Page 19 of 33
PH9.6 | PH9.6 | Dermatological Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Describe the mechanism of action, uses, and adverse effects of drugs used in acne vulgaris (topical and oral)
- Outline the pharmacotherapy of scabies and pediculosis with first-line and second-line options
- Describe topical and systemic treatment options for psoriasis in a step-up approach
- Apply knowledge of sunscreen science (SPF, UV spectrum) to patient counselling
INSTRUCTIONS
Skin disorders are among the most common conditions in Indian clinical practice — acne affects 80–90% of adolescents, scabies is endemic in crowded communities, and psoriasis affects approximately 2% of the population. Understanding dermatological pharmacotherapy from first principles — which drugs target which mechanisms, and the critical safety issues (isotretinoin teratogenicity, methotrexate weekly dosing) — is essential for safe prescribing in general practice and dermatology.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 64 (Dermatological Pharmacology) (textbook)
- Goodman & Gilman. The Pharmacological Basis of Therapeutics, 13th ed., Ch. 65 (Dermatological Pharmacology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 18-year-old engineering student presents to your outpatient clinic in tears. She has had severe nodular acne for two years — painful, deep cysts on her cheeks and jaw — leaving permanent scarring despite two courses of oral doxycycline and three months of combined topical tretinoin and benzoyl peroxide. Her self-confidence has deteriorated. You consider oral isotretinoin. She asks: 'Will it cure my acne?' The answer: yes, in approximately 85% of cases after a single course — isotretinoin is the only drug that can induce prolonged remission in severe nodular acne. But it is also Pregnancy Category X — a single dose during early pregnancy causes severe foetal malformations in >25% of exposed foetuses. Understanding both its extraordinary efficacy and its mandatory safety programme is what separates safe prescribing from dangerous practice.
WHY THIS MATTERS
Dermatological pharmacotherapy is directly relevant across primary care, general practice, paediatrics, and general medicine. Scabies and pediculosis are endemic in rural India and require correct first-line treatment (permethrin) and simultaneous household treatment to prevent reinfection. Acne management involves a stepwise escalation from topical agents to oral antibiotics to isotretinoin, with precise monitoring required for the latter. Psoriasis, though non-infectious, causes profound quality-of-life impairment and can require systemic immunomodulation (methotrexate, ciclosporin) or expensive biologics for moderate-severe disease. Sunscreen counselling is relevant to skin cancer prevention in a high UV-exposure country like India. PH9.6 encompasses all of these.
RECALL
From earlier pharmacology modules, recall that retinoids are vitamin A derivatives. All-trans-retinoic acid (tretinoin) and 13-cis-retinoic acid (isotretinoin) act on nuclear retinoic acid receptors (RARs) to regulate gene expression. From immunology (PY), recall that psoriasis is a T-cell mediated inflammatory skin disease — activated T-helper 17 (Th17) cells release IL-17 and IL-23 drives Th17 differentiation; these cytokines drive keratinocyte hyperproliferation (turnover every 3–5 days in psoriasis vs normal 28 days). From the autonomic pharmacology cluster, recall that androgens (testosterone, DHT) stimulate sebaceous gland growth and sebum production — which is why hormonal manipulation (anti-androgens like cyproterone acetate) can be useful in female acne with androgen excess.
Pathophysiology of Common Skin Disorders
Understanding the pathophysiology of each skin disorder is essential for rational drug selection — each therapeutic agent targets a specific step in the pathological process.
Provided image
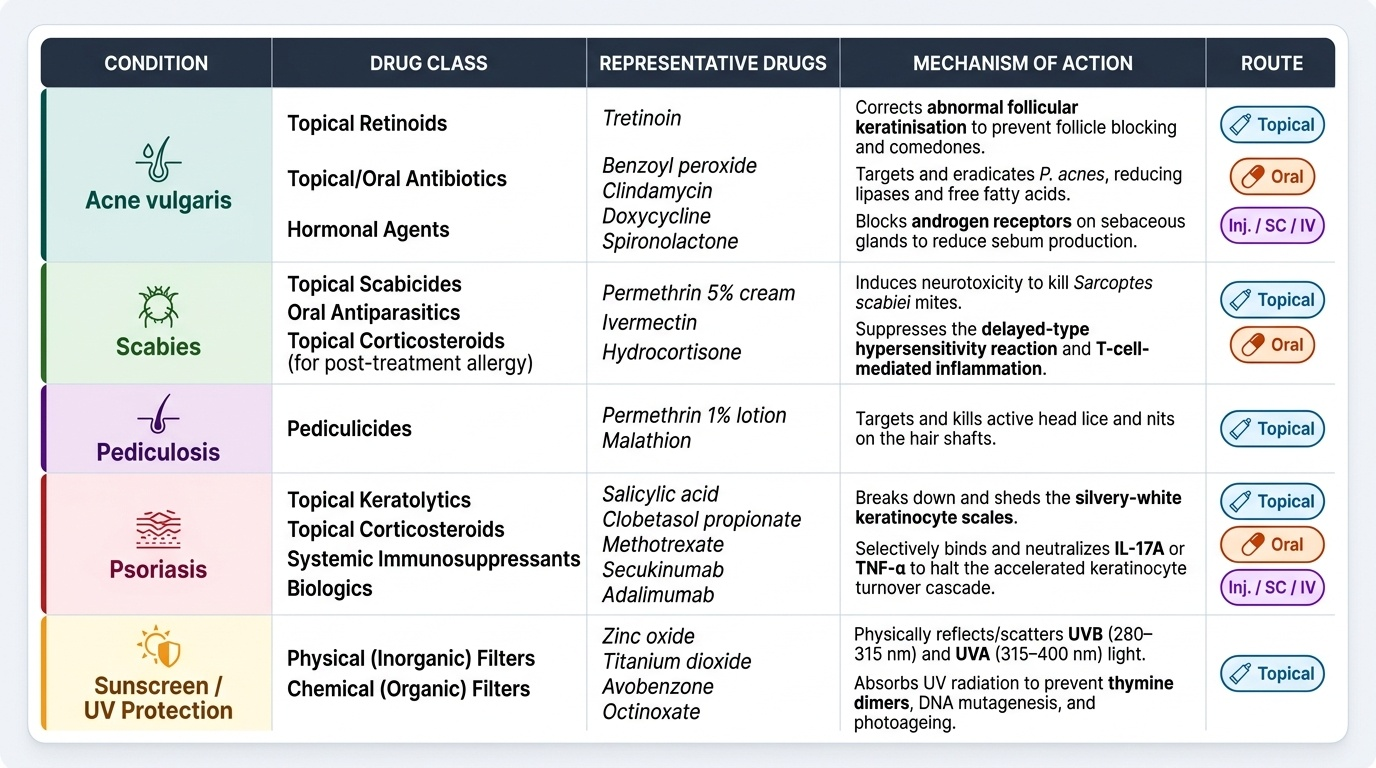
Acne vulgaris: The primary pathogenic event is abnormal follicular keratinisation — excess keratin blocks the pilosebaceous follicle, trapping sebum and creating an anaerobic environment. The gram-positive anaerobe Propionibacterium acnes (Cutibacterium acnes) colonises this sebum-rich environment, producing lipases that break down sebum triglycerides into free fatty acids — potent pro-inflammatory stimuli. Androgens amplify the process by stimulating sebaceous gland activity. The result: comedones (non-inflammatory plugged follicles — open = blackhead, closed = whitehead) progressing to inflammatory papules, pustules, and nodules (cysts).
Scabies: Caused by the mite Sarcoptes scabiei var. hominis, which burrows into the stratum corneum, lays eggs, and triggers a delayed-type hypersensitivity reaction. The intense nocturnal pruritus is immune-mediated (allergic), not from the mite itself — this is why symptoms persist for 2–4 weeks after successful treatment (the immune reaction continues until mite antigens are cleared). Transmission: direct prolonged skin contact.
Pediculosis (head lice): Caused by Pediculus humanus capitis (head louse). The louse bites the scalp, causing pruritus and secondary bacterial infection from scratching. Nits (eggs) are cemented to hair shafts. Transmission: direct head-to-head contact.
Psoriasis: A T-cell-mediated autoimmune inflammatory disease characterised by dramatically accelerated keratinocyte turnover (3–5 days vs normal 28 days). Th17 cells infiltrate the dermis and secrete IL-17A, IL-17F, and TNF-α, which activate keratinocytes to proliferate and produce chemokines that further amplify the inflammatory cascade. Clinically: well-demarcated, erythematous plaques with silvery-white scales, Auspitz sign (pinpoint bleeding on scale removal), and involvement at extensor surfaces (elbows, knees), scalp, and sacrum.
UV radiation and skin damage: Solar UV radiation reaches the skin in two components: UVB (280–315 nm) — absorbed by DNA in keratinocytes → thymine dimers → mutagenesis, sunburn, skin cancer; UVA (315–400 nm) — deeper penetration, less erythema per dose but causes photoageing and contributes to melanoma. Sunscreens prevent both types of damage.
Therapeutic Goals in Dermatological Pharmacotherapy
The therapeutic goals differ by condition, which guides both drug selection and the route of administration (topical vs systemic) and the formulation vehicle.
Acne: Goals are to: (1) normalise follicular keratinisation (retinoids), (2) reduce sebum production (isotretinoin, hormonal therapy), (3) kill or reduce P. acnes colonisation (benzoyl peroxide, topical and oral antibiotics), and (4) reduce inflammation (all of the above, plus anti-inflammatory retinoids). The step-up approach prioritises topical therapy for mild disease and escalates to systemic agents (oral antibiotics, isotretinoin) for moderate-severe disease.
Scabies and pediculosis: Goal is to kill the parasite (scabicidal, pediculicidal). The entire household and close contacts must be treated simultaneously to prevent reinfection — treating only the index case is one of the most common reasons for treatment failure.
Psoriasis: Goal is to reduce keratinocyte hyperproliferation and the underlying T-cell-mediated inflammation. For mild localised plaque psoriasis, topical agents (corticosteroids, vitamin D analogues, coal tar) suffice. For moderate-severe psoriasis (>10% body surface area, or involvement of face/genitals/hands/nails, or functional impairment), systemic therapy is required.
Sunscreens: Goal is primary prevention of UV-induced DNA damage, sunburn, photoageing, and skin cancer. SPF (Sun Protection Factor) measures protection against UVB only — it does not quantify UVA protection. A 'broad spectrum' label indicates both UVA and UVB protection. SPF 30 blocks approximately 97% of UVB; SPF 50 blocks approximately 98% — the incremental difference diminishes above SPF 30.
Vehicle selection: The pharmaceutical vehicle determines both efficacy and patient adherence. Ointments (water-in-oil) — most occlusive, highest drug penetration, ideal for hyperkeratotic, dry, or thick-skinned areas (palms, soles, scalp psoriasis); Creams (oil-in-water) — cosmetically acceptable, less occlusive, suitable for most skin conditions; Gels — alcohol-based, good for oily/hairy areas (acne on face, scalp seborrhoeic dermatitis); Lotions — lowest viscosity, for large hairy areas. Wrong vehicle impairs drug delivery and reduces patient compliance.
Classification of Dermatological Drugs
Provided image
Dermatological drugs for the conditions in PH9.6 span several pharmacological classes. The classification below groups them by condition and mechanism.
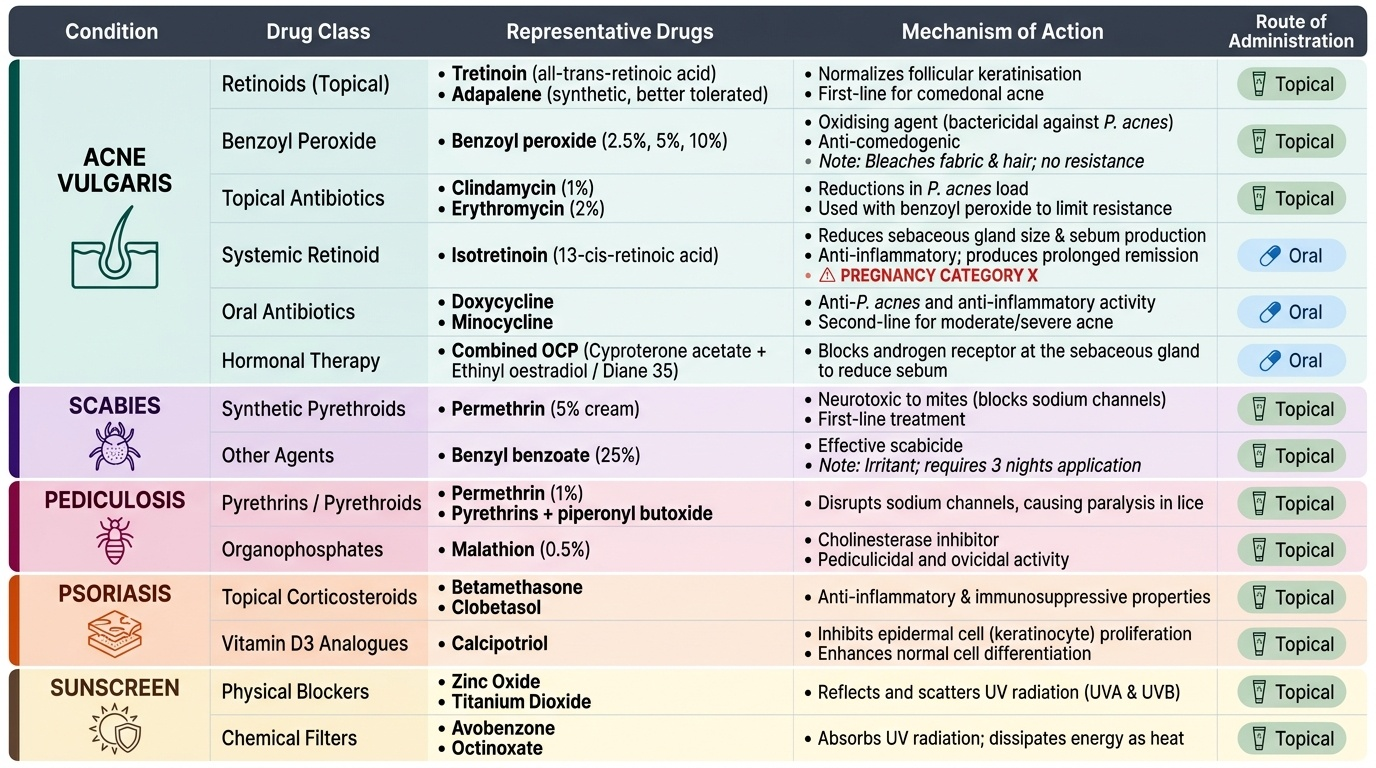
For acne vulgaris:
- Retinoids (topical): tretinoin (all-trans-retinoic acid), adapalene (synthetic retinoid — better tolerated than tretinoin) — normalise follicular keratinisation; first-line for comedonal acne
- Benzoyl peroxide: oxidising agent — bactericidal against P. acnes; anti-comedogenic; available 2.5%, 5%, 10%; bleaches fabric and hair; does NOT promote antibiotic resistance
- Topical antibiotics: clindamycin 1%, erythromycin 2% — reduce P. acnes; used in combination with benzoyl peroxide (to reduce resistance emergence)
- Oral isotretinoin: systemic retinoid (13-cis-retinoic acid) — reduces sebaceous gland size and sebum production; normalises follicular keratinisation; anti-inflammatory; the only drug producing prolonged remission; PREGNANCY CATEGORY X
- Oral antibiotics: doxycycline, minocycline (tetracyclines) — anti-P. acnes and anti-inflammatory; 2nd-line for moderate acne or topical therapy failures
- Hormonal therapy (females): combined OCP with anti-androgenic progestin (cyproterone acetate + ethinyl oestradiol — Diane 35) — reduces sebum by blocking androgen receptor at the sebaceous gland
For scabies:
- Permethrin 5% cream: synthetic pyrethroid — first-line
- Benzyl benzoate 25%: older agent; effective but irritant; 3 nights application in adults, 3 nights with dilution in children
- Ivermectin (oral): second-line, for crusted scabies or when topical therapy fails
For pediculosis:
- Permethrin 1% lotion (creme rinse): first-line for head lice
- Malathion 0.5% lotion: second-line; organophosphate insecticide; effective against nits and lice
- Ivermectin oral: for resistant pediculosis
For psoriasis:
- Topical corticosteroids: first-line for mild-moderate localised psoriasis; potency classes I–IV; risk of skin atrophy and tachyphylaxis with prolonged use
- Calcipotriol (calcipotriene): synthetic vitamin D3 analogue; normalises keratinocyte proliferation; no skin atrophy; used in combination with topical corticosteroids for additive effect
- Coal tar: reduces epidermal proliferation; messy but effective for scalp and body plaques; some carcinogenicity concern (polycyclic aromatic hydrocarbons)
- Dithranol (anthralin): reduces keratinocyte DNA synthesis; stains skin/clothing; used as short-contact therapy
- Systemic — methotrexate: antifolate; weekly low dose (7.5–25 mg once weekly); folic acid supplementation reduces mucositis ADRs
- Systemic — ciclosporin: calcineurin inhibitor; rapid onset; nephrotoxic with long-term use
- Systemic — acitretin: oral retinoid; teratogenic; slow onset
- Biologics: anti-TNF-α (infliximab, adalimumab, etanercept), anti-IL-17 (secukinumab, ixekizumab), anti-IL-23 (guselkumab, risankizumab) — for moderate-severe, refractory psoriasis
Sunscreens:
- Chemical filters: oxybenzone, avobenzone, octocrylene — absorb UV and release energy as heat; broad spectrum (UVA + UVB)
- Physical blockers: zinc oxide, titanium dioxide — inorganic particles that reflect and scatter UV; broad spectrum, photostable, preferred in sensitive skin and infants
SELF-CHECK
A 17-year-old boy presents with moderate inflammatory acne (papulopustular, no cysts). He has tried benzoyl peroxide 5% for 3 months with partial response. What is the most appropriate next step in management?
A. Start oral isotretinoin immediately — moderate acne always requires systemic retinoid therapy
B. Add topical tretinoin to the benzoyl peroxide regimen, and consider adding topical clindamycin if the benzoyl peroxide-tretinoin combination is insufficient
C. Start oral doxycycline alone and stop topical therapy to simplify the regimen
D. Start a topical corticosteroid cream to reduce the inflammation
Reveal Answer
Answer: B. Add topical tretinoin to the benzoyl peroxide regimen, and consider adding topical clindamycin if the benzoyl peroxide-tretinoin combination is insufficient
For moderate acne not responding adequately to benzoyl peroxide monotherapy, the step-up approach adds a topical retinoid (tretinoin or adapalene) and potentially a topical antibiotic (clindamycin) — always combined with benzoyl peroxide to prevent antibiotic resistance. Oral isotretinoin is reserved for severe nodular/cystic acne that has failed multiple treatment lines — it should not be the second step for moderate acne. Topical corticosteroids are not used for acne and can actually worsen it by promoting comedone formation.