Page 8 of 33
PH9.2 | PH9.2 | Common Toxicology Emergencies — SDL Guide — SDL Guide
Learning Objectives
- Recognise common toxidromes and their causative agents
- Describe the mechanism of toxicity and specific antidote for paracetamol, opioid, benzodiazepine, and organophosphate poisoning
- Outline the management of common insecticide poisonings, bee/wasp stings, scorpion stings, and snake bites in the Indian clinical context
- Apply a systematic ABCDE approach to poisoning emergencies with correct antidote selection
INSTRUCTIONS
Poisoning is a common medical emergency in India — organophosphate ingestion in agricultural settings, paracetamol overdose in suicidal attempts, and snake bite in rural areas account for a significant proportion of emergency department admissions. This module teaches you to rapidly recognise the toxidrome, select the correct antidote (and understand why it works), and manage these emergencies systematically. Understanding the pharmacology of antidotes is as important as the antidotes themselves.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 63 (Pharmacology of Toxicology) (textbook)
- Goodman & Gilman. The Pharmacological Basis of Therapeutics, 13th ed., Ch. 4 (Principles of Toxicology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old woman is brought to the emergency department at 2 AM by her family after ingesting 'a fistful of tablets' of paracetamol 8 hours ago following a domestic argument. She is currently alert, with mild nausea — no signs of liver failure yet. Her serum paracetamol level is 150 mg/L. The emergency resident asks: 'She looks fine — can we just observe?' The answer is no. Paracetamol-induced hepatic necrosis peaks at 72–96 hours after ingestion, and N-acetylcysteine is most effective when started within the first 8–10 hours. Delay here causes permanent liver damage. This case illustrates the core principle of toxicology management: the clinical presentation at presentation does NOT predict the trajectory — pharmacokinetics and mechanism of toxicity determine what happens next.
WHY THIS MATTERS
Toxicology emergencies are among the highest-acuity cases in emergency medicine and internal medicine. In India, organophosphate poisoning — primarily from agricultural pesticide ingestion — is the leading cause of poisoning mortality. Paracetamol overdose is the most common drug overdose presenting to urban emergency departments. Snake bites cause an estimated 50,000–60,000 deaths annually in India (the world's highest burden). Understanding the pharmacology of these poisonings and their antidotes is directly life-saving. The Pharmacology competency PH9.2 maps directly to clinical emergency scenarios you will face from your third year onward.
RECALL
From your General Pharmacology study, recall that NAPQI (N-acetyl-p-benzoquinone imine) is the reactive hepatotoxic metabolite of paracetamol formed by CYP2E1. It is normally detoxified by conjugation with glutathione, but in overdose, glutathione is depleted and NAPQI accumulates, causing centrilobular hepatic necrosis. From the Autonomic Nervous System cluster, recall the distinction between muscarinic effects (SLUDGE: salivation, lacrimation, urination, defaecation, GI distress, emesis) and nicotinic effects (muscle fasciculations, weakness, tachycardia, hypertension) — this distinction is critical for understanding organophosphate toxicity and the selective action of atropine vs pralidoxime. Recall that opioids act on mu (μ), kappa (κ), and delta (δ) receptors — the classic triad of opioid overdose (respiratory depression, miosis, coma) results primarily from μ-receptor activation.
Poisoning as a Medical Emergency: Toxidrome Recognition
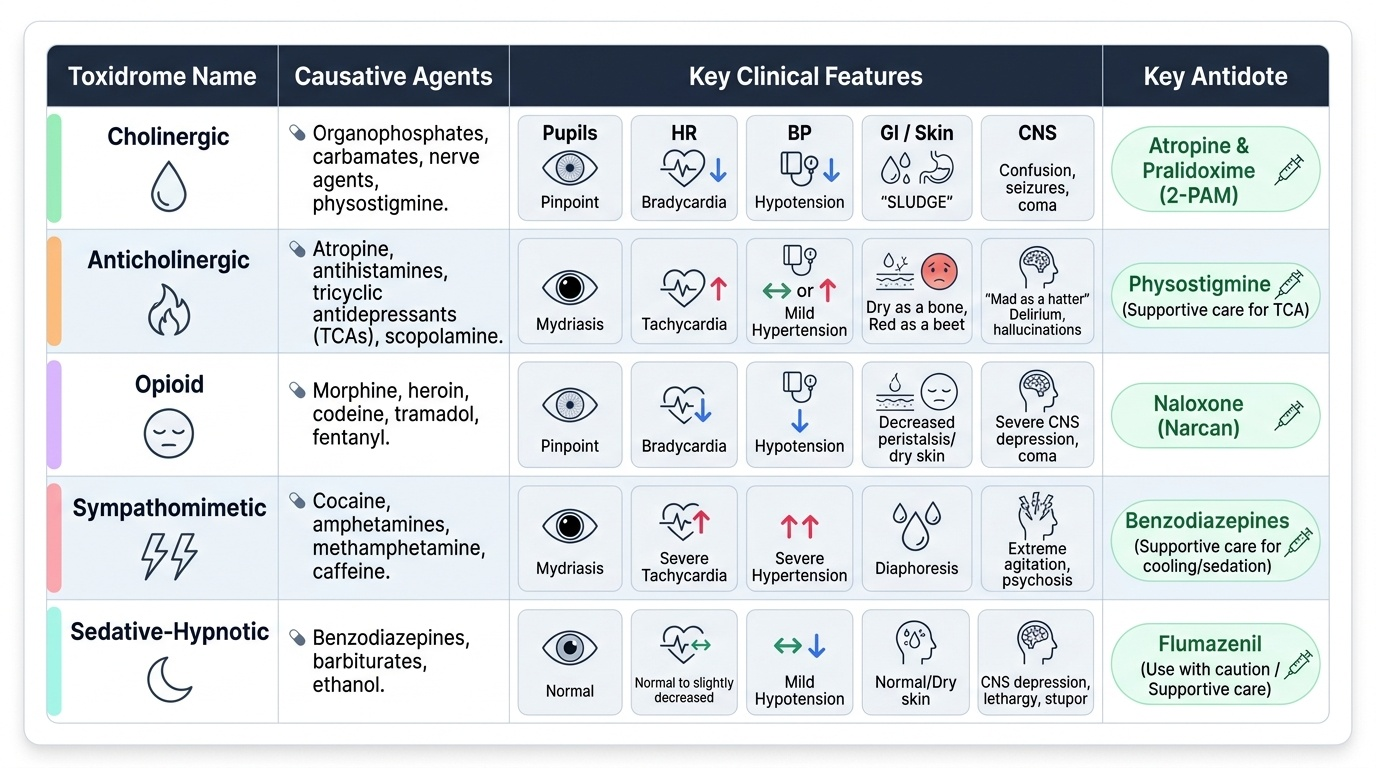
A toxidrome is a syndrome produced by a specific class of toxins — a characteristic cluster of signs and symptoms that points to the causative agent and guides antidote selection before laboratory confirmation. Recognising the toxidrome is the first and most critical step in managing any poisoning patient, because it allows empirical antidote administration when time is critical.
Provided image
The five classic toxidromes are:
- Cholinergic toxidrome: caused by organophosphates, carbamates, physostigmine, nerve agents. Excess acetylcholine at all cholinergic synapses. Features: SLUDGE (salivation, lacrimation, urination, defaecation, GI distress, emesis) + bronchospasm/bronchorrhoea + miosis (pinpoint pupils) + bradycardia (muscarinic, predominantly). Plus nicotinic effects: fasciculations, weakness, tachycardia. Plus CNS: confusion, seizures, coma.
- Anticholinergic toxidrome: caused by atropine, antihistamines, tricyclic antidepressants, scopolamine. Features: 'hot as hell, blind as a bat, dry as a bone, red as a beet, mad as a hatter' — hyperthermia, mydriasis (dilated pupils), dry skin/mouth, flushing, delirium/hallucinations.
- Opioid toxidrome: caused by morphine, heroin, codeine, tramadol. Features: miosis (pinpoint pupils), respiratory depression (rate <12/min), reduced consciousness, hypotension, bradycardia.
- Sympathomimetic toxidrome: caused by cocaine, amphetamines, caffeine excess. Features: mydriasis, tachycardia, hypertension, hyperthermia, agitation/psychosis.
- Sedative-hypnotic toxidrome: benzodiazepines, barbiturates, ethanol. Features: CNS depression, respiratory depression, normal pupils (neither pinpoint nor dilated), normal BP.
The general approach to any poisoning patient uses ABCDE resuscitation first: Airway (clear, intubate if GCS ≤8 or airway threat), Breathing (supplemental oxygen, mechanically ventilate if needed), Circulation (IV access, fluids, vasopressors), Disability (GCS, pupils, blood glucose), Exposure (look for injection sites, burns, trauma). Only after initial stabilisation should definitive antidote therapy and decontamination be pursued.
Therapeutic Goals in Poisoning Management
The therapeutic goals in poisoning management follow a consistent hierarchy, regardless of the specific agent. Understanding this hierarchy prevents the common error of reaching for an antidote before the patient is stabilised.
Priority 1 — Resuscitation: Maintain the airway, ventilation, and circulation. Most poisoning deaths occur from respiratory arrest, cardiac arrhythmia, or cardiovascular collapse before any antidote is administered. Supportive care is the backbone of toxicology management — specific antidotes exist for only a minority of poisons.
Priority 2 — Antidote administration (when available and indicated): A specific antidote is a drug or treatment that counteracts the toxic mechanism of the poison. The most important antidotes in clinical practice include N-acetylcysteine (paracetamol), naloxone (opioids), flumazenil (benzodiazepines), atropine + pralidoxime (organophosphates), and antivenom (snake bites). The pharmacological goal is to either restore the disrupted receptor/enzyme function (pralidoxime reactivates AChE; naloxone competitively displaces the opioid) or replenish depleted endogenous defence mechanisms (NAC replenishes glutathione).
Priority 3 — Decontamination: Reduce further absorption of the toxin. Gastric lavage is now used rarely and only within 1 hour of ingestion for significant life-threatening poisonings. Activated charcoal (50 g in adults, 1 g/kg in children) adsorbs many drugs if given within 1–2 hours of ingestion — contraindicated for caustics, alcohols, and hydrocarbons. Whole bowel irrigation with polyethylene glycol is used for sustained-release preparations and iron poisoning.
Priority 4 — Enhanced elimination: For some poisons, active removal measures are warranted. Alkalinisation of urine (IV sodium bicarbonate to urine pH 7.5–8.5) enhances elimination of aspirin and phenobarbitone by ion-trapping. Haemodialysis removes small, water-soluble, low-protein-bound toxins: salicylates, methanol, ethylene glycol, lithium, metformin. Multiple-dose activated charcoal (MDAC) enhances elimination of drugs with enterohepatic recycling (carbamazepine, phenobarbitone, theophylline).
Classification of Common Poisonings
For clinical and educational purposes, PH9.2 covers four categories of poisoning, each with its own toxidrome, mechanism, and antidote strategy. It is essential to keep the antidote-poison pairs clear — giving the wrong antidote (or giving atropine alone without pralidoxime in severe organophosphate poisoning) is a preventable clinical error.
A. Common drug poisonings:
- Paracetamol overdose → NAPQI-mediated hepatotoxicity → antidote: N-acetylcysteine (NAC)
- Opioid overdose → respiratory depression via μ-receptor → antidote: naloxone
- Benzodiazepine overdose → GABA-A potentiation → antidote: flumazenil (use with caution)
- Organophosphate poisoning → AChE inhibition → cholinergic toxidrome → antidote: atropine + pralidoxime
B. Insecticide poisonings:
- Organophosphates (malathion, parathion, chlorpyrifos) — AChE inhibition; same management as above
- Carbamates (carbofuran, carbaryl) — reversible AChE inhibition; atropine; pralidoxime controversial (may worsen carbamate poisoning — NOT recommended by some authorities)
- Pyrethroids — sodium channel disruptors; no specific antidote; supportive care
C. Common stings:
- Bee/wasp (Hymenoptera) stings → anaphylaxis → epinephrine (adrenaline) 0.5 mg IM (1:1000) first-line
- Scorpion stings — Indian red scorpion (Mesobuthus tamulus): autonomic storm (massive catecholamine release → hypertension, pulmonary oedema, myocarditis) → prazosin (α-1 blocker); supportive care
D. Common bites:
- Snake bites (the 'Big Four' in India): neurotoxic (krait, cobra — progressive flaccid paralysis, respiratory failure); hemotoxic (Russell's viper, saw-scaled viper — coagulopathy, haemorrhage, local necrosis) → polyvalent antivenom (ASV); diagnose coagulopathy with 20-minute whole blood clotting test (20WBCT)
- Dog bite → rabies prophylaxis (wound wash + anti-rabies vaccine ± rabies immunoglobulin)
SELF-CHECK
A farmer is brought to the casualty unconscious, with pinpoint pupils, profuse salivation, bronchospasm, and muscle fasciculations. Which toxidrome does this represent, and what is the FIRST specific antidote that should be administered?
A. Anticholinergic toxidrome — administer flumazenil IV
B. Opioid toxidrome — administer naloxone IV and maintain airway
C. Cholinergic toxidrome from organophosphate poisoning — secure airway, then administer atropine IV (titrated until secretions dry)
D. Sympathomimetic toxidrome — administer labetalol for hypertension
Reveal Answer
Answer: C. Cholinergic toxidrome from organophosphate poisoning — secure airway, then administer atropine IV (titrated until secretions dry)
The classic cholinergic toxidrome — SLUDGE + bronchospasm + miosis + fasciculations + CNS depression — is caused by organophosphate poisoning, which irreversibly inhibits acetylcholinesterase. After securing the airway and providing oxygen (critical — bronchospasm and hypoxia are the immediate killers), atropine is administered IV in large doses (2–4 mg, then doubling every 5–10 minutes) titrated until secretions dry — this is the muscarinic blockade endpoint. Pralidoxime (an AChE reactivator) is given concurrently but must be started early before 'aging' of the organophosphate-AChE bond makes it irreversible. Flumazenil is for benzodiazepine overdose; naloxone for opioids.