Page 2 of 33
PH9.1 | PH9.1 | Immunomodulators — SDL Guide — SDL Guide (Part 2)
Immunosuppressants: PK, PD, Uses and ADRs
Understanding the pharmacokinetics (PK) and pharmacodynamics (PD) of each immunosuppressant class is essential because most have narrow therapeutic indices and serious organ-specific toxicities that require monitoring.
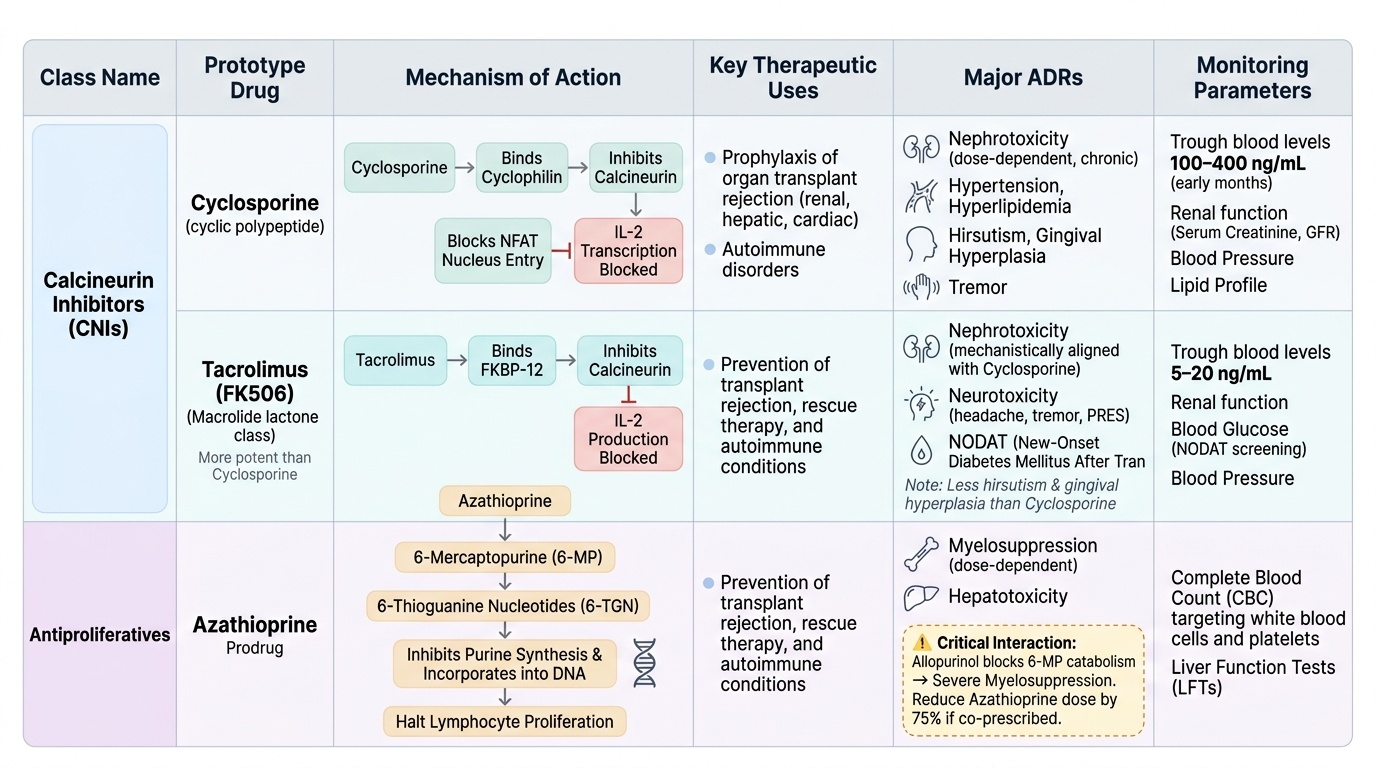
Calcineurin inhibitors — cyclosporine and tacrolimus:
Cyclosporine is a cyclic polypeptide fungal metabolite. It is orally absorbed (bioavailability 30–45%; highly variable — Neoral microemulsion formulation improves consistency) and extensively distributed; primarily metabolised by CYP3A4 in the liver and intestine. Elimination is predominantly biliary. Its narrow therapeutic index demands trough blood level monitoring (transplant target varies by organ and time post-transplant, generally 100–400 ng/mL in early months). Mechanism: cyclosporine binds cyclophilin → the complex inhibits calcineurin → NFAT cannot enter the nucleus → IL-2 gene transcription blocked. ADRs: nephrotoxicity (dose-dependent and chronic, limiting long-term use), hypertension, hyperlipidaemia, hirsutism, gingival hyperplasia, tremor, hepatotoxicity (less common).
Tacrolimus (FK506) is a macrolide lactone. Oral bioavailability variable (14–24%); metabolised by CYP3A4. More potent than cyclosporine on a weight basis. Mechanism: binds FKBP-12 → tacrolimus-FKBP12 complex inhibits calcineurin. Therapeutic trough range: typically 5–20 ng/mL (organ and indication-specific). ADRs: nephrotoxicity (same mechanism as cyclosporine; predominant long-term risk), neurotoxicity (tremor, headache, posterior reversible encephalopathy syndrome — more prominent than cyclosporine), new-onset diabetes mellitus after transplantation (NODAT), hypertension. Note: tacrolimus causes less hirsutism and gingival hyperplasia than cyclosporine — relevant for patient selection.
Antiproliferatives:
Azathioprine is a prodrug hydrolysed to 6-mercaptopurine (6-MP), which is then metabolised to 6-thioguanine nucleotides (6-TGN) that inhibit purine synthesis and are incorporated into DNA, halting lymphocyte proliferation. Oral bioavailability ~50%. Key interaction: allopurinol (a xanthine oxidase inhibitor) blocks azathioprine catabolism → 6-MP accumulates → severe myelosuppression. Azathioprine dose must be reduced by 75% if allopurinol is co-prescribed. ADRs: myelosuppression (dose-dependent), hepatotoxicity, nausea, increased malignancy risk (especially non-melanoma skin cancer and lymphoma) with long-term use.
Mycophenolate mofetil (MMF) is a prodrug of mycophenolic acid (MPA). MPA is a selective, reversible inhibitor of inosine monophosphate dehydrogenase (IMPDH), the rate-limiting enzyme in de novo purine synthesis. T and B lymphocytes rely almost entirely on the de novo pathway (unlike most other cells that can use the salvage pathway), making MMF relatively lymphocyte-selective. Oral bioavailability ~90%. ADRs: gastrointestinal (diarrhoea, nausea — the dose-limiting toxicity in practice), myelosuppression (leukopenia), increased infection risk, teratogenicity (absolute contraindication in pregnancy). Standard maintenance dose: 1–1.5 g twice daily in transplant recipients.
mTOR inhibitors:
Sirolimus (rapamycin) and everolimus bind FKBP-12 (same binding protein as tacrolimus) but, unlike tacrolimus, the sirolimus-FKBP12 complex does NOT inhibit calcineurin — instead, it inhibits mTOR (mammalian target of rapamycin), blocking T-cell cycle progression from G1 to S phase downstream of the IL-2 receptor. This distinguishes them mechanistically from both calcineurin inhibitors and antiproliferatives. ADRs: hyperlipidaemia (triglycerides and cholesterol), impaired wound healing, thrombocytopenia, oral ulcers, interstitial pneumonitis (class effect), less nephrotoxic than calcineurin inhibitors (an advantage in patients with calcineurin inhibitor-induced renal impairment).
Monoclonal antibodies and biologics:
Basiliximab is a chimeric anti-CD25 (IL-2 receptor α-chain) monoclonal antibody used for induction immunosuppression in renal transplantation. It saturates CD25 on activated T-cells, blocking IL-2 signalling at the receptor level.
Rituximab is a chimeric anti-CD20 monoclonal antibody that depletes mature B-cells (CD20+ cells) via complement-dependent cytotoxicity and antibody-dependent cellular cytotoxicity (ADCC). Uses: lymphoma (original indication), RA, granulomatosis with polyangiitis, pemphigus. Risk: progressive multifocal leukoencephalopathy (PML, JC virus), hepatitis B reactivation.
Infliximab and adalimumab are anti-TNF-α agents (infliximab: chimeric monoclonal antibody; adalimumab: fully human monoclonal antibody). TNF-α blockade reduces the inflammatory cascade in RA, Crohn's disease, psoriatic arthritis, ankylosing spondylitis. Risk: tuberculosis reactivation (screen with Mantoux test and chest X-ray BEFORE starting), opportunistic infections, worsening heart failure.
JAK inhibitors — tofacitinib and baricitinib are small molecules (oral, not injectable like biologics) that block the JAK-STAT intracellular signalling pathway used by multiple cytokines. ADRs class: serious infections, herpes zoster reactivation, venous thromboembolism (baricitinib — FDA warning), potential increased malignancy risk.
Provided image
Immunostimulants: PK, PD, Uses and ADRs
Immunostimulants enhance a deficient or inadequate immune response. They are used in settings ranging from post-chemotherapy neutropenia to viral hepatitis, immunodeficiency states, and certain malignancies.
Provided image
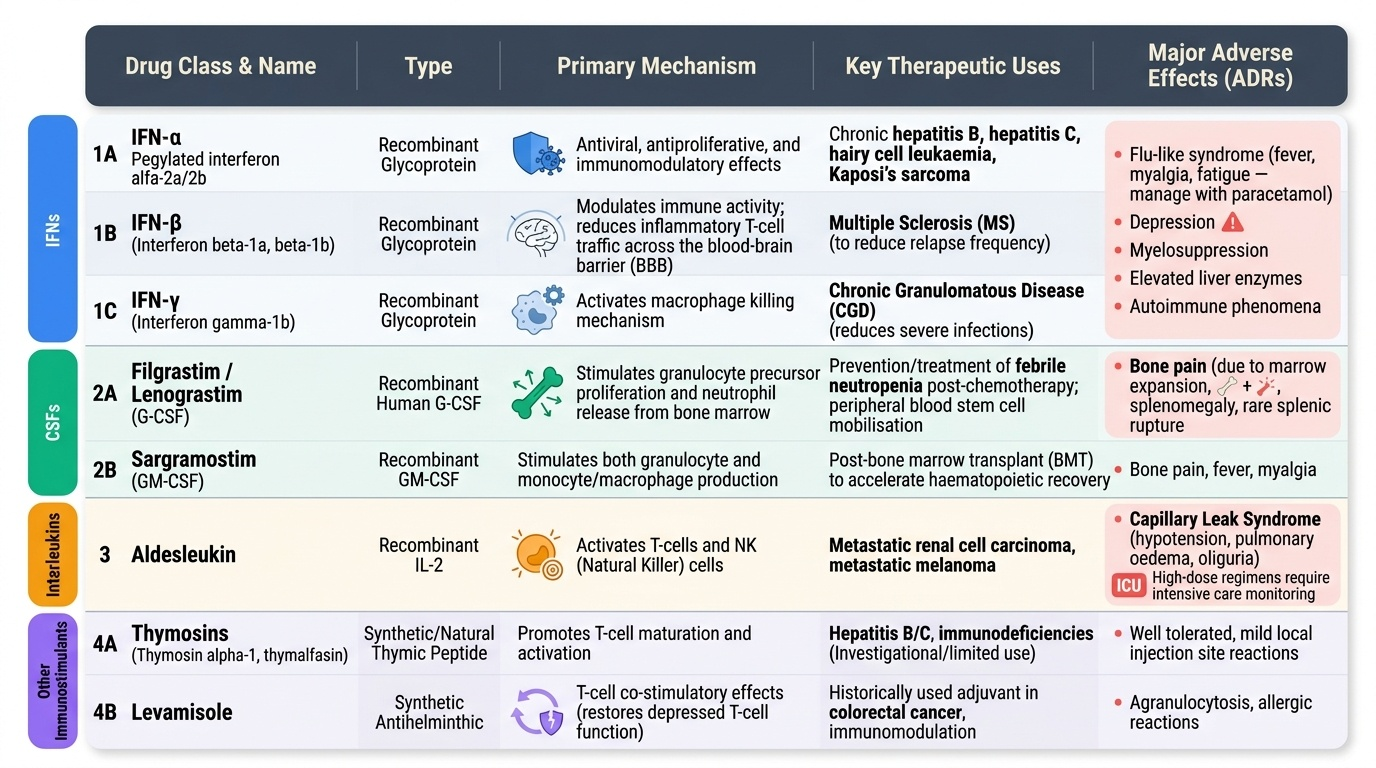
Interferons (IFNs) are glycoproteins produced by virus-infected cells and immune cells. Recombinant forms are used therapeutically. IFN-α (pegylated interferon alfa-2a/2b) has antiviral, antiproliferative, and immunomodulatory effects; historically used for chronic hepatitis B, hepatitis C (now largely replaced by direct-acting antivirals), hairy cell leukaemia, and Kaposi's sarcoma. IFN-β (interferon beta-1a, beta-1b) modulates immune activity in multiple sclerosis by reducing inflammatory T-cell traffic across the blood-brain barrier. IFN-γ (interferon gamma-1b) activates macrophage killing and is used in chronic granulomatous disease (CGD) to reduce the frequency of severe infections. ADRs of all interferons: flu-like syndrome (fever, myalgia, fatigue — characteristically after injection; managed by pre-dosing with paracetamol), depression (significant, can be disabling), myelosuppression, elevated liver enzymes, autoimmune phenomena.
Colony-stimulating factors (CSFs):
Filgrastim (recombinant human G-CSF) and lenograstim stimulate granulocyte precursor proliferation and neutrophil release from bone marrow. Primary use: prevention and treatment of febrile neutropenia after cytotoxic chemotherapy, and peripheral blood stem cell mobilisation before harvest for transplant. ADRs: bone pain (most common, due to marrow expansion), splenomegaly (with prolonged use), rare: splenic rupture.
Sargramostim (GM-CSF) stimulates both granulocyte and monocyte/macrophage production; used post-BMT to accelerate haematopoietic recovery.
Interleukins:
Aldesleukin (recombinant IL-2) activates T-cells and NK cells; approved for metastatic renal cell carcinoma and metastatic melanoma (high-dose regimen). ADRs: severe: capillary leak syndrome (hypotension, pulmonary oedema, oliguria) — high-dose regimen requires intensive care monitoring.
Thymosins (thymosin alpha-1, thymalfasin): naturally occurring thymic peptides that promote T-cell maturation and activation. Investigational/limited use in hepatitis B/C and immunodeficiency.
Levamisole is an antihelminthic drug with T-cell co-stimulatory effects (restores depressed T-cell function). It was historically used as an adjuvant in colon cancer treatment but is no longer standard practice because the benefit was modest and toxicity (agranulocytosis) was significant. It is no longer a first-line immunostimulant.
BCG (Bacille Calmette-Guérin) is a live attenuated strain of Mycobacterium bovis. As an immunostimulant, it activates macrophages and T-cells via innate immune pattern recognition. Clinical use: (1) intravesical BCG therapy for superficial (non-muscle-invasive) bladder cancer — the most effective intravesical treatment to reduce recurrence and progression; (2) intradermal BCG vaccination for tuberculosis prevention (immune protection, not immunostimulant in the pharmacological sense but mechanism is the same). ADRs of intravesical BCG: cystitis (very common), haematuria, flu-like symptoms, rare disseminated BCG infection (BCG-osis) in immunocompromised patients.
SELF-CHECK
A patient on azathioprine develops gout and is started on allopurinol. Which serious toxicity is most likely to occur if the azathioprine dose is not adjusted?
A. Cyclosporine-induced nephrotoxicity
B. Severe myelosuppression due to 6-mercaptopurine accumulation
C. Hepatitis B reactivation due to B-cell depletion
D. Capillary leak syndrome from IL-2 release
Reveal Answer
Answer: B. Severe myelosuppression due to 6-mercaptopurine accumulation
Allopurinol inhibits xanthine oxidase, which is the enzyme that degrades 6-mercaptopurine (the active metabolite of azathioprine). When xanthine oxidase is blocked, 6-MP accumulates to toxic levels, causing severe myelosuppression (leukopenia, thrombocytopenia, anaemia). The azathioprine dose must be reduced by approximately 75% if allopurinol is unavoidable — or ideally, allopurinol should be replaced with febuxostat (which does not interact with azathioprine to the same degree).
Clinical Decision-Making in Immunomodulator Use
Clinical decision-making with immunomodulators requires integrating mechanism, toxicity profile, monitoring requirements, and patient-specific factors (renal function, concurrent infections, drug interactions, pregnancy status).
Transplant immunosuppression — standard triple therapy: Most solid organ transplant centres use a calcineurin inhibitor + antiproliferative + corticosteroid (e.g. tacrolimus + mycophenolate mofetil + prednisolone). Induction therapy with basiliximab is added in high-rejection-risk recipients. Choice of tacrolimus vs cyclosporine: tacrolimus is preferred in most centres for its superior rejection prophylaxis; cyclosporine may be chosen where NODAT risk is a concern or where tacrolimus neurotoxicity has occurred.
Monitoring for calcineurin inhibitors: Trough blood levels are measured regularly (tacrolimus 5–15 ng/mL at 3–6 months post-transplant, lower in stable patients; cyclosporine 100–400 ng/mL depending on organ and time post-transplant). Serial creatinine monitoring is essential because nephrotoxicity may be indistinguishable from rejection on clinical grounds alone — biopsy is then required.
Drug interactions: CYP3A4 is a critical interaction point for cyclosporine and tacrolimus. Strong CYP3A4 inducers (rifampicin, phenytoin, carbamazepine) dramatically reduce levels → rejection risk. Strong CYP3A4 inhibitors (azole antifungals, macrolide antibiotics, grapefruit juice) dramatically increase levels → toxicity risk. These interactions are clinically common and potentially fatal.
Autoimmune disease strategy — step-up approach: In conditions like RA, treatment follows a step-up ladder: conventional DMARDs first (methotrexate, hydroxychloroquine, sulfasalazine), then biologics (anti-TNF agents, rituximab, abatacept, JAK inhibitors) if conventional DMARDs fail. Before starting anti-TNF agents or JAK inhibitors: screen for latent tuberculosis (Mantoux test + CXR), hepatitis B and C serology, and live vaccine catch-up (because live vaccines are contraindicated once biologics are started).
Balancing infection risk: Every immunosuppressed patient is at risk for opportunistic infections — Pneumocystis jirovecii pneumonia (PCP), CMV, fungal infections (Aspergillus, Candida), tuberculosis. Co-trimoxazole prophylaxis is standard in transplant recipients; CMV prophylaxis with valganciclovir is given in high-risk combinations.
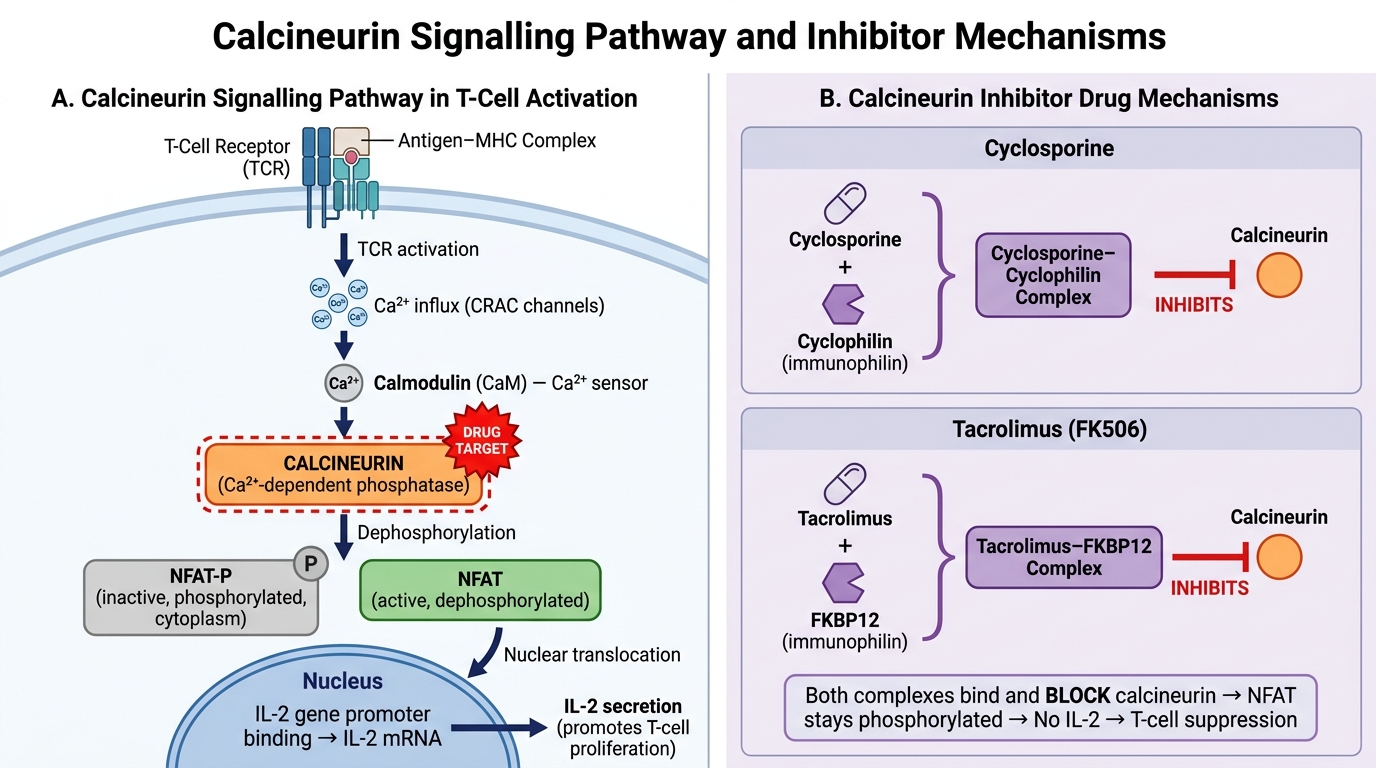
Calcineurin Inhibitor Mechanism of Action in T-Cell Signalling
CLINICAL PEARL
Clinical Pearl: TNF-α inhibitors and tuberculosis reactivation. Infliximab and adalimumab cause significantly increased risk of reactivating latent tuberculosis — TB granulomas require TNF-α for their structural integrity, and TNF-α blockade causes granuloma dissolution. Every patient must be screened with a tuberculin skin test (TST) or interferon-gamma release assay (IGRA) AND a chest X-ray before starting anti-TNF therapy. If latent TB is found, complete an INH prophylaxis course (at least 1 month into treatment, ideally full course) before initiating the biologic. Failure to screen has caused deaths from disseminated TB. This rule also applies to JAK inhibitors and other biologics.