Page 1 of 33
PH9.1 | PH9.1 | Immunomodulators — SDL Guide — SDL Guide
Learning Objectives
- Classify immunomodulators into immunosuppressants and immunostimulants with representative examples
- Describe the pharmacokinetics and pharmacodynamics of major immunosuppressant classes (calcineurin inhibitors, antiproliferatives, mTOR inhibitors, biologics, JAK inhibitors)
- Identify the major therapeutic uses and adverse drug reactions of immunomodulators
- Apply clinical reasoning to select appropriate immunomodulatory therapy and monitor for toxicity
INSTRUCTIONS
Immunomodulators are among the most consequential drugs in modern medicine — they make organ transplantation possible, control life-threatening autoimmune diseases, and stimulate deficient immune responses. Understanding their mechanisms, benefits, and serious risks is essential for any clinician managing post-transplant patients, rheumatological conditions, or complex infections. This module builds directly on your knowledge of lymphocyte biology from Year 1 Physiology.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 62 (Immunosuppressants) (textbook)
- Goodman & Gilman. The Pharmacological Basis of Therapeutics, 13th ed., Ch. 35 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old woman with end-stage renal disease receives a cadaveric kidney transplant. She is started on tacrolimus, mycophenolate mofetil, and prednisolone. Two months later, she develops a productive cough, fever, and a chest radiograph showing bilateral infiltrates. Her tacrolimus trough level is 18 ng/mL. What is happening, and how should you balance the competing demands of preventing rejection and controlling infection? This dilemma — too much immunosuppression risks infection; too little risks rejection — defines the clinical challenge of immunomodulatory pharmacology.
WHY THIS MATTERS
Immunomodulators are relevant across virtually every specialty. Transplant physicians use calcineurin inhibitors daily. Rheumatologists prescribe methotrexate, azathioprine, and biologics for autoimmune conditions. Oncologists use checkpoint inhibitors that the immune system exploits to attack tumours. Haematologists administer colony-stimulating factors to rescue neutrophils after chemotherapy. Understanding the pharmacology of these agents — their mechanisms, toxicity profiles, and monitoring requirements — is central to Year-2 clinical pharmacology and will be revisited throughout your clinical training in internal medicine, surgery, and dermatology.
RECALL
From Year-1 Physiology, recall that T-cell activation proceeds through a well-defined pathway: antigen presentation to the T-cell receptor (TCR) triggers intracellular calcium signalling, activating the phosphatase calcineurin, which dephosphorylates the transcription factor NFAT (Nuclear Factor of Activated T-cells). NFAT enters the nucleus and drives transcription of interleukin-2 (IL-2) — the key T-cell growth factor. IL-2 then binds its receptor (IL-2R, also called CD25) and signals through the mTOR pathway to drive lymphocyte proliferation. This cascade is the molecular scaffold on which almost every immunosuppressant acts. Also recall: B-cells bear surface immunoglobulin and CD20; plasma cells secrete antibodies; natural killer (NK) cells kill without MHC restriction; interferons are antiviral cytokines produced by infected cells.
The Immune System: Why We Need to Modulate It
The immune system is exquisitely calibrated to distinguish self from non-self, but that calibration can fail in two opposite directions. In transplant rejection, the recipient's immune system correctly identifies donor tissue as foreign and mounts a destructive T-cell and antibody response that destroys the graft. Without pharmacological suppression, all solid organ transplants would be rejected within days to weeks. In autoimmune diseases — such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and inflammatory bowel disease — the immune system mistakenly attacks the host's own tissues, leading to chronic inflammation and organ damage.
Conversely, in states of immunodeficiency (primary immunodeficiencies, HIV, post-chemotherapy neutropenia, or chronic infection), the immune response is inadequate and needs to be enhanced to fight infection or malignancy. Immunomodulators are drugs that restore this balance — either dampening pathological overactivation (immunosuppressants) or boosting a deficient response (immunostimulants).
The therapeutic challenge is that the same immune cells that cause harm in rejection or autoimmunity also protect the patient from infection and cancer surveillance. Every immunosuppressant, by definition, increases infection risk and potentially malignancy risk — this fundamental trade-off drives all dosing, monitoring, and therapeutic decision-making.
Classification of Immunomodulators
Therapeutic Goals of Immunomodulation
The therapeutic goal of immunosuppression in organ transplantation is to prevent allograft rejection while preserving sufficient immunity to defend against infection. This is operationalised as a therapeutic window that is narrow for many agents: too low a drug level risks rejection; too high risks nephrotoxicity, opportunistic infection, or post-transplant lymphoproliferative disorder.
In autoimmune disease, the goal shifts subtly: reduce the pathological autoimmune response to achieve disease remission or low disease activity while minimising cumulative drug toxicity. Because autoimmune therapy may continue for years or decades, cumulative adverse effects (bone loss from corticosteroids, increased malignancy from antiproliferatives) become the dominant long-term concern.
For immunostimulants, the goal is to restore or amplify an appropriate immune response — for example, correcting post-chemotherapy neutropenia with G-CSF to prevent life-threatening bacterial infection, or activating antiviral immunity with interferons in hepatitis C or multiple sclerosis.
All immunomodulatory prescribing therefore involves continuous reassessment: What is the current level of immune activity? What is the dose-limiting toxicity for this agent? What infections are currently circulating? Clinical decisions are never static — the target changes with graft maturation, disease flares, concurrent infections, and co-administered drugs.
Classification of Immunomodulators
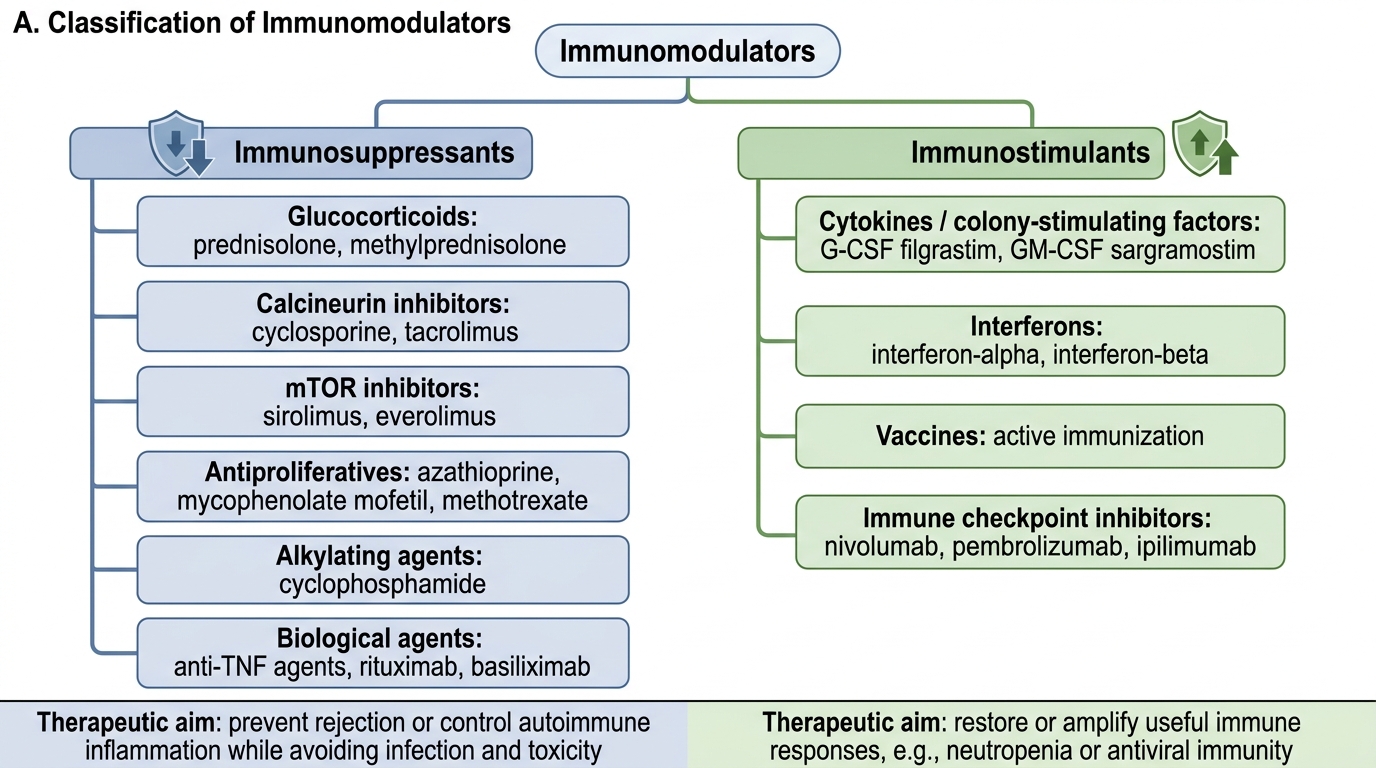
Immunomodulators are classified into two major groups based on whether they dampen or enhance immune function. It is essential to keep these groups conceptually distinct, because their indications, adverse-effect profiles, and monitoring requirements differ completely.
Immunosuppressants act by inhibiting lymphocyte activation, proliferation, or effector function. They are further divided by molecular mechanism:
- Calcineurin inhibitors: cyclosporine, tacrolimus — block IL-2 gene transcription
- Antiproliferatives: azathioprine, mycophenolate mofetil — block DNA synthesis in proliferating lymphocytes
- mTOR inhibitors: sirolimus (rapamycin), everolimus — block IL-2 receptor downstream signalling
- Corticosteroids: prednisolone, methylprednisolone — broad anti-inflammatory and lympholytic effects
- Monoclonal antibodies and biologics: basiliximab (anti-CD25), rituximab (anti-CD20), infliximab/adalimumab (anti-TNF-α), abatacept (CTLA-4 fusion)
- Small molecule JAK inhibitors: tofacitinib, baricitinib — block cytokine signalling via JAK-STAT pathway
Immunostimulants act by augmenting immune cell production, activation, or function:
- Interferons: IFN-α (antiviral/anti-tumour), IFN-β (MS), IFN-γ (CGD)
- Colony-stimulating factors: G-CSF (filgrastim — neutrophil stimulation), GM-CSF (sargramostim)
- Interleukins: IL-2 (aldesleukin — renal cell carcinoma/melanoma)
- Thymosins: thymosin-α1 (hepatitis B/C, immune restoration)
- Levamisole: antihelminthic with T-cell co-stimulatory effect; historically used as colon cancer adjuvant
- BCG: live attenuated Mycobacterium bovis; non-specific immunostimulant; used intravesically for superficial bladder cancer and as TB vaccine
SELF-CHECK
Which of the following drug pairs correctly identifies the mechanism of calcineurin inhibitors?
A. Cyclosporine and tacrolimus — inhibit IMPDH to block de novo purine synthesis
B. Cyclosporine and tacrolimus — inhibit calcineurin to prevent NFAT-driven IL-2 transcription
C. Sirolimus and everolimus — inhibit calcineurin to prevent NFAT-driven IL-2 transcription
D. Azathioprine and mycophenolate — inhibit calcineurin to prevent NFAT-driven IL-2 transcription
Reveal Answer
Answer: B. Cyclosporine and tacrolimus — inhibit calcineurin to prevent NFAT-driven IL-2 transcription
Cyclosporine and tacrolimus are calcineurin inhibitors — they block the phosphatase calcineurin, preventing dephosphorylation and nuclear translocation of NFAT, which abolishes IL-2 gene transcription. IMPDH inhibition is the mechanism of mycophenolate mofetil; mTOR inhibition is the mechanism of sirolimus/everolimus.