dysphagia; rapid onset | Short shelf life; measurement error risk |
| Suspension | Amoxicillin suspension | Flexible dosing; easy to swallow | Must shake well; short shelf life after reconstitution |
| Cream/ointment/gel | Clobetasol cream, mupirocin ointment | Local action; minimal systemic effects | Variable skin penetration |
| MDI inhaler | Salbutamol MDI | Rapid onset; portability | Requires actuation-inhalation coordination |
| DPI inhaler | Tiotropium DPI | No propellant; breath-activated | Requires adequate inspiratory flow |
| Transdermal patch | Fentanyl patch, GTN patch | Avoids first-pass; sustained release | Skin irritation; slow onset |
| Depot injection | Haloperidol decanoate | Weeks to months duration; improves adherence | Painful injection; cannot reverse rapidly |
| Liposomal | Liposomal amphotericin B | Reduced nephrotoxicity; targeted delivery | High cost |
SELF-CHECK
A patient with peptic ulcer disease is prescribed enteric-coated omeprazole. The ward nurse asks if she can crush the tablet and give it via nasogastric tube. Your response should be:
A. Yes — crushing makes administration easier and will not affect the drug.
B. No — crushing destroys the enteric coating, exposing the acid-labile drug to gastric acid and causing degradation before absorption.
C. Yes — but only if mixed with apple juice to protect it.
D. No — enteric-coated drugs should always be given intravenously via NG tube.
Reveal Answer
Answer: B. No — crushing destroys the enteric coating, exposing the acid-labile drug to gastric acid and causing degradation before absorption.
Enteric coatings consist of acid-resistant polymers that protect the drug from gastric acid. Crushing breaks this protection, exposing the API to gastric pH 1–3 where acid-labile drugs such as omeprazole are degraded. Omeprazole should either be given as granules (which can be dispersed without crushing) or switched to an IV formulation when the oral route is impractical. This is a common, high-stakes ward error.