Page 9 of 33
PH9.2 | PH9.2 | Common Toxicology Emergencies — SDL Guide — SDL Guide (Part 2)
Drug Poisonings: Paracetamol, Opioids, Benzodiazepines
The three most common drug poisonings in clinical practice each have a specific, well-defined mechanism and antidote — understanding the mechanism is what makes the antidote choice rational rather than rote.
Paracetamol (acetaminophen) poisoning:
Paracetamol is metabolised primarily by glucuronidation and sulfation (>90% of therapeutic doses). A small fraction is oxidised by CYP2E1 to NAPQI (N-acetyl-p-benzoquinone imine), a highly reactive hepatotoxic metabolite. At therapeutic doses, NAPQI is rapidly conjugated with glutathione (GSH) and rendered harmless. In overdose (>150 mg/kg or >7.5 g in adults), glucuronidation and sulfation are saturated, more paracetamol is shunted through CYP2E1, and glutathione is depleted below 30% of normal — NAPQI accumulates and binds covalently to hepatocyte proteins, causing centrilobular hepatic necrosis.
Clinical course: Phase 1 (0–24 h) — nausea, vomiting, malaise (may be absent); Phase 2 (24–72 h) — apparent improvement, but LFTs rising; Phase 3 (72–96 h) — peak hepatotoxicity (jaundice, coagulopathy, encephalopathy, acute liver failure — the danger zone); Phase 4 — resolution or death.
Antidote — N-acetylcysteine (NAC): NAC replenishes glutathione stores (it is a GSH precursor/substitute) and directly neutralises NAPQI. It also acts as an antioxidant. Effectiveness is time-dependent: most effective within 8–10 hours of ingestion; still beneficial up to 24 hours; less effective after 24 hours when hepatic necrosis is established but can still reduce severity. IV protocol (21-hour regimen): 150 mg/kg loading dose over 15–60 min, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours. Decision to treat is guided by the Rumack-Matthew nomogram (serum paracetamol level plotted against time post-ingestion at 4 hours minimum); levels above the treatment line indicate NAC therapy.
Opioid overdose:
Opioids (morphine, heroin, codeine, tramadol, fentanyl, oxycodone) cause the classic triad of miosis (pinpoint pupils), respiratory depression (rate <12/min), and altered consciousness through μ-opioid receptor activation in the brainstem respiratory centres, locus coeruleus, and Edinger-Westphal nucleus. Respiratory arrest is the immediate cause of death.
Antidote — Naloxone: Naloxone is a competitive antagonist at all three opioid receptors (μ, κ, δ) with highest affinity for μ-receptors. It reverses respiratory depression, sedation, and miosis rapidly (within 2–5 minutes IV). Half-life of naloxone (approximately 60–90 minutes) is SHORTER than most opioids — repeat doses or infusion required to prevent re-narcotisation. Dose: 0.4–2 mg IV/IM/SC; may repeat every 2–3 minutes; if no response after 10 mg, question the diagnosis. In opioid-dependent patients, naloxone can precipitate acute withdrawal — administer cautiously, titrating to respiratory rate rather than consciousness.
Benzodiazepine overdose:
Benzodiazepines potentiate GABA-A receptor chloride channel opening, causing CNS depression (sedation, anxiolysis, anticonvulsant effects, muscle relaxation). In overdose: excessive sedation, respiratory depression (usually mild unless combined with alcohol or opioids), and hypotension.
Antidote — Flumazenil: Competitive antagonist at the benzodiazepine binding site of GABA-A receptor. Reverses benzodiazepine-induced sedation rapidly. Short-acting (30–60 min) — resedation occurs as it wears off; may need repeat dosing. Critical contraindications: (1) Patients with known or suspected tricyclic antidepressant (TCA) co-ingestion — flumazenil removes GABA-mediated seizure protection and can precipitate life-threatening seizures; (2) Patients using benzodiazepines chronically for seizure prophylaxis — flumazenil can cause acute withdrawal and status epilepticus.
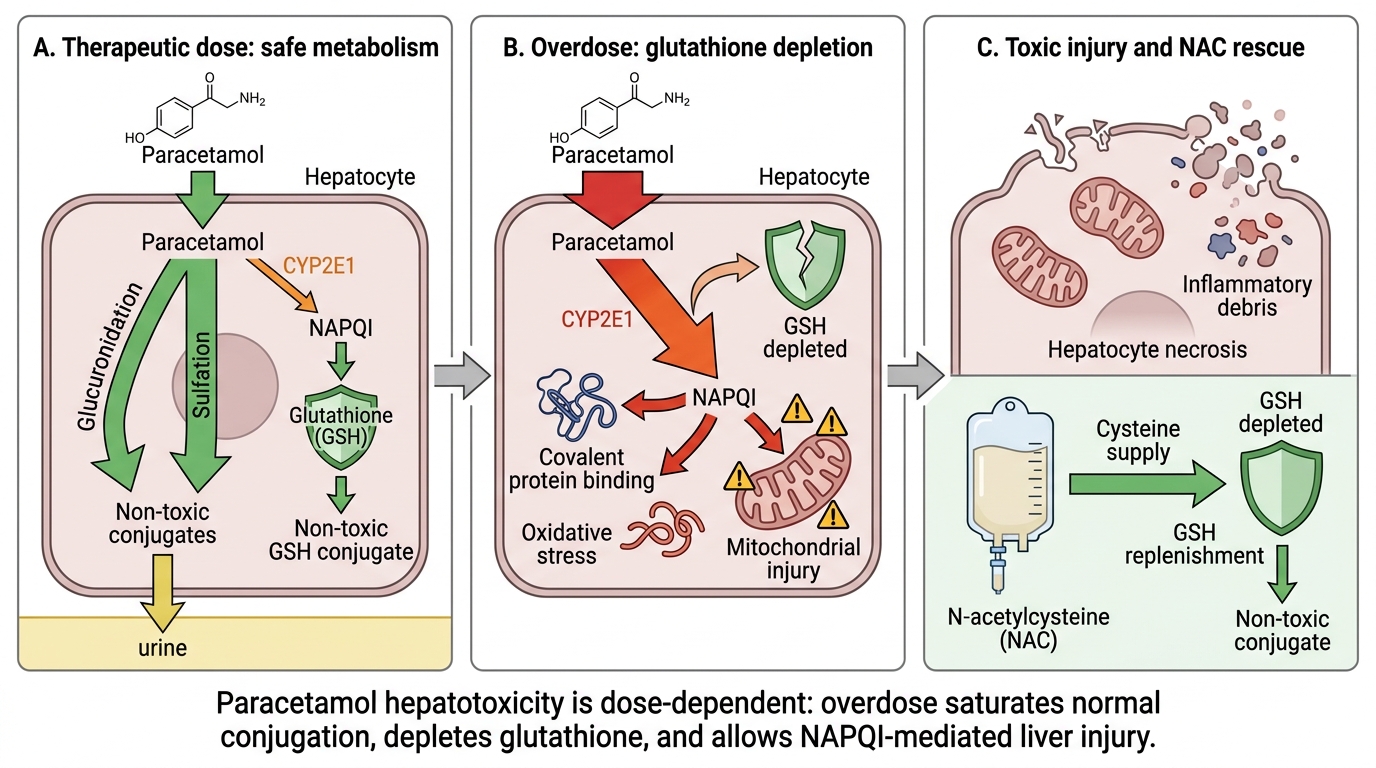
Mechanism of Paracetamol Hepatotoxicity and NAC Rescue
SELF-CHECK
A 45-year-old man with chronic back pain and opioid dependence is found unresponsive with a respiratory rate of 4/min and pinpoint pupils. He is given naloxone 0.4 mg IV with dramatic improvement — GCS 15, respiratory rate 18/min — but 2 hours later he becomes deeply sedated again. What is the most appropriate next step?
A. Administer flumazenil — he likely co-ingested benzodiazepines
B. Repeat naloxone administration or start a naloxone infusion, because naloxone's half-life is shorter than most opioids and re-narcotisation is expected
C. Administer N-acetylcysteine — the paracetamol in his combination pain medications has caused liver failure
D. No further medication is needed — the initial naloxone response confirms the diagnosis and he will recover spontaneously
Reveal Answer
Answer: B. Repeat naloxone administration or start a naloxone infusion, because naloxone's half-life is shorter than most opioids and re-narcotisation is expected
Naloxone has a half-life of approximately 60–90 minutes, which is shorter than most opioids (e.g. morphine 2–4 hours; methadone 15–55 hours; oxycodone 4–6 hours; heroin metabolites persist longer). Once the naloxone is metabolised, the opioid reasserts its effect and re-narcotisation occurs — this is a well-recognised and predictable phenomenon. Management: repeated bolus dosing or a continuous naloxone infusion (two-thirds of the effective bolus dose per hour) titrated to maintain adequate ventilation. The patient must be monitored for the duration of the opioid effect.
Insecticide Poisoning and Stings and Bites
Organophosphate and carbamate insecticide poisoning, common stings, and snake bites are major toxicological emergencies in India, particularly in rural settings.
Organophosphate (OP) poisoning:
Organophosphates (malathion, parathion, chlorpyrifos, dimethoate, dichlorvos) irreversibly inhibit acetylcholinesterase (AChE), causing accumulation of acetylcholine at all cholinergic synapses: muscarinic (smooth muscle, glands, SA/AV node) and nicotinic (neuromuscular junction, autonomic ganglia) and in the CNS. The cholinergic toxidrome is the result: SLUDGE at muscarinic synapses, fasciculations and weakness at nicotinic synapses, and confusion/seizures/coma centrally.
Management: (1) Personal protective equipment before touching the patient (skin absorption continues to poison healthcare workers); (2) ABCDE resuscitation with immediate high-flow oxygen and airway protection; (3) Atropine — the muscarinic antagonist, given in large and repeated IV doses (starting 2–4 mg, repeating every 5–10 minutes) until secretions dry (the clinical endpoint — do NOT target heart rate or pupil size, as nicotinic and CNS effects are unaffected by atropine); (4) Pralidoxime (2-PAM) — a cholinesterase reactivator that cleaves the organophosphate-AChE bond, restoring enzyme activity, if given BEFORE 'aging' (spontaneous, irreversible covalent modification of the OP-AChE complex that renders it permanently inactive — timing varies by agent, from hours to days).
Carbamate poisoning causes a similar but generally milder cholinergic toxidrome because carbamate-AChE inhibition is reversible (spontaneous hydrolysis). Atropine is the same. Pralidoxime is not recommended for pure carbamate poisoning because carbamates dissociate rapidly on their own and pralidoxime may paradoxically worsen the toxicity; however, if the agent is unknown (mixed or uncertain), pralidoxime is given.
Bee/wasp (Hymenoptera) stings:
Venom contains phospholipase A2, melittin, and other allergens. Most stings cause local pain and swelling. In sensitised individuals, stings trigger anaphylaxis — systemic IgE-mediated mast cell degranulation causing urticaria, angioedema, bronchospasm, and haemodynamic collapse. Treatment: Epinephrine (adrenaline) 0.5 mg IM into the anterolateral thigh (1:1000 solution) — first-line; counteracts all components of anaphylaxis via α-1 (vasoconstriction, BP↑), β-1 (heart rate and contractility↑), and β-2 (bronchodilation) effects. IV antihistamines and corticosteroids are adjuncts, NOT substitutes for epinephrine. Multiple stings can cause direct toxicity from venom (haemolysis, myonecrosis) without allergy.
Scorpion stings — Indian context:
The Indian red scorpion (Mesobuthus tamulus) is particularly lethal — it causes a massive catecholamine storm (sympathetic autonomic excess): hypertension, sweating, tachycardia, and — critically — acute pulmonary oedema and myocarditis (due to catecholamine cardiomyopathy). Treatment: Prazosin (α-1 adrenergic blocker) counteracts the catecholamine-induced vasoconstriction and hypertension; prazosin 0.5 mg sublingually followed by oral dosing. Supportive management of pulmonary oedema. NOTE: antivenom is not generally available or effective for Indian scorpion stings; scorpion antivenom exists for some species but is not the primary treatment here.
Snake bites — the 'Big Four' in India:
The four most medically significant species are:
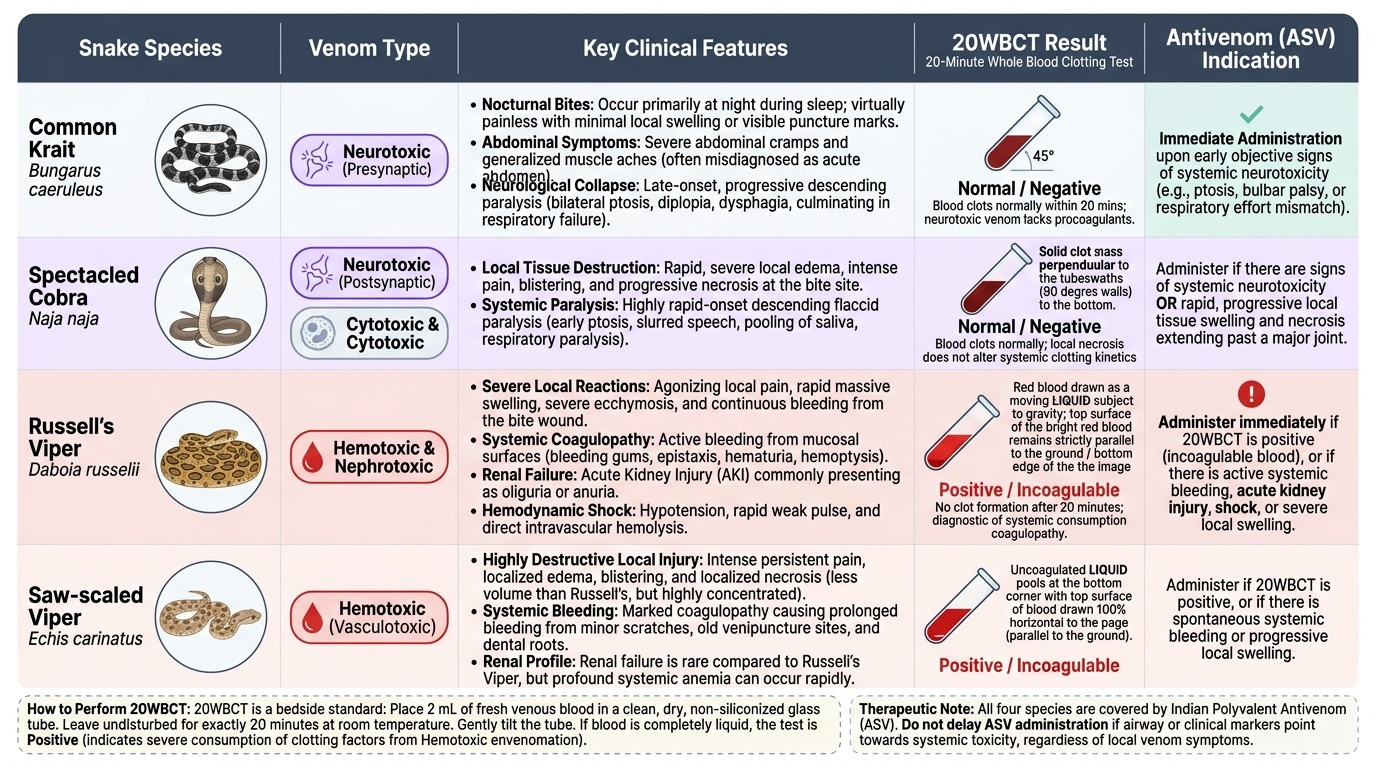
- Neurotoxic: Bungarus caeruleus (common krait) and Naja naja (Indian cobra). Post-synaptic (cobra) or pre-synaptic (krait) neurotoxins cause progressive descending flaccid paralysis beginning with ptosis, diplopia, dysphagia, and progressing to respiratory muscle paralysis and respiratory failure. Death is from respiratory arrest.
- Hemotoxic: Daboia russelii (Russell's viper) and Echis carinatus (saw-scaled viper). Venom causes venom-induced consumption coagulopathy (VICC): activation and exhaustion of clotting factors, fibrin degradation, thrombocytopenia → bleeding from every orifice, haematuria, haemorrhage into vital organs. Local necrosis is also characteristic of Russell's viper.
Diagnosis of coagulopathy: 20-minute whole blood clotting test (20WBCT) — place 2–3 mL of fresh venous blood in a clean glass tube; if blood fails to clot within 20 minutes, VICC is present and antivenom is indicated. Repeat every 6 hours.
Antivenom (Anti-Snake Venom, ASV): Polyvalent ASV covers all four Big Four species. Given IV (not IM — rapid absorption needed). Dose is by venom amount (not body weight) — typically 8–10 vials initially, repeated if the 20WBCT remains positive after 6 hours. Anaphylaxis risk: pre-treat with adrenaline 0.25 mg SC (prophylactic, though controversial) and have resuscitation ready.
Dog bite — rabies prophylaxis: Category II (minor scratches, no bleeding) — wound wash + anti-rabies vaccine (ARV); Category III (transdermal bites, contamination of mucous membranes) — wound wash + ARV + rabies immunoglobulin (RIG, infiltrated at the wound site).
Provided image
Clinical Decision-Making in Toxicological Emergencies
Clinical decision-making in toxicology requires integrating the rapidly gathered history, toxidrome recognition, and knowledge of antidote pharmacology to act quickly while avoiding the pitfalls of incorrect antidote use.
When antidotes help most — timing principles:
For paracetamol, starting NAC within 8–10 hours gives >90% hepatoprotection; after 24 hours, hepatic necrosis is established and NAC reduces severity but cannot prevent liver failure in severe cases. For naloxone, reversal of respiratory depression is the goal — give enough to restore ventilation, not to achieve full consciousness (in dependent patients, precipitating full withdrawal is painful and unsafe). For pralidoxime in organophosphate poisoning, efficacy depends critically on timing — the earlier, the better. There is a clinical window of hours before aging makes reactivation impossible; once a patient is 24–48 hours post-exposure (especially with dichlorvos or demeton), pralidoxime has little benefit.
Flumazenil pitfall — the most dangerous antidote misuse:
Flumazenil is paradoxically one of the most dangerous antidotes when used incorrectly. In the emergency setting, the patient's co-ingestions may be unknown. If a patient has co-ingested tricyclic antidepressants (TCAs) — a common suicide attempt pattern — benzodiazepine-mediated GABA-A activity may be the only thing preventing seizures from TCA sodium channel blockade. Removing this protection with flumazenil can precipitate status epilepticus. Rule: always consider TCA co-ingestion (suspect if QRS >100 ms on ECG) before using flumazenil.
Calling poison control: The National Poison Information Centre (NPIC) at AIIMS Delhi (1800-11-6117) provides 24-hour guidance on uncommon poisonings, antidote dosing, and management of rare exposures. Use it — toxicology is a specialty that most non-specialists underestimate in complexity.
Monitoring and discharge criteria: After paracetamol poisoning — monitor LFTs, INR, creatinine for 72–96 hours before discharge; patients with elevated LFTs require hepatology review. After opioid overdose on short-acting opioids — 4–6 hours observation after last naloxone dose. After organophosphate poisoning — hospitalise all patients for at least 24 hours; intermediate syndrome (weakness 24–96 hours post-exposure, from nicotinic junction failure) can emerge after apparent recovery and cause sudden respiratory arrest.
CLINICAL PEARL
Clinical Pearl: Atropine dosing in organophosphate poisoning — 'titrate to dry secretions, not to heart rate.' Many junior doctors stop atropine when the heart rate rises to 100–110 bpm, fearing tachycardia. This is wrong. In severe OP poisoning, atropine must be continued — and often large cumulative doses (50–100 mg or more over hours) are required — until the secretions (bronchial secretions, salivation) dry up. The endpoint is DRY secretions, not the heart rate. Nicotinic effects (tachycardia from ganglionic stimulation, fasciculations) are NOT reversed by atropine — only pralidoxime addresses those. Insufficient atropine dosing causes death from bronchorrhoea and respiratory failure.