Page 20 of 33
PH9.6 | PH9.6 | Dermatological Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Acne Vulgaris: Drug Classes and Management
Each acne drug acts on a specific pathogenic step — understanding this enables rational combination therapy and appropriate escalation.
Topical retinoids (tretinoin, adapalene):
Tretinoin (all-trans-retinoic acid) normalises follicular keratinisation by binding retinoic acid receptors (RARs) in keratinocytes, reducing abnormal corneocyte cohesion that causes follicular plugging. It also has anti-inflammatory effects. ADRs: dryness, peeling, photosensitivity (use at night; always use sunscreen). Adapalene is a synthetic retinoid with a similar mechanism but better tolerated (less irritant), making it preferred for first-time retinoid users and patients with sensitive skin.
Benzoyl peroxide (BPO):
BPO releases free oxygen radicals that are directly lethal to P. acnes. It is keratolytic (reduces comedones) and has anti-inflammatory effects. Critical advantage over antibiotics: it does NOT promote antibiotic resistance in P. acnes. BPO should always be used alongside topical antibiotics to prevent resistance emergence. ADRs: dryness, bleaching of clothing and pillowcases (warn patients). Available in multiple concentrations (2.5%–10%) — higher concentration is more drying but not more effective, so 2.5–5% is preferred.
Topical antibiotics (clindamycin 1%, erythromycin 2%):
Reduce P. acnes colonisation and have intrinsic anti-inflammatory effects. Growing resistance to clindamycin in P. acnes is a concern — always combine with benzoyl peroxide (the combination is synergistic and reduces resistance emergence). Do NOT use topical antibiotics as monotherapy.
Oral isotretinoin:
Isotretinoin is the most powerful acne therapy available, inducing prolonged remission (often permanent) in >80% of patients with severe nodular acne after a single course. It reduces sebaceous gland size and sebum production by ~90% (via RAR-β-mediated reduction in sebocyte differentiation), normalises follicular keratinisation, and inhibits P. acnes. Dose: typically 0.5–1 mg/kg/day for 15–20 weeks. Side effects: cheilitis (lip dryness — near-universal), skin dryness and photosensitivity, elevated triglycerides and LFTs (monitor monthly), myalgia, night blindness, depression (controversial association; monitor carefully). Teratogenicity — MANDATORY SAFETY: Isotretinoin is Pregnancy Category X — single therapeutic doses cause major foetal malformations (CNS, cardiac, facial) in >25% of exposed foetuses. All female patients of childbearing age MUST have: a negative pregnancy test before starting, two reliable forms of contraception throughout treatment and for 1 month after stopping, and monthly pregnancy tests during treatment.
Oral antibiotics (doxycycline, minocycline):
For moderate acne with inflammatory component not controlled by topical therapy alone. Doxycycline 100 mg once daily; minocycline 100 mg once daily. ADRs: doxycycline — photosensitivity (counsel to use sunscreen), oesophageal ulceration (take with a full glass of water, do not lie down for 30 min); minocycline — vestibular side effects (vertigo, dizziness), drug-induced lupus. Duration: typically 3–6 months; always combine with topical BPO to limit resistance. Avoid in pregnancy and children under 8 years (tooth staining).
Hormonal therapy:
For females with hormonally-driven acne (worse pre-menstrually, chin/jaw distribution, elevated androgens or PCOS). The combined OCP containing cyproterone acetate (anti-androgen progestin) + ethinyl oestradiol (e.g. Diane-35) reduces sebum production by blocking androgen receptor at the sebaceous gland. Effective in 3–6 months. Contraindicated in smokers over 35, personal or family history of thromboembolic disease.
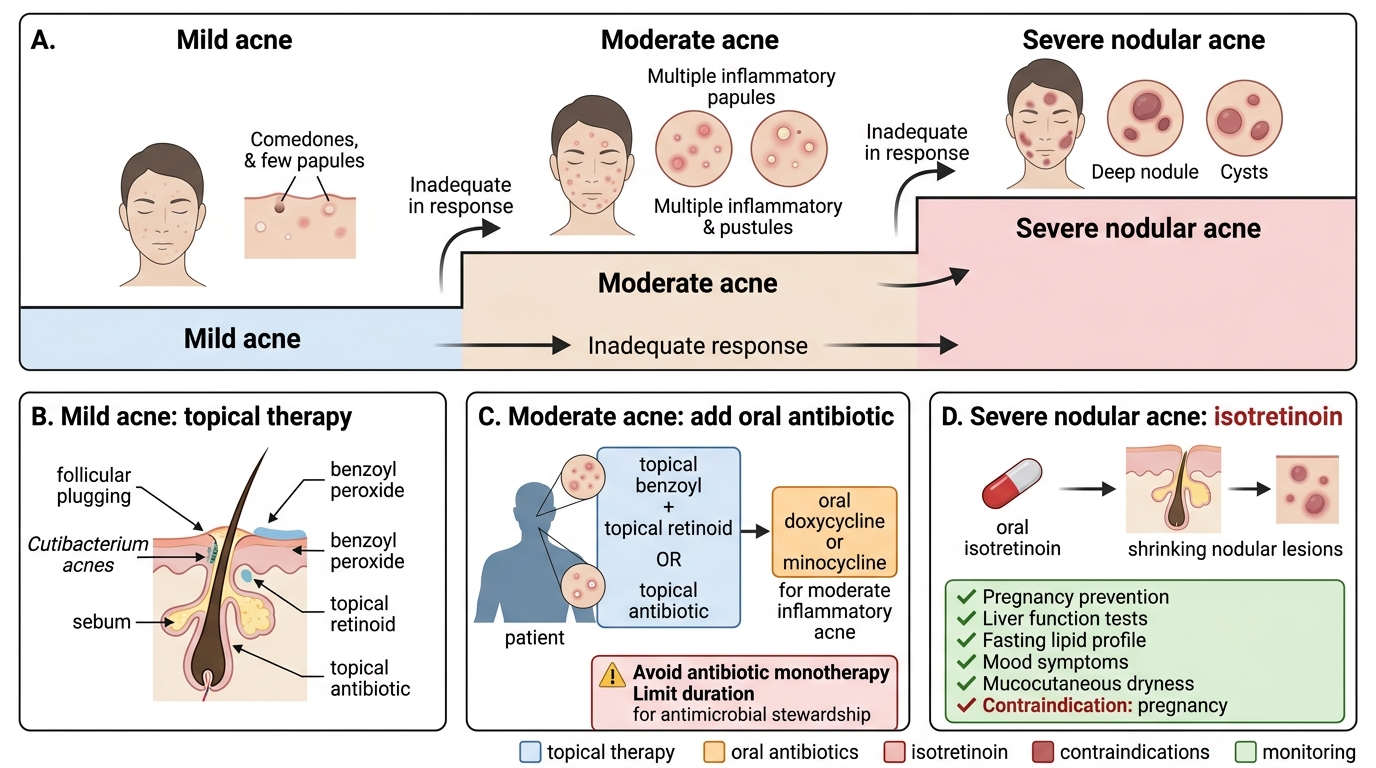
Stepwise Pharmacological Management of Acne Vulgaris
Scabies, Pediculosis, and Psoriasis: Drug Classes and Management
Scabies, pediculosis, and psoriasis each require distinct pharmacological approaches tailored to their pathophysiology.
Scabies pharmacotherapy:
Permethrin 5% cream is the first-line treatment for scabies worldwide. Permethrin is a synthetic pyrethroid that prolongs the opening of voltage-gated sodium channels in the mite's nervous system, causing prolonged depolarisation and paralysis followed by death — the same mechanism as natural pyrethrins but more stable and more potent. Application: applied from the neck downward to all skin surfaces (including webspaces, genitalia, under fingernails) at night; washed off after 8–14 hours; repeat application after one week. Simultaneously treat ALL household members and sexual contacts, and wash all clothing/bedding in hot water.
Benzyl benzoate 25% is an older alternative; effective but more irritant. Applied for 3 consecutive nights; repeat after 1 week. Dilute for use in children (12.5%) and infants (6.25%).
Ivermectin (oral) is used for crusted (Norwegian) scabies (where the mite load is massive), in immunocompromised patients, and when topical therapy fails. Dose: 200 mcg/kg single dose, repeat after 2 weeks. Ivermectin is an antiparasitic that binds glutamate-gated chloride channels in invertebrates (paralysis). It does not cross the blood-brain barrier in normal mammals (P-glycoprotein barrier) — but patients with CNS P-gp deficiency (collie dogs — classic example; human equivalent: MDR1 mutation) are at risk of CNS toxicity.
Pediculosis pharmacotherapy:
Permethrin 1% lotion (creme rinse) is first-line for head lice. Applied to wet hair, left for 10 minutes, rinsed out; repeat after 7–10 days (to kill newly hatched nymphs from eggs not killed by the first application). The 1% concentration is pediculicidal but only weakly ovicidal — hence the two-application schedule. Malathion 0.5% lotion is a second-line organophosphate insecticide that is both pediculicidal and ovicidal — single application may suffice. Physical removal with a fine-tooth nit comb is an important adjunct. Wet-combing (applying conditioner) facilitates nit removal.
Psoriasis pharmacotherapy:
Treatment is stepped by severity. Mild psoriasis (<5–10% BSA, non-disabling) starts with topical therapy:
- Topical corticosteroids: most widely used first-line; reduce inflammation rapidly; risk of skin atrophy, striae, and tachyphylaxis (reduced response) with prolonged use — rotate or use in 4-week-on/2-week-off cycles. Potency grades (Class I most potent: clobetasol propionate; Class IV least potent: hydrocortisone) guide site selection (face/flexures use low potency; palms/soles use high potency).
- Calcipotriol (calcipotriene): vitamin D3 analogue; binds VDR in keratinocytes → inhibits cell cycle progression → reduces proliferation and normalises differentiation. No skin atrophy. Effective as monotherapy and synergistic with corticosteroids in combination products.
- Coal tar and dithranol: older agents; still useful for scalp psoriasis (coal tar shampoos) and plaque psoriasis (dithranol 'short-contact therapy').
Moderate-severe psoriasis (>10% BSA, psoriatic arthritis, or functionally significant): systemic therapy:
- Methotrexate: antifolate DMARD; inhibits dihydrofolate reductase → blocks rapidly proliferating T-cells and keratinocytes. DOSE: 7.5–25 mg ONCE WEEKLY — NOT DAILY. Daily dosing at these doses is LETHAL from pancytopenia. Supplement with folic acid 5 mg once weekly (on a different day from methotrexate) to reduce mucositis. Monitor FBC, LFTs, creatinine monthly.
- Ciclosporin: calcineurin inhibitor; rapid onset; nephrotoxic with prolonged use; reserved for short courses.
- Acitretin: oral retinoid; particularly effective for pustular and erythrodermic psoriasis; highly teratogenic (must not be used in females of childbearing age unless absolutely necessary; teratogenicity persists for 3 years after stopping).
- Biologics: anti-TNF-α (infliximab, adalimumab, etanercept), anti-IL-17A (secukinumab, ixekizumab — particularly effective, PASI 90 in ~50%), anti-IL-23 (guselkumab, risankizumab) — for moderate-severe psoriasis unresponsive to conventional systemic therapy.
SELF-CHECK
A patient with severe nodular acne (multiple painful cysts, scarring) is prescribed oral isotretinoin. She is a 20-year-old woman who is sexually active. What is the mandatory monitoring requirement before and during isotretinoin therapy?
A. Monthly liver function tests and haematology only; no additional female-specific monitoring required
B. Negative pregnancy test before starting; two reliable forms of contraception throughout treatment; monthly pregnancy tests during therapy; continue contraception for 1 month after the last dose
C. Pregnancy test before starting is sufficient; contraception can be determined by patient preference
D. Weekly FBC monitoring to detect aplastic anaemia — the most dangerous adverse effect of isotretinoin
Reveal Answer
Answer: B. Negative pregnancy test before starting; two reliable forms of contraception throughout treatment; monthly pregnancy tests during therapy; continue contraception for 1 month after the last dose
Isotretinoin is Pregnancy Category X — it is teratogenic at therapeutic doses, causing major malformations (cranial, cardiac, CNS) in >25% of exposed foetuses. For every female patient of childbearing potential, the mandatory safety programme requires: (1) a documented negative pregnancy test BEFORE starting treatment; (2) TWO reliable forms of contraception throughout treatment; (3) monthly pregnancy tests during the course; (4) continuing contraception for at least 1 month after the last dose (isotretinoin has a short half-life but metabolites persist). In India, the Ministry of Health recommends a pregnancy prevention programme analogous to the US iPLEDGE system. This is a non-negotiable safety step, not optional monitoring.
Clinical Decision-Making in Dermatological Prescribing
Rational dermatological prescribing requires matching the drug, route, vehicle, and monitoring to the condition severity and patient profile.
Acne — step-up approach:
Mild (comedonal and mild inflammatory): topical retinoid ± benzoyl peroxide. Moderate (papulopustular, significant inflammatory): topical retinoid + benzoyl peroxide + topical clindamycin, or add oral doxycycline for 3–6 months. Severe (nodular/cystic, scarring potential): oral isotretinoin — refer to dermatologist. Females with hormonal acne: combined OCP with anti-androgenic progestin.
Sunscreen counselling — evidence-based:
SPF (Sun Protection Factor) measures UVB protection only. SPF 30 blocks 97% of UVB; SPF 50 blocks 98% of UVB. Higher SPF provides marginally more UVB protection but does NOT automatically provide better UVA protection — the 'broad spectrum' label (indicating UVA protection as well) is required. For Indian skin types and outdoor work, SPF 30 broad spectrum is the minimum recommendation. Physical blockers (zinc oxide, titanium dioxide) are photostable (do not degrade in sunlight), non-comedogenic, and preferred for sensitive skin, children, and patients with acne (chemical filters can be comedogenic). Apply 20–30 minutes before sun exposure; reapply every 2 hours or after swimming.
Methotrexate dosing safety in psoriasis:
The methotrexate weekly dosing rule is a critical prescribing safety issue. Methotrexate for psoriasis is 7.5–25 mg ONCE WEEKLY — the same drug given daily for cancer chemotherapy at these doses causes rapid lethal pancytopenia, mucositis, and hepatotoxicity. The mechanism difference: weekly dosing allows normal cells (but not rapidly proliferating skin cells and T-cells) to recover because most normal tissues have lower dihydrofolate reductase and can recover via the salvage pathway during the drug-free interval. Folic acid 5 mg ONCE weekly (not on the same day as methotrexate) reduces mucositis without significantly compromising efficacy.
Permethrin household treatment rule:
Failing to treat ALL household members simultaneously is the most common cause of scabies and pediculosis treatment failure and re-infestation. Every member of the household must apply permethrin on the same night, and all clothing, bed linen, and towels must be washed in hot water (>50°C) at the same time. Post-treatment itch (from dying mites and continued immune reaction) does not mean treatment failure — reassure patients that pruritus may persist for 2–4 weeks after successful scabies treatment.
CLINICAL PEARL
Clinical Pearl: Methotrexate for psoriasis is WEEKLY, not daily. This is the single most dangerous prescribing error in dermatology. Methotrexate for psoriasis and rheumatoid arthritis is always dosed ONCE A WEEK (7.5–25 mg). The same tablet strength used for chemotherapy, if given DAILY, has caused numerous patient deaths from pancytopenia and sepsis. When prescribing methotrexate, write both the dose AND the frequency explicitly ('Methotrexate 15 mg by mouth ONCE WEEKLY on Mondays') and always check that the patient and the dispensing pharmacist understand the weekly schedule. Ensure folic acid supplementation (5 mg weekly on a different day) is co-prescribed.