Page 17 of 33
PH9.5 | PH9.5 | Antiseptics and Disinfectants — SDL Guide — SDL Guide (Part 2)
Per-Class Pharmacology, Uses and Precautions
The practical use of antiseptics and disinfectants depends on knowing the specific properties, precautions, and limitations of each class — errors in concentration, contact time, or compatibility can render agents ineffective or cause tissue damage.
Hydrogen peroxide (H₂O₂):
3% solution is used for wound cleaning and debridement — the release of oxygen bubbles (from catalase in tissue) mechanically dislodges debris and necrotic tissue, and the reactive oxygen species have antimicrobial activity. Note: hydrogen peroxide at 3% does not penetrate biofilms well and may damage granulation tissue if used repeatedly; it is primarily a wound-cleaning agent, not for chronic wound management where it can delay healing. Higher concentrations (6–7.5%) are used as high-level disinfectants.
Povidone-iodine:
Broad spectrum; recommended for wound antisepsis, preoperative skin preparation, and oral care (dilute gargle). Key precaution: avoid on large open wounds or burns because systemic iodine absorption can cause hypothyroidism (iodine toxicity) or metabolic acidosis. Not for use in neonates. Dilute solutions (0.5–1%) are more effective than concentrated (10%) because high concentration reduces the release of free iodine. Discolours skin and linen.
Chlorhexidine:
Unlike most antiseptics, chlorhexidine has residual (substantive) activity — it binds to keratin in skin and remains active for hours after application, providing prolonged antibacterial effect. This is the reason it is superior to povidone-iodine for surgical hand preparation and preoperative skin antisepsis in multiple RCTs (Darouiche 2010 NEJM: chlorhexidine-alcohol significantly reduced surgical site infections vs povidone-iodine in clean-contaminated surgery). Ototoxic — never instil into the middle ear. Avoid contact with eyes and brain.
Ethanol (70%) and isopropanol:
Rapidly effective; evaporates quickly (no residual activity); excellent for hand rubbing (WHO ABHR — alcohol-based hand rub). Not sporicidal — cannot kill Clostridioides difficile spores (C. diff). Therefore alcohol hand rubs must be supplemented with soap-and-water handwashing when C. diff is suspected (mechanical removal of spores, as soap does not kill them). Flammable — store and use away from open flames.
Glutaraldehyde (2% Cidex):
Most powerful chemical disinfectant/sterilant. Must be freshly prepared or within its stated use-life. Highly irritating to mucous membranes and skin — healthcare workers handling it must use gloves, eye protection, and well-ventilated areas. Can cause occupational asthma and contact dermatitis. Instruments must be rinsed thoroughly with sterile water after glutaraldehyde treatment before use (residual glutaraldehyde on endoscopes causes mucosal injury). Shelf life of activated solution ~14–28 days (depending on formulation).
Quaternary ammonium compounds (QACs):
Inactivated by organic matter (blood, pus) and soap — must clean surfaces with soap/water BEFORE applying QAC. Pseudomonas aeruginosa is notably resistant and can colonise QAC solutions — a hospital outbreak risk if QAC containers are not replaced frequently. Effective for environmental surface disinfection (floors, equipment) but not for medical instruments or wounds.
SELF-CHECK
A nurse uses an alcohol-based hand rub before entering the room of a patient with confirmed Clostridioides difficile infection. What is the critical limitation of this approach?
A. Alcohol-based hand rubs are not effective against any gram-positive bacteria
B. Alcohol is not sporicidal — it cannot kill C. difficile spores; soap-and-water handwashing is required to mechanically remove spores
C. Chlorhexidine-alcohol is required in place of ethanol for C. difficile
D. The nurse should use glutaraldehyde hand scrub instead of alcohol
Reveal Answer
Answer: B. Alcohol is not sporicidal — it cannot kill C. difficile spores; soap-and-water handwashing is required to mechanically remove spores
Alcohol-based hand rubs (ABHR) are highly effective against vegetative bacteria, fungi, and most viruses, but are NOT sporicidal. Clostridioides difficile produces highly resistant endospores that survive alcohol exposure. For C. diff contact precautions, soap-and-water handwashing is mandatory because the mechanical friction of handwashing physically removes spores from the skin surface — even though soap itself does not kill spores. This is a critical and clinically important exception to the general superiority of ABHR for hand hygiene.
Clinical Decision-Making: Selecting the Right Agent
Selecting the correct antiseptic or disinfectant requires answering three questions: (1) Is this being applied to living tissue or an inanimate surface? (2) What is the Spaulding category of the item being decontaminated? (3) What organisms need to be killed?
Preoperative skin antisepsis: Chlorhexidine-alcohol (e.g. 2% chlorhexidine in 70% isopropanol) is the preferred preoperative skin preparation agent based on RCT evidence — superior to povidone-iodine-alcohol for surgical site infection prevention. Allow full contact time (2–3 minutes); allow to dry completely before draping (fire risk from alcohol if diathermy used before drying).
Wound care antisepsis: Povidone-iodine 10% (or 0.5–1% for dilute use) for acute contaminated wounds; chlorhexidine 0.05–0.1% for clean wounds. Avoid hydrogen peroxide on chronic wounds where it impairs healing. Avoid concentrations that are tissue-toxic — the common error is using undiluted antiseptics that damage healing tissue.
Endoscope reprocessing: Flexible endoscopes: glutaraldehyde 2% high-level disinfection (20–30 min); rigid heat-tolerant endoscopes: autoclave preferred. All endoscopes must be pre-cleaned (enzymatic detergent) to remove organic matter before disinfection — organic matter inactivates both glutaraldehyde and QACs.
Hand hygiene: ABHR (ethanol 70% or isopropanol 70–80%) for routine clinical hand hygiene — faster, better tolerated, more effective than soap for most organisms. Soap-and-water for visibly soiled hands, after toileting, and for C. diff contact precautions.
Environmental surface disinfection: 0.5% sodium hypochlorite (approximately 1000 ppm available chlorine) for most clinical surfaces; 1% (10,000 ppm) for blood/body fluid spills and C. diff contaminated environments (to kill spores). QACs can be used for general non-critical environmental surfaces but are insufficient for TB or spore-forming organism decontamination.
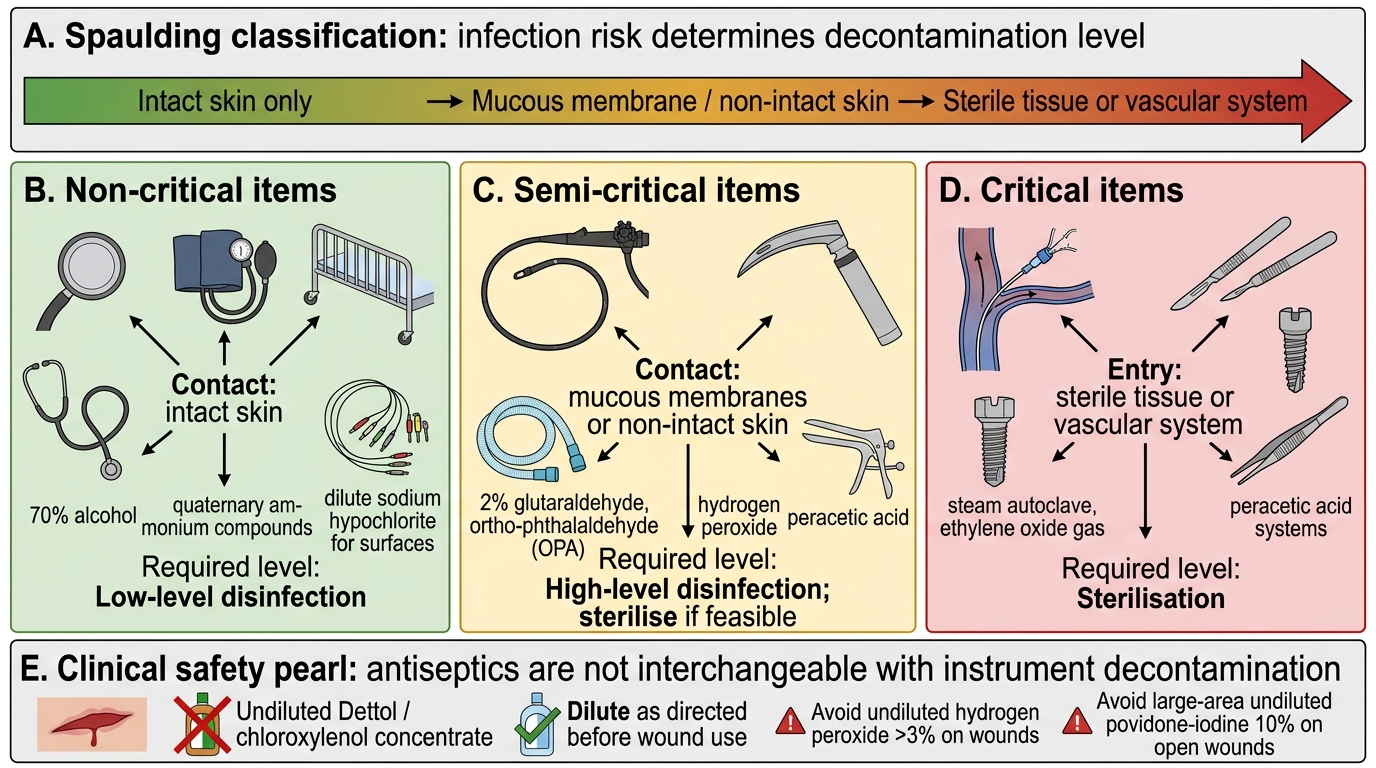
Spaulding Classification of Medical Devices
CLINICAL PEARL
Clinical Pearl: Never put undiluted Dettol (chloroxylenol) on a wound. Dettol is supplied as a concentrated solution (approx. 4.8% chloroxylenol) intended to be diluted 1:20 for wound care. Undiluted Dettol is tissue-toxic — it causes chemical burns to the wound bed and impairs healing. This is one of the most common antiseptic misuse errors in primary care settings. Advise patients explicitly: always dilute Dettol as directed on the label (1 teaspoon in 600 mL water) before applying to wounds. Similarly, undiluted hydrogen peroxide above 3% and undiluted povidone-iodine 10% on large open wounds can cause systemic toxicity and impaired healing.
Self-Assessment
Test your understanding of antiseptic and disinfectant pharmacology.
- Apply the Spaulding classification to categorise: (a) a stethoscope, (b) a flexible colonoscope, (c) a vascular catheter, (d) a blood pressure cuff. State the required level of decontamination for each.
- Which antiseptic has residual (substantive) activity on skin, and why is this important for preoperative skin preparation?
- Why is alcohol-based hand rub ineffective against Clostridioides difficile, and what should be used instead?
- A healthcare worker soaks endoscopes in glutaraldehyde 2% for 10 minutes and then uses them. What is the risk, and what is the correct contact time for high-level disinfection?
- Name two important incompatibilities of quaternary ammonium compounds (QACs) that can render them ineffective in clinical practice.
SELF-CHECK
Which statement about ethanol as an antiseptic is correct?
A. 100% (absolute) ethanol is the most effective concentration because it is the purest form
B. Ethanol 70% is sporicidal and can replace glutaraldehyde for high-level disinfection
C. Ethanol 70% is more effective than absolute alcohol because some water is needed for protein denaturation; it is not sporicidal
D. Ethanol must be mixed with chlorhexidine to have any bactericidal activity
Reveal Answer
Answer: C. Ethanol 70% is more effective than absolute alcohol because some water is needed for protein denaturation; it is not sporicidal
Ethanol 70% is the optimal bactericidal concentration — absolute (100%) ethanol is actually less effective because it evaporates too quickly and lacks the water needed for effective protein denaturation of the microbial cell. The mechanism requires contact between alcohol-water mixtures and microbial proteins; anhydrous alcohol coagulates a surface protein shell on the bacterium that reduces penetration. Ethanol is NOT sporicidal — it cannot kill bacterial endospores, and does not provide high-level disinfection. It does not require chlorhexidine to have activity, though chlorhexidine-alcohol combinations provide both immediate and residual (prolonged) antimicrobial action.