Page 5 of 25
PH1.4-5 | PH1.4-5 | Drug Formulations, Delivery Systems and Administration Routes — SDL Guide — SDL Guide (Part 2)
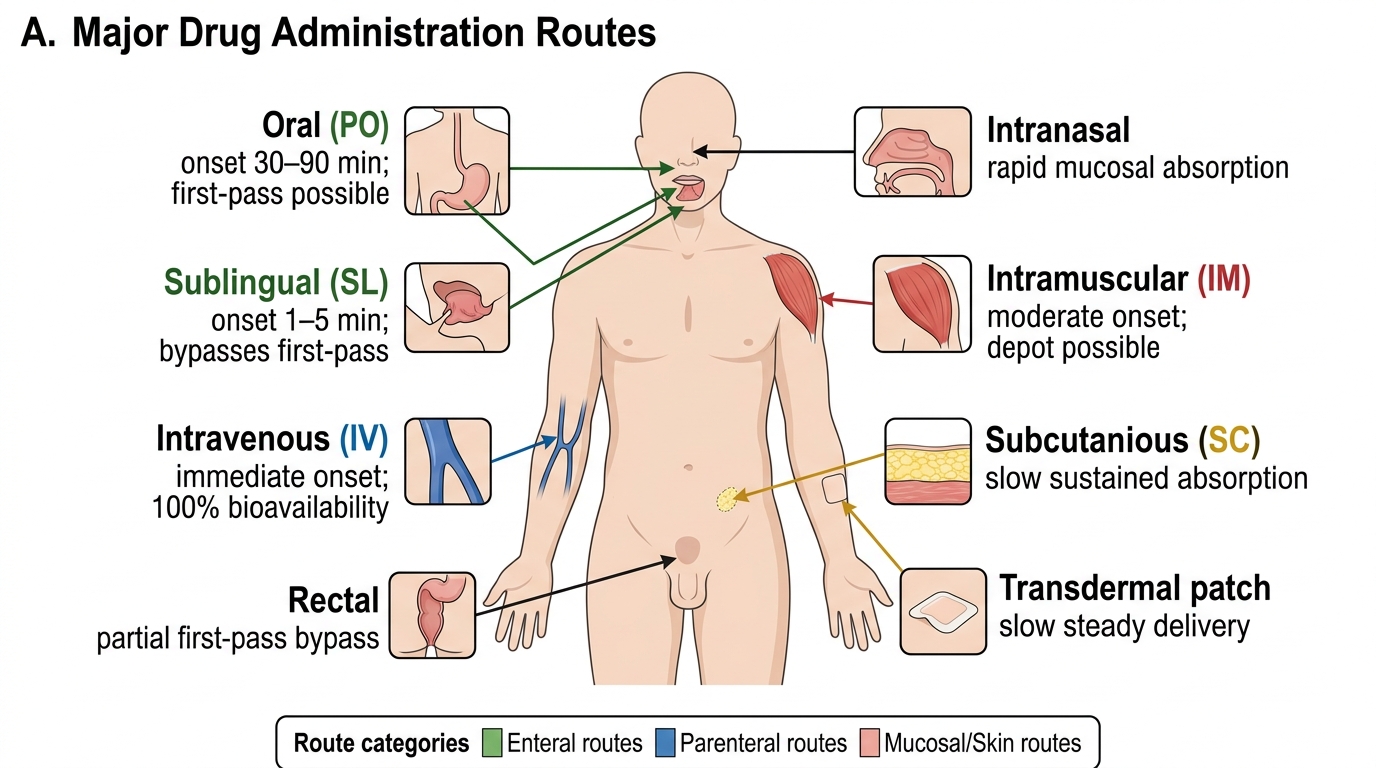
Routes of Drug Administration: Characteristics and Comparison
The route of drug administration determines the pathway a drug takes from the site of administration to the systemic circulation, and directly governs onset of action, peak plasma level, bioavailability, and clinical applicability. Routes are broadly classified as enteral (through the gastrointestinal tract), parenteral (bypassing the GI tract), and topical/local.
Enteral routes:
The oral (PO) route is the most common, most convenient, and safest route for non-emergency drugs. Absorption occurs primarily in the small intestine. Disadvantages include first-pass hepatic metabolism (which reduces bioavailability for high-extraction drugs), dependence on gastric pH and motility, and inability to use in unconscious or vomiting patients. Oral bioavailability ranges from near zero (insulin — destroyed as protein) to nearly 100% (metformin — absorbed via intestinal transporters).
The sublingual (SL) route places the drug under the tongue, where it dissolves and absorbs through the thin, highly vascular sublingual mucosa directly into the sublingual veins → internal jugular → superior vena cava → systemic circulation, completely bypassing first-pass metabolism. Onset is rapid (1–5 minutes for glyceryl trinitrate / GTN). Only suitable for small doses of lipid-soluble drugs. Buccal administration (between cheek and gum) uses a similar mechanism.
The rectal route is used when the oral route is unavailable (vomiting, unconsciousness, paediatric). Upper rectal veins drain via the superior rectal vein into the portal system (partial first-pass effect); lower rectal veins drain into the middle and inferior rectal veins, bypassing the portal circulation. Bioavailability is therefore intermediate and variable. Examples: diazepam suppositories for febrile seizures, paracetamol suppositories.
Parenteral routes:
The intravenous (IV) route provides 100% bioavailability (no absorption step; drug enters systemic circulation directly), the fastest onset (seconds to minutes), and the ability to administer large volumes precisely. It is the route of choice for emergencies, drugs not absorbed orally, and titrated infusions. Disadvantages: requires trained personnel; risk of infection, air embolism, thrombophlebitis; cannot be reversed once injected.
The intramuscular (IM) route uses the highly vascular muscle tissue (deltoid, gluteal, vastus lateralis) for absorption by diffusion and lymphatic uptake. Onset is 10–30 minutes for aqueous solutions; depot formulations in oil can provide drug release for weeks. Suitable for vaccines, antibiotics, and antipsychotic depot preparations. Disadvantages: painful; haematoma risk in anticoagulated patients; absorption variable with reduced muscle blood flow.
The subcutaneous (SC) route injects into the loose connective tissue beneath the skin. Absorption is slower than IM due to lower vascularity; suitable for insulin (variable dose, frequent administration), low-molecular-weight heparin, vaccines, and self-administered biologics. The rate of absorption can be modified: hyaluronidase accelerates; adrenaline (added with local anaesthetics) delays by causing vasoconstriction.
The intradermal (ID) route injects into the dermis itself; used exclusively for tuberculin (Mantoux) testing and some vaccines. Very small volumes (0.1 mL); absorption is slow and limited — the advantage is that the local reaction (wheal) itself is the clinical endpoint.
The intrathecal (spinal) route injects drug into the subarachnoid space, bypassing the blood-brain barrier to achieve high CSF concentrations. Used for spinal anaesthesia (bupivacaine, lignocaine), intrathecal chemotherapy (methotrexate), and intrathecal antibiotics for meningitis in specific circumstances. High risk — requires strict aseptic technique and expertise.
Topical and inhalation routes are designed for local effect, though systemic absorption can occur. Inhaled drugs (salbutamol, corticosteroids) reach the airways directly with high local concentration and minimal systemic dose. Transdermal patches (GTN, fentanyl, oestrogen) achieve slow systemic absorption through skin bypassing first-pass metabolism.
Major Routes of Drug Administration
| Route | Onset | Bioavailability vs IV | First-pass effect | Clinical uses | Key disadvantages |
|---|---|---|---|---|---|
| Oral (PO) | 30–90 min | Variable (0–100%) | Yes (for many drugs) | Most chronic therapies | Cannot use in unconscious/vomiting |
| Sublingual (SL) | 1–5 min | High (bypasses liver) | No | GTN, buprenorphine | Small dose only; drug must dissolve rapidly |
| Rectal | 15–30 min | Intermediate/variable | Partial (lower rectum bypasses) | Antiemetics, anticonvulsants, paediatrics | Socially inconvenient; variable absorption |
| Intravenous (IV) | Seconds–minutes | 100% (definition) | No | Emergencies, infusions, chemotherapy | Trained personnel; infection; irreversible |
| Intramuscular (IM) | 10–30 min | 75–100% | No | Vaccines, antibiotics, depot antipsychotics | Painful; haematoma risk; variable in shock |
| Subcutaneous (SC) | 15–45 min | Variable | No | Insulin, LMWH, vaccines | Slower than IM; lipodystrophy with insulin |
| Intradermal (ID) | Slow (local) | Minimal | No | Mantoux test, BCG | Very small volume; technique-sensitive |
| Intrathecal | Minutes (CSF) | N/A (direct to CSF) | No | Spinal anaesthesia, IT chemotherapy | Highly technique-sensitive; severe errors possible |
| Transdermal | Hours | Variable (drug-dependent) | No | GTN, fentanyl, oestrogen | Slow onset; skin irritation |
| Inhaled | 1–5 min | High locally | Minimal systemic | Bronchodilators, inhaled steroids | Technique-dependent; systemic effects at high dose |
SELF-CHECK
Glyceryl trinitrate (GTN) is ineffective when swallowed as an oral tablet due to extensive first-pass hepatic metabolism. Which route of administration is used in acute angina specifically BECAUSE it bypasses first-pass metabolism?
A. Intramuscular injection — rapid onset from muscle vasculature
B. Sublingual — absorbed via sublingual mucosa directly into systemic circulation
C. Oral sustained-release — larger dose compensates for first-pass effect
D. Transdermal patch — immediate-onset via skin penetration
Reveal Answer
Answer: B. Sublingual — absorbed via sublingual mucosa directly into systemic circulation
The sublingual route delivers drug via the sublingual veins directly to the superior vena cava, bypassing the portal circulation entirely. GTN's first-pass extraction is ~90%, meaning only ~10% of an oral dose reaches systemic circulation. Sublingual GTN achieves near-complete systemic bioavailability and acts within 1–3 minutes — essential for acute angina relief. Transdermal GTN is used for angina prophylaxis (slow onset, hours) not acute attacks.
Demonstrating Administration: Inhalers, Injections, and Specialised Routes
Knowing which route to choose is necessary but not sufficient — the correct technique of drug administration is itself a clinical competency, and errors in technique lead to therapeutic failure as surely as prescribing the wrong drug. This section summarises the practical steps for the routes most commonly demonstrated and examined in clinical skills sessions.
Metered-dose inhaler (MDI) technique: (1) Remove cap and shake vigorously. (2) Exhale slowly and completely. (3) Place mouthpiece between lips creating a tight seal. (4) Begin slow, steady inhalation; simultaneously press the canister once to release a puff. (5) Continue inhaling slowly and deeply for 3–5 seconds. (6) Hold breath for 10 seconds to allow particle deposition. (7) Exhale slowly. A spacer device (valved holding chamber) removes the need for precise actuation-inhalation coordination, reduces oropharyngeal deposition, and is mandatory for inhaled corticosteroids (to reduce oral candidiasis) and recommended for children and patients with poor coordination.
Dry-powder inhaler (DPI) technique: (1) Load dose per device instructions (pierce capsule or click mechanism). (2) Exhale away from device. (3) Seal lips around mouthpiece. (4) Inhale forcefully and rapidly — the drug is carried by the patient's inspiratory airflow (no propellant). (5) Hold breath 5–10 seconds. DPIs require a minimum inspiratory flow rate (~30–60 L/min depending on device); patients in acute severe bronchoconstriction may be unable to generate sufficient flow, making nebulisation the preferred fallback.
Subcutaneous injection: Clean skin with antiseptic swab. Pinch a fold of subcutaneous tissue (abdomen, outer thigh, upper arm). Insert needle at 45° (or 90° for longer needles with adequate fat tissue). Inject slowly. Do not aspirate (aspirating before SC injection is no longer recommended; it increases bruising without reducing intravascular injection risk). Remove needle, apply gentle pressure. Insulin injection sites should be rotated systematically to prevent lipohypertrophy, which impairs absorption.
Intramuscular injection: Select appropriate site — deltoid (vaccines, small volumes ≤2 mL), vastus lateralis (paediatric, larger volumes), ventrogluteal or dorsogluteal (large volumes, depot formulations). Use Z-track technique for large volumes and irritating drugs (draws skin laterally before injection to seal drug in muscle after needle removal). Insert needle at 90°, full length. Aspirate for 5–10 seconds (IM aspiration is still recommended to reduce risk of inadvertent IV injection into gluteal vessels). Inject slowly. Remove. For depot preparations, do not massage the injection site (massaging disperses the depot and destroys the sustained-release effect).
Sublingual administration: Instruct patient to place tablet or spray under the tongue and keep mouth closed without swallowing. The drug must dissolve and be absorbed before swallowing. Patients should be warned not to eat or drink while the tablet dissolves, as this washes the drug into the stomach where it undergoes first-pass metabolism.
Clinical decision-making for route selection integrates four questions: (1) Is the patient conscious and able to swallow? (2) Is speed of onset critical? (3) Does the drug have high first-pass extraction? (4) Is the dose or volume compatible with the available routes? A drug needed within minutes in an unconscious patient requires IV administration. A chronic once-daily medication for a cooperative outpatient defaults to oral. A drug destroyed by GI enzymes or first-pass metabolism requires parenteral or mucosal routes.
CLINICAL PEARL
The inhaler technique gap: Clinical studies consistently show that 70–80% of patients use their inhalers incorrectly, even after verbal instruction. The most common errors are failing to exhale before inhalation, stopping inhalation at actuation instead of continuing the breath, and not holding the breath afterward. Each error substantially reduces pulmonary drug deposition. The clinical consequence is that apparent 'inhaler failure' in poorly controlled asthma or COPD is often a technique failure. Before escalating therapy in a patient with suboptimal inhaler response, always directly observe the patient's technique — this single step frequently identifies the problem and avoids unnecessary dose escalation or drug changes.
SELF-CHECK
A 7-year-old child with mild persistent asthma is prescribed salbutamol MDI. The parents report she cannot coordinate the inhaler properly. The most appropriate management is:
A. Switch to a DPI, which does not require coordination.
B. Add a spacer device to the MDI — this removes the need for precise actuation-inhalation coordination and reduces oropharyngeal deposition.
C. Switch to oral salbutamol tablets for better adherence.
D. Increase the MDI dose and teach repeated inhalations.
Reveal Answer
Answer: B. Add a spacer device to the MDI — this removes the need for precise actuation-inhalation coordination and reduces oropharyngeal deposition.
A valved spacer device attached to the MDI holds the drug cloud and allows the child to inhale at her own pace, removing the need for simultaneous actuation and inhalation. Spacers also reduce oropharyngeal deposition (and the risk of oral candidiasis with inhaled corticosteroids). DPIs require a higher inspiratory flow rate that young children often cannot generate. Oral salbutamol has more systemic side effects than inhaled; dose escalation without addressing technique is irrational.