Page 16 of 33
PH9.5 | PH9.5 | Antiseptics and Disinfectants — SDL Guide — SDL Guide
Learning Objectives
- Classify antiseptics and disinfectants by chemical group with examples and mechanisms
- Describe the spectrum of antimicrobial activity, clinical uses, precautions, and key limitations of each class
- Apply the Spaulding classification to select the appropriate level of decontamination for medical devices
- Identify important incompatibilities and safety precautions in antiseptic and disinfectant use
INSTRUCTIONS
Antiseptics and disinfectants are foundational to infection control, wound care, and sterilisation practice. Every clinician prescribes or recommends antiseptics for wound care, and every healthcare facility uses disinfectants for surface and instrument decontamination. Understanding which agent works for which purpose — and the critical precautions (concentration, contact time, incompatibilities, toxicity) — prevents healthcare-associated infections and avoids patient harm from incorrect use.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 55 (Antiseptics and Disinfectants) (textbook)
- Goodman & Gilman. The Pharmacological Basis of Therapeutics, 13th ed., Ch. 59 (Antiseptic Agents) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In the 1840s, Ignaz Semmelweis demonstrated that handwashing with chlorinated lime solution reduced the mortality from childbed (puerperal) fever in his Vienna obstetric ward from 10–18% to under 2% — before the germ theory was established. His colleagues rejected his findings. Thousands of women died unnecessarily before Lister's antiseptic surgical technique (carbolic acid spray) and Pasteur's germ theory finally established the scientific basis for what Semmelweis had proven empirically. Today, healthcare-associated infections (HAIs) remain a major patient safety crisis — and the pharmacological tools to prevent them (antiseptics for skin and wounds, disinfectants for instruments and surfaces) are among the most practically important drugs in clinical medicine.
WHY THIS MATTERS
Antiseptics and disinfectants are used in virtually every clinical encounter — from handwashing before a physical examination, to wound care in the emergency department, to endoscope reprocessing in the gastroenterology unit, to sterilisation of surgical instruments. In primary care settings, prescribing the correct antiseptic for a wound (and explaining how to use it) is a routine competency. Incorrect selection — applying a tissue-toxic disinfectant to a wound, or using a low-level disinfectant on a semi-critical instrument — causes either patient harm or inadequate infection prevention. PH9.5 operationalises infection control pharmacology for the everyday clinician.
RECALL
From Microbiology, recall the structural differences between gram-positive and gram-negative bacteria — gram-negative organisms have an outer membrane (lipopolysaccharide layer) that excludes many amphipathic molecules, making them inherently less susceptible to some detergent-type antiseptics (e.g. quaternary ammonium compounds). Recall also that bacterial endospores (Bacillus, Clostridium) are metabolically dormant structures with extreme resistance to heat, chemicals, and drying — no standard antiseptic kills spores except glutaraldehyde and certain oxidising agents under specific conditions. Recall the chain of infection: source → transmission route → susceptible host — antiseptics and disinfectants interrupt transmission at different points (hand antisepsis interrupts person-to-person transmission; instrument disinfection interrupts equipment-mediated transmission).
Infection Control: The Problem that Antiseptics Solve
Healthcare-associated infections (HAIs) — infections that patients acquire during the process of receiving healthcare — represent one of the most significant preventable causes of patient harm globally. The WHO estimates that at any given time, more than 1.4 million patients worldwide suffer from HAIs, with rates highest in low- and middle-income countries. In India, HAIs are responsible for prolonged hospital stays, increased antimicrobial resistance, and preventable deaths.
HAIs occur because healthcare environments concentrate potentially infected patients, invasive devices (catheters, endoscopes, surgical instruments), and immunocompromised hosts. The chain of infection — pathogen source → transmission (direct contact, droplet, airborne, vehicle) → susceptible host — is broken at the transmission step by proper antisepsis and disinfection. Handwashing/hand antisepsis is the single most effective intervention to reduce person-to-person HAI transmission. Instrument disinfection and sterilisation prevent device-mediated infections.
The historical milestone was Joseph Lister's introduction of carbolic acid (phenol) spray in the 1860s, which dramatically reduced post-operative sepsis mortality from approximately 45% to under 15%. This established the principle of antiseptic technique — using chemical agents on tissues and instruments to reduce the microbial burden before and during surgical procedures. Modern infection control builds on this principle with far safer and more targeted agents.
The key conceptual distinction for this module: antiseptic refers to an agent safe enough to apply to living tissue (skin, wounds, mucous membranes) to reduce microbial numbers. Disinfectant refers to an agent applied to inanimate surfaces and instruments; many disinfectants are too toxic for skin use at effective concentrations.
Therapeutic Goals and Principles
The therapeutic goals of antiseptics and disinfectants follow a hierarchy based on the required level of microbial reduction. Understanding this hierarchy — and knowing which agent achieves which level — is the foundation of rational infection control pharmacology.
Sterilisation: Complete elimination of ALL microbial life, including bacterial endospores. Required for critical items that enter sterile body tissues or the vascular system (surgical instruments, implants, injectable preparations). Physical methods (autoclaving at 121°C or 134°C under pressure; dry heat; ionising radiation) are preferred. Chemical sterilisation (glutaraldehyde 2% for 10 hours; ethylene oxide gas) is used for heat-sensitive instruments.
High-level disinfection: Kills all microorganisms EXCEPT some high-burden bacterial spores. Required for semi-critical items (endoscopes, laryngoscopes, respiratory therapy equipment) that contact mucous membranes but do not penetrate sterile tissue. Glutaraldehyde 2% (20–30 minute contact), ortho-phthalaldehyde (OPA), hydrogen peroxide (6–7.5%).
Low-level disinfection: Kills vegetative bacteria, some fungi, and lipid-envelope viruses; does NOT kill mycobacteria or spores reliably. Required for non-critical items (stethoscopes, blood pressure cuffs, bedside tables). Quaternary ammonium compounds, chlorhexidine solutions, some alcohol preparations.
Antisepsis: Reduction of microbial burden on living tissue sufficient to prevent infection. Antiseptics do not achieve sterilisation — they reduce the microbial load to a safe level. Concentration and contact time are critical: an agent used for less than its required contact time may fail to kill target organisms.
The Spaulding classification (developed by Earle Spaulding in 1968) provides the standard framework for selecting the level of decontamination by the risk category of the item: Critical (enters sterile tissue → sterilise), Semi-critical (contacts mucous membranes → high-level disinfection), Non-critical (contacts intact skin → low-level disinfection).
Classification of Antiseptics and Disinfectants
Antiseptics and disinfectants are classified by their chemical class, which largely determines their mechanism of action, spectrum of activity, and safe application. The classification below proceeds from the broad-spectrum, sporicidal agents to the more narrow-spectrum surface agents.
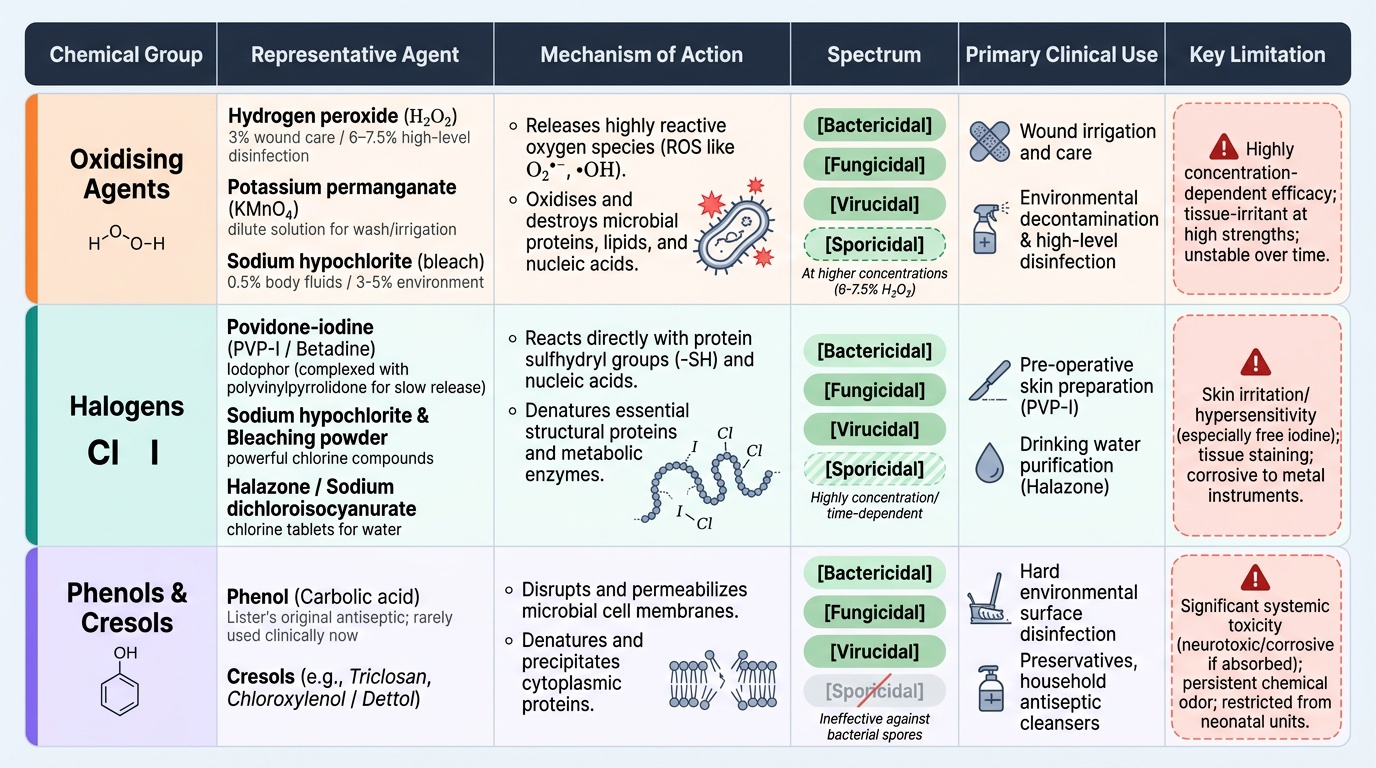
1. Oxidising agents: Release reactive oxygen species (ROS — superoxide radicals, hydroxyl radicals) that oxidise and destroy microbial proteins, lipids, and nucleic acids. Non-selective, concentration-dependent activity. Examples: hydrogen peroxide (H₂O₂, 3% wound care; 6–7.5% high-level disinfection), potassium permanganate (KMnO₄, dilute solution for wound irrigation), sodium hypochlorite (bleach — 0.5% for body fluid spill decontamination; household 3–5% for environmental disinfection).
2. Halogens: React with protein sulfhydryl groups and nucleic acids. Iodine — either as Lugol's iodine or povidone-iodine (PVP-I, Betadine) — is the most widely used. Povidone-iodine is an iodophore (iodine complexed with polyvinylpyrrolidone carrier) that provides sustained slow release of free iodine — better tolerated, less irritant than Lugol's. Broad spectrum: gram+, gram-, mycobacteria, fungi, viruses, spores at higher concentrations. Chlorine compounds (sodium hypochlorite, bleaching powder) are powerful surface disinfectants; chlorine tablet (Halzone, Sodium dichloroisocyanurate) for water purification.
3. Phenols and cresols: Act by disrupting cell membranes and denaturing cytoplasmic proteins. Phenol (carbolic acid) — Lister's original antiseptic — is now rarely used clinically due to toxicity. Cresol (Lysol, a mixture of cresols in soap solution) — used for instrument disinfection and environmental disinfection, particularly effective against non-spore-forming bacteria including mycobacteria. Chloroxylenol (Dettol) — halogenated phenol; widely used as a household antiseptic and for wound care; broad spectrum against gram+ and gram- bacteria; incompatible with hard water (forms inactive complexes — always dilute in soft or distilled water).
4. Alcohols: Denature proteins by disrupting hydrogen bonds and dehydrating the bacterial cytoplasm; also dissolve lipid envelope of viruses. Ethanol 70% — the most widely used alcohol antiseptic and handrub. Optimal concentration is 70% — NOT 100% (absolute alcohol is less effective because some water is needed for protein denaturation; concentrated alcohol also evaporates too quickly for effective contact). Isopropanol 70–90% — slightly more effective than ethanol for some organisms; common in hand sanitisers. NOT sporicidal.
5. Biguanides: Disrupt cell membranes. Chlorhexidine — the most important biguanide. Bactericidal against gram-positive and gram-negative organisms, effective against Candida, active against some enveloped viruses. Not sporicidal. Persists on skin (residual activity — important for surgical hand scrub). 4% solution (Hibiscrub) for surgical hand preparation. 0.05–0.5% for wound antisepsis. 0.12–0.2% as oral rinse for gingivitis. Resistant organisms: Pseudomonas aeruginosa (some strains) and non-enveloped viruses.
6. Aldehydes: Cross-link proteins and nucleic acids, killing all microbial forms. Glutaraldehyde 2% alkaline solution (Cidex) — the gold standard chemical agent for high-level disinfection and (with long contact) sterilisation of heat-sensitive instruments (flexible endoscopes, bronchoscopes). Contact 20–30 min = high-level disinfection; 10 hours = sterilisation. Toxic to tissue — never an antiseptic. Formaldehyde (HCHO) — used for tissue fixation (formalin), fumigation, sterilisation of pharmaceutical equipment. Carcinogenic (IARC Group 1); use declining in favour of glutaraldehyde and newer agents.
7. Quaternary ammonium compounds (QACs): Cationic detergents that disrupt cell membranes. Benzalkonium chloride (BZK) — low-level disinfectant for non-critical surfaces; NOT effective against Pseudomonas aeruginosa, mycobacteria, or spores; incompatible with soap/anionic detergents (which neutralise their positive charge). Cetrimide — used for wound care at dilute concentrations. Pseudomonas is famously resistant to QACs and can even grow in contaminated QAC solutions — a hospital infection control hazard.
Provided image
SELF-CHECK
A flexible colonoscope needs to be reprocessed after use. Using the Spaulding classification, what level of decontamination is required, and which agent is most appropriate?
A. Low-level disinfection — benzalkonium chloride solution for 5 minutes is sufficient
B. High-level disinfection — glutaraldehyde 2% for 20–30 minutes, as the colonoscope contacts mucous membranes (semi-critical item)
C. Autoclave sterilisation at 121°C — endoscopes must be completely sterilised after every use
D. Ethanol 70% wipe — alcohol effectively kills all organisms relevant to GI endoscopy
Reveal Answer
Answer: B. High-level disinfection — glutaraldehyde 2% for 20–30 minutes, as the colonoscope contacts mucous membranes (semi-critical item)
A colonoscope contacts the mucous membrane of the colon — it is a semi-critical item in the Spaulding classification. Semi-critical items require high-level disinfection: killing all microorganisms except resistant bacterial spores. Glutaraldehyde 2% (alkaline, e.g. Cidex) for a minimum contact time of 20–30 minutes is the standard chemical agent for flexible endoscope high-level disinfection. Autoclaving at high temperatures would destroy flexible endoscopes. Benzalkonium chloride provides only low-level disinfection and cannot kill mycobacteria or some gram-negative bacteria. Ethanol wipes provide surface disinfection but are not appropriate for luminal endoscope reprocessing.