Page 23 of 33
PH9.7 | PH9.7 | Ocular Pharmacotherapy and Topical Delivery — SDL Guide — SDL Guide
Learning Objectives
- Describe the mechanism of action, uses, and adverse effects of anti-glaucoma drugs (prostaglandin analogues, beta-blockers, alpha-2 agonists, carbonic anhydrase inhibitors, miotics, hyperosmotic agents)
- Identify contraindications to ocular beta-blockers and brimonidine in specific clinical settings
- Outline the pharmacotherapy for other ocular conditions (bacterial/viral/allergic conjunctivitis, mydriasis, wet AMD)
- Explain the pharmacokinetics of topical ocular drug delivery, including blood-ocular barrier, nasolacrimal drainage, and punctal occlusion
INSTRUCTIONS
Glaucoma is the second leading cause of irreversible blindness worldwide, and in India affects an estimated 12 million people — over half of whom are unaware of their diagnosis. The pharmacotherapy of glaucoma centres on IOP reduction using eye drops, which are among the most widely prescribed medications in ophthalmology. Understanding topical ocular drug delivery — how drugs reach the anterior and posterior segments, how nasolacrimal drainage causes systemic absorption, and when systemic effects from eye drops can be dangerous — is essential for safe prescribing.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 10 (Ocular Pharmacology) (textbook)
- Goodman & Gilman. The Pharmacological Basis of Therapeutics, 13th ed., Ch. 66 (Ocular Pharmacology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 67-year-old man with chronic obstructive pulmonary disease (COPD) visits his ophthalmologist for his routine glaucoma follow-up. He has been using timolol 0.5% eye drops twice daily for three years. Today he presents with worsening breathlessness — his pulmonologist found new bronchospasm and adjusted his inhalers without improvement. No one questioned his eye drops. The connection: timolol is a non-selective beta-blocker that, when instilled as an eye drop, is absorbed systemically via the nasolacrimal duct — enough to reach systemic levels sufficient to cause bronchospasm in patients with obstructive airway disease. A simple switch to betaxolol (cardioselective beta-1 blocker) or a prostaglandin analogue (which has no systemic beta-blockade) would have prevented this. Eye drops are not pharmacologically inert — they reach the systemic circulation and can cause serious adverse effects.
WHY THIS MATTERS
Ocular pharmacology is clinically important well beyond ophthalmology. As a general physician, you will encounter patients on anti-glaucoma drops who develop systemic adverse effects (bradycardia, bronchospasm, depression, fatigue from timolol; systemic metabolic acidosis from acetazolamide). You will dilate pupils with mydriatics for fundoscopy and understand how to reverse inadvertent overdose. You will prescribe antibiotic and antiviral eye drops for conjunctivitis and herpes simplex keratitis. And you will understand why the nasolacrimal drainage system requires patients to use punctal occlusion to reduce systemic drug absorption. PH9.7 integrates pharmacology with clinical anatomy in a way that directly affects patient safety.
RECALL
From the Autonomic Nervous System cluster, recall that muscarinic receptors in the eye include M3 receptors on the iris sphincter (contraction = miosis) and the ciliary muscle (contraction = accommodation, 'spasm of near'). Atropine (muscarinic antagonist) blocks both: mydriasis (iris sphincter relaxes) and cycloplegia (ciliary muscle relaxes, loss of accommodation). Pilocarpine (muscarinic agonist) causes the opposite: miosis and ciliary muscle contraction, which pulls on the scleral spur and opens the trabecular meshwork. From the beta-blocker section, recall that timolol is a non-selective beta-blocker (blocks β1 and β2) — β2 blockade in the lung causes bronchoconstriction. Betaxolol is cardioselective (β1-selective), causing less bronchospasm. Also recall that carbonic anhydrase is the enzyme that facilitates CO₂ hydration to bicarbonate and H⁺ — the same reaction in the ciliary body produces the bicarbonate-rich aqueous humour; blocking it reduces aqueous humour production.
Aqueous Humour Dynamics and the Pathophysiology of Glaucoma
Understanding aqueous humour (AH) dynamics is the physiological basis for understanding how every anti-glaucoma drug works. Aqueous humour is a clear fluid produced by the ciliary body (via active secretion driven by carbonic anhydrase and Na⁺/K⁺-ATPase) at approximately 2–2.5 mL/minute. It flows from the posterior chamber, through the pupil into the anterior chamber, and drains primarily via two routes: (1) the trabecular meshwork route (conventional drainage, ~80%) — through the trabecular meshwork, Schlemm's canal, and into the episcleral venous system; and (2) the uveoscleral route (unconventional drainage, ~20%) — across the ciliary body face and supraciliary space into the uveal vasculature.
Intraocular pressure (IOP) is determined by the balance between aqueous humour production and drainage. Normal IOP is 10–21 mmHg. Elevated IOP is the primary risk factor for glaucomatous optic neuropathy — progressive death of retinal ganglion cells and their axons (which form the optic nerve), causing characteristic cupped optic disc and visual field loss.
Glaucoma pathophysiology — two main types:
- Open-angle glaucoma (OAG): The anterior chamber angle (where the trabecular meshwork is located) is open and appears structurally normal, but there is increased resistance at the trabecular meshwork, reducing drainage and gradually elevating IOP. The most common form; asymptomatic until late-stage. Most anti-glaucoma drugs target OAG.
- Angle-closure glaucoma (ACG): The iris physically obstructs the trabecular meshwork (the angle 'closes'). Acute ACG presents dramatically: sudden severe eye pain, halos around lights, blurred vision, nausea/vomiting, red eye, a mid-dilated fixed pupil, and corneal oedema — an ophthalmic emergency.
Elevated IOP damages the optic nerve through mechanical compression of axons at the lamina cribrosa and possibly through ischaemia. The damage is cumulative and irreversible — this is why early detection and IOP reduction are life-changing for patients with glaucoma.
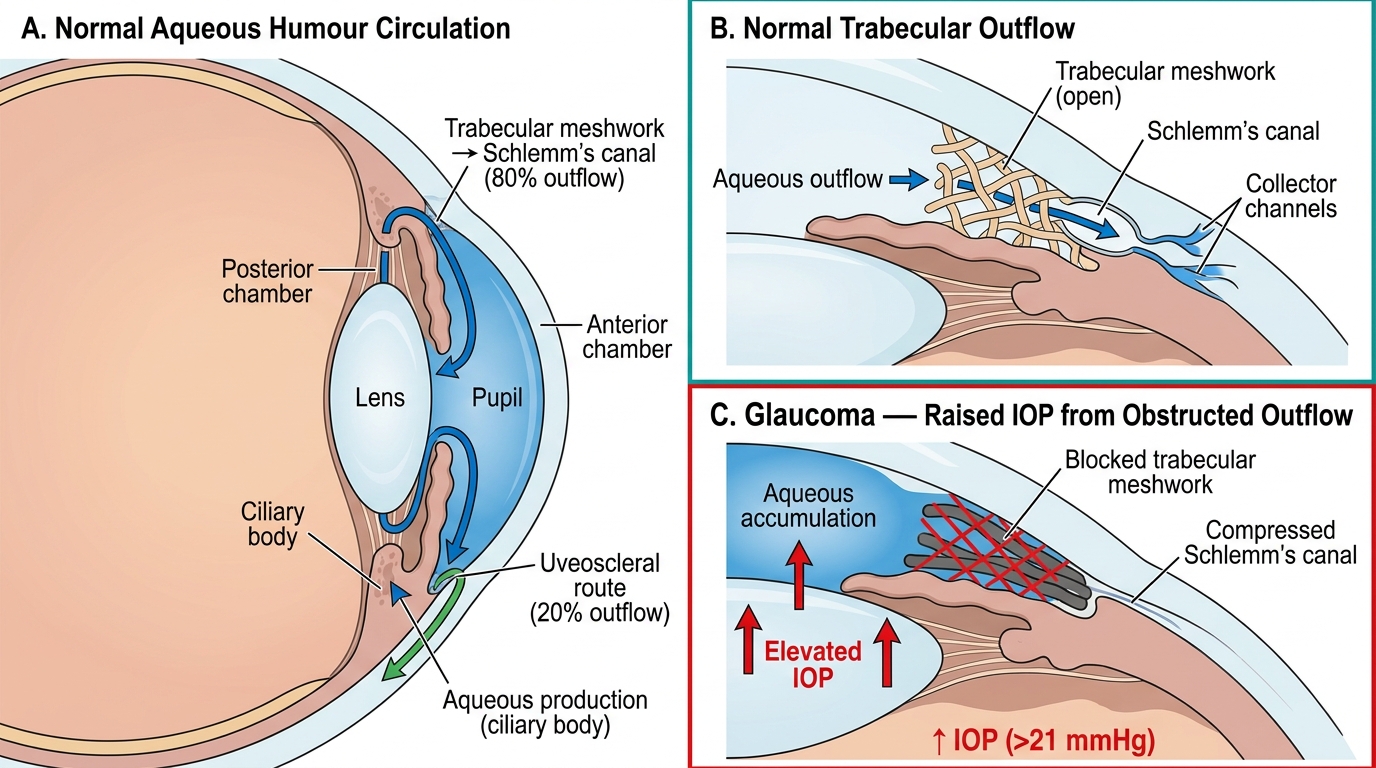
Aqueous Humour Circulation and IOP Regulation in the Anterior Eye
Therapeutic Goals in Ocular Pharmacotherapy
The therapeutic goals in ocular pharmacology vary by condition, but for glaucoma they are particularly well defined by both pathophysiology and clinical trial evidence.
Glaucoma — IOP reduction: The goal is to reduce IOP to a 'target IOP' that prevents further optic nerve damage. Target IOP is individualised — typically 18–20% reduction from baseline, or an absolute target below 21 mmHg for early disease, but lower (15–16 mmHg) for patients with advanced optic nerve damage or normal tension glaucoma. Lower is generally better. Any anti-glaucoma drug should be evaluated by: (1) magnitude of IOP reduction, (2) systemic contraindications, (3) local tolerability, and (4) dosing convenience (once-daily prostaglandins have better adherence than twice-daily timolol).
Other ocular conditions:
- Bacterial conjunctivitis: goal = kill or inhibit the causative organism (topical antibiotics); most cases are self-limiting, but antibiotics shorten duration.
- Herpes simplex keratitis: goal = suppress viral replication with antiviral (acyclovir ointment) without steroids (which can cause corneal perforation if used alone in herpes keratitis).
- Allergic conjunctivitis: goal = reduce mast cell-mediated histamine release and itch (mast cell stabilisers, antihistamines).
- Fundoscopy (diagnostic): goal = dilate pupil fully (mydriasis) and paralyse accommodation (cycloplegia) using atropine or tropicamide.
- Wet age-related macular degeneration (AMD): goal = stop neovascularisation by blocking VEGF (anti-VEGF injections).
Topical route rationale: Topical ocular administration achieves high drug concentrations at the target tissue (cornea, anterior chamber) while minimising systemic exposure compared to oral dosing. However, it is NOT systemic-exposure-free — nasolacrimal drainage carries unabsorbed drug to the nasolacrimal duct → nasal mucosa → systemic absorption, bypassing first-pass metabolism. For timolol and other drugs with systemic ADR potential, this absorption route is clinically significant.
Classification of Ocular Drugs
Ocular drugs are classified by indication and mechanism. The anti-glaucoma drugs form the most pharmacologically diverse group, as they target different steps in aqueous humour dynamics.
Anti-glaucoma drugs:
- Prostaglandin analogues: latanoprost, bimatoprost, travoprost — most potent single-agent IOP reducers; once-daily evening dosing; increase uveoscleral (unconventional) outflow
- Beta-blockers: timolol (non-selective), betaxolol (β1-selective) — reduce aqueous humour production; first-line in many settings; systemic absorption via nasolacrimal route
- Alpha-2 adrenergic agonists: brimonidine — reduce AH production AND increase uveoscleral outflow; dual mechanism
- Carbonic anhydrase inhibitors (CAIs): dorzolamide, brinzolamide (topical); acetazolamide (oral/IV) — reduce AH production by inhibiting ciliary body CAI
- Miotics (parasympathomimetics): pilocarpine — muscarinic agonist; increases trabecular drainage; less used since prostaglandins became available
- Hyperosmotic agents: mannitol (IV), glycerol (oral) — acute angle-closure emergency; reduces vitreous volume by osmotic dehydration
Drugs for other ocular conditions:
- Antibiotics: chloramphenicol (broad spectrum, topical; aplastic anaemia risk is theoretical with topical use), fluoroquinolones (ciprofloxacin, ofloxacin — first-line for bacterial keratitis and contact-lens-related infections)
- Antivirals: acyclovir ophthalmic ointment — herpes simplex keratitis; ganciclovir gel
- Antiallergic/mast cell stabilisers: olopatadine (dual antihistamine + mast cell stabiliser — first-line for allergic conjunctivitis), ketotifen, cromolyn sodium (pure mast cell stabiliser, prophylactic)
- Mydriatics and cycloplegics: atropine (longest acting — cycloplegia 10–14 days; used for treatment of amblyopia), tropicamide (short-acting 4–6 hours — preferred for routine fundoscopy), cyclopentolate
- Anti-VEGF agents: ranibizumab (Lucentis — Fab fragment), bevacizumab (Avastin — off-label full antibody), aflibercept (VEGF trap) — intravitreal injection for wet AMD and diabetic macular oedema
- Topical NSAIDs: diclofenac, nepafenac — post-operative inflammation, cystoid macular oedema prevention after cataract surgery
- Topical corticosteroids: prednisolone acetate, dexamethasone — for uveitis, post-operative inflammation; risk: steroid-induced glaucoma (IOP elevation) and steroid cataract with prolonged use
SELF-CHECK
A 60-year-old man with open-angle glaucoma and well-controlled asthma is started on a new IOP-lowering drug and develops progressive worsening of his asthma over the following 2 months. Which drug is most likely responsible, and what is the mechanism?
A. Latanoprost — it stimulates bronchial prostaglandin receptors causing bronchoconstriction
B. Timolol eye drops — non-selective beta-blocker absorbed systemically via the nasolacrimal duct, causing beta-2 blockade and bronchoconstriction
C. Brimonidine — alpha-2 agonist stimulates bronchoconstriction via adrenergic pathways
D. Dorzolamide — carbonic anhydrase inhibitor reduces bicarbonate in bronchial mucus causing airway irritation
Reveal Answer
Answer: B. Timolol eye drops — non-selective beta-blocker absorbed systemically via the nasolacrimal duct, causing beta-2 blockade and bronchoconstriction
Timolol is a non-selective beta-blocker that blocks both β1 (cardiac) and β2 (bronchial/vascular) adrenergic receptors. Although instilled as an eye drop, timolol is absorbed via the nasolacrimal duct into the nasal mucosa and then systemically, bypassing first-pass metabolism — achieving blood levels sufficient to block bronchial β2 receptors in susceptible patients. This causes bronchoconstriction, worsening asthma and COPD. Latanoprost (prostaglandin analogue) has no significant bronchial effects. The correct alternative for this patient would be betaxolol (cardioselective β1 blocker with significantly less β2 blockade) or switching to a prostaglandin analogue which has no systemic beta-blocking activity.