Page 24 of 33
PH9.7 | PH9.7 | Ocular Pharmacotherapy and Topical Delivery — SDL Guide — SDL Guide (Part 2)
Anti-Glaucoma Drugs: PK, PD, Uses and ADRs
Each anti-glaucoma drug class has a specific mechanism targeting one of the two determinants of IOP: production of aqueous humour or its outflow. Understanding the mechanism predicts both the efficacy and the adverse-effect profile.
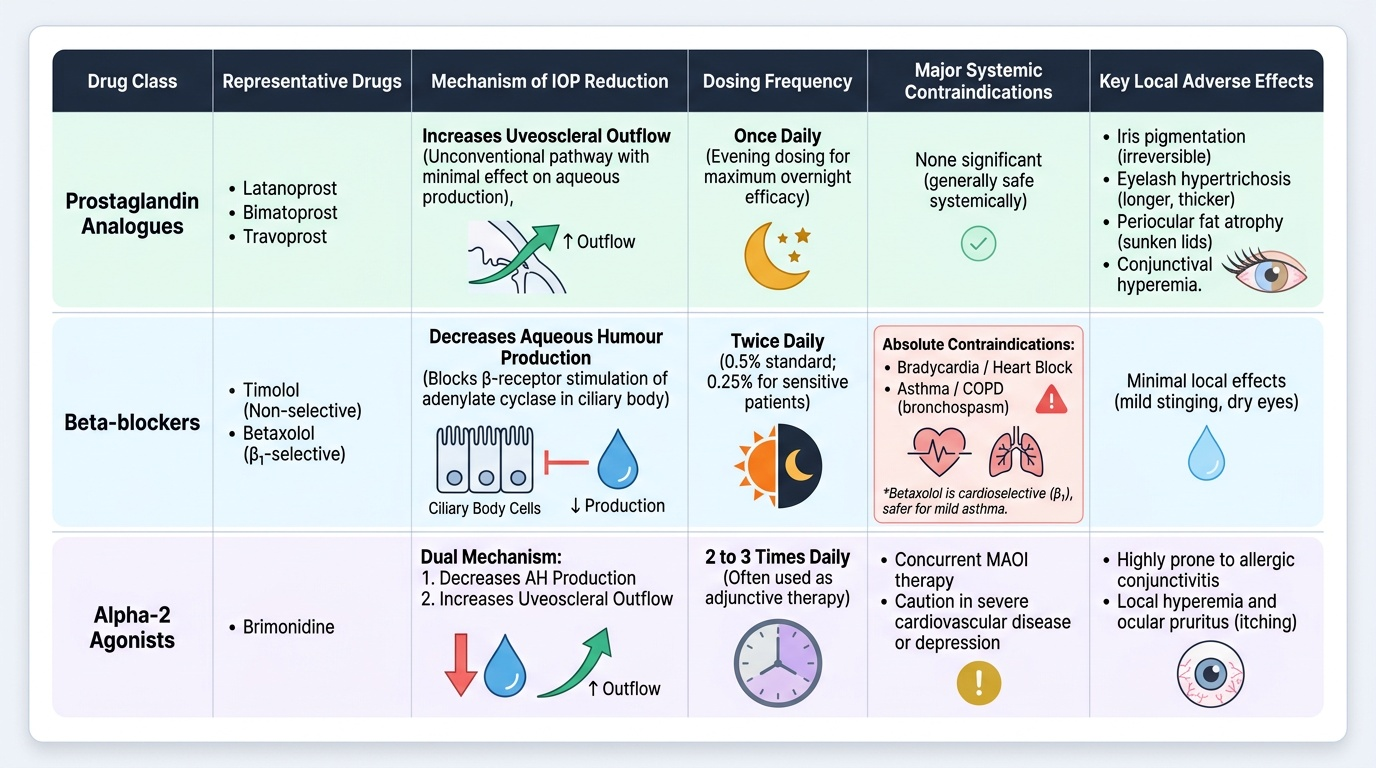
Prostaglandin analogues (latanoprost, bimatoprost, travoprost):
These are the most potent single-agent IOP-reducing drugs available, lowering IOP by 25–35% from baseline. They are prodrugs (ester form) that are hydrolysed in the cornea to the active acid form, which binds prostaglandin FP receptors on the ciliary body and trabecular meshwork, increasing uveoscleral (unconventional) outflow with minimal effect on aqueous production. Once-daily evening instillation (evening dosing correlates with maximum overnight IOP reduction). Local ADRs: iris pigmentation (melanin accumulation — irreversible, more common in mixed-colour irides); eyelash hypertrichosis and darkening (lengthening, thickening of lashes — actually sought by some patients); periocular fat atrophy (prostaglandin-induced adipocyte lipolysis — leads to enophthalmos, deepened upper lid sulcus); conjunctival hyperaemia.
Beta-blockers (timolol, betaxolol):
Timolol (non-selective) and betaxolol (β1-selective) reduce IOP by decreasing aqueous humour production from the ciliary body (via blocking β-receptor-mediated adenylate cyclase stimulation that drives active secretion). IOP reduction 20–27%. Timolol is instilled twice daily (0.5% standard; 0.25% for elderly/sensitive patients). Systemic absorption via nasolacrimal duct: bioavailability ~80% of the instilled dose reaches systemic circulation, bypassing hepatic first-pass metabolism. Systemic ADRs from timolol: bradycardia and heart block (β1 blockade — contraindicated in sinus bradycardia, AV block, decompensated heart failure), bronchospasm (β2 blockade — absolute contraindication in asthma and COPD), cold extremities, CNS effects (depression, vivid dreams, fatigue). Betaxolol (cardioselective, β1-selective) causes significantly less bronchospasm and is safer in mild-moderate asthma, but is less IOP-effective than timolol.
Alpha-2 agonists (brimonidine):
Brimonidine reduces AH production (via α2-mediated inhibition of adenylate cyclase in ciliary body) AND increases uveoscleral outflow — a dual mechanism making it useful as adjunctive therapy. IOP reduction ~20–25%. ADRs: allergic blepharoconjunctivitis (occurs in ~15–25% of patients with prolonged use — an important clinical reason for discontinuation), ocular hyperaemia, dry mouth, drowsiness. Absolute contraindication in infants (<2 years): brimonidine crosses the blood-brain barrier adequately in neonates/young infants (whose BBB is immature) and causes CNS depression (somnolence, hypotonia, bradycardia, apnoea) — a potentially life-threatening adverse effect documented in paediatric reports.
Carbonic anhydrase inhibitors (CAIs):
Dorzolamide (topical, 3 times daily) and brinzolamide (topical) inhibit carbonic anhydrase type II in the ciliary body epithelium, reducing the bicarbonate-driven active secretion of AH. IOP reduction ~15–20%. Topical ADRs: stinging on instillation (particularly dorzolamide — acidic pH), metallic taste (via systemic absorption and secretion in saliva). Acetazolamide (oral CAI): used for acute angle-closure glaucoma when rapid IOP reduction is required, or when topical therapy is insufficient. Dose: 250–500 mg four times daily. Systemic ADRs: hyperchloraemic metabolic acidosis (inhibits renal tubular CAI, reducing bicarbonate reabsorption), renal calculi (citraturia increases stone risk), paraesthesia (hands, feet — very common), sulfonamide hypersensitivity — contraindicated in sulfa allergy (CAIs are sulfonamide derivatives).
Miotics (pilocarpine):
Pilocarpine (0.5–4% eye drops) is a direct muscarinic agonist. It contracts the ciliary muscle, which pulls on the scleral spur and mechanically opens the trabecular meshwork, increasing conventional drainage. Also causes miosis (iris sphincter contraction). Uses: historically a first-line glaucoma drug; now largely replaced by more effective/better-tolerated agents; still used for acute angle-closure crisis (together with other agents) and in narrow-angle glaucoma to prevent closure. ADRs: spasm of accommodation (induced myopia — problematic in young patients, causing blurred distance vision); induced myopia; brow ache; night driving difficulty (due to miosis reducing light entry).
Hyperosmotic agents (mannitol IV, glycerol oral):
For acute angle-closure glaucoma emergency, when rapid IOP reduction is urgently needed while laser peripheral iridotomy is arranged. Mannitol IV (1–2 g/kg over 30–45 min) creates an osmotic gradient across the blood-ocular barrier, drawing fluid from the vitreous body into the bloodstream → reduces vitreous volume and mechanically pushes the lens-iris complex forward, relieving the angle closure. Contraindicated in heart failure and renal failure (fluid overload risk).
Provided image
SELF-CHECK
A 45-year-old woman presents to the emergency department with sudden severe right eye pain, visual blurring, halos around lights, nausea, and a mid-dilated fixed right pupil with corneal haziness. Her IOP is measured at 58 mmHg. What is the diagnosis and which drug class should be started immediately to lower IOP while awaiting laser iridotomy?
A. Bacterial endophthalmitis — start topical fluoroquinolone antibiotics
B. Acute angle-closure glaucoma — start IV mannitol and topical pilocarpine, with a systemic carbonic anhydrase inhibitor (acetazolamide), while arranging urgent laser peripheral iridotomy
C. Open-angle glaucoma — start topical latanoprost once daily
D. Herpes simplex keratitis — start topical acyclovir ointment
Reveal Answer
Answer: B. Acute angle-closure glaucoma — start IV mannitol and topical pilocarpine, with a systemic carbonic anhydrase inhibitor (acetazolamide), while arranging urgent laser peripheral iridotomy
The clinical presentation — sudden severe eye pain, halos, blurred vision, mid-dilated fixed pupil, corneal oedema (haziness from corneal oedema), and IOP 58 mmHg — is the classic presentation of acute angle-closure glaucoma (AACG). This is an ophthalmic emergency: untreated, the rapidly elevated IOP causes irreversible optic nerve ischaemia within hours. Immediate management: IV mannitol (or oral glycerol) to rapidly lower IOP by reducing vitreous volume; pilocarpine eye drops (to constrict the pupil and pull the iris away from the angle); acetazolamide oral/IV (reduces AH production); topical beta-blocker or CAI. Definitive treatment is laser peripheral iridotomy to create an alternative drainage pathway. Latanoprost alone is too slow (works over days) for this acute emergency.
Other Ocular Conditions and Topical Drug Delivery
Beyond glaucoma, ocular pharmacotherapy spans infection, allergy, inflammation, vascular disorders, and diagnostic procedures — all requiring an understanding of topical drug delivery principles.
Topical antibiotics:
For bacterial conjunctivitis (commonly caused by Staphylococcus aureus, Haemophilus influenzae, Streptococcus pneumoniae): chloramphenicol eye drops (broad spectrum, cost-effective; theoretical risk of aplastic anaemia with topical use is extremely rare); fluoroquinolones (ciprofloxacin 0.3%, ofloxacin 0.3%) — first-line for bacterial keratitis and contact-lens-associated infections (broader gram-negative coverage). Neomycin-polymyxin B-gramicidin (Neosporin) — combination for mild bacterial conjunctivitis. Viral conjunctivitis (adenoviral — the most common cause of epidemic conjunctivitis) does NOT respond to antibiotics — self-limiting, supportive care only.
Topical antivirals:
Acyclovir ophthalmic ointment 3% — for herpes simplex keratitis (dendritic ulcer on the cornea — diagnosed on fluorescein staining). Acyclovir inhibits HSV DNA polymerase after conversion to acyclovir triphosphate by viral thymidine kinase. Critical rule: do NOT use topical corticosteroids alone in herpes simplex keratitis — steroids suppress the host immune response while promoting viral replication, potentially causing corneal stromal melting and perforation. Corticosteroids can be used ONLY in stromal keratitis under antiviral cover.
Antiallergic drugs:
Olopatadine is a dual-action agent (antihistamine H1 receptor antagonist + mast cell stabiliser) — the preferred first-line for allergic conjunctivitis. Ketotifen — similar dual mechanism. Cromolyn sodium — pure mast cell stabiliser, prophylactic (must be started before allergen exposure). Topical corticosteroids are reserved for severe allergic eye disease (only with ophthalmologist supervision due to risk of steroid-induced glaucoma and cataract).
Mydriatics and cycloplegics:
Tropicamide (0.5–1%) — short-acting muscarinic antagonist; mydriasis lasting 4–6 hours; minimal cycloplegia; standard for routine fundoscopy. Atropine (1%) — long-acting; mydriasis and cycloplegia lasting 10–14 days; used for amblyopia treatment (penalisation of the better eye), uveitis (to prevent posterior synechiae by keeping the iris mobile), and refraction in children. Phenylephrine (2.5–10%) — sympathomimetic (alpha-1 agonist); mydriasis without cycloplegia; used in combination with tropicamide for fundoscopy.
Anti-VEGF intravitreal injections:
Ranibizumab (Lucentis) and bevacizumab (Avastin — off-label) inhibit VEGF-A, preventing the pathological neovascularisation in wet age-related macular degeneration (AMD), diabetic macular oedema, and retinal vein occlusion. Administered by intravitreal injection by the ophthalmologist. Bevacizumab (the oncology anti-VEGF) is used off-label for wet AMD because it is orders of magnitude cheaper than ranibizumab with similar efficacy (CATT trial). ADRs: endophthalmitis (rare but serious infection from intravitreal injection), rhegmatogenous retinal detachment, subconjunctival haemorrhage at injection site.
Topical ocular drug delivery — pharmacokinetics:
The eye has multiple barriers to drug entry. For anterior segment drugs (glaucoma, conjunctivitis): the cornea is the main route of drug absorption into the anterior chamber — drugs penetrate the cornea via transcellular (lipid-soluble drugs) or paracellular (hydrophilic drugs) routes. Optimal corneal penetration requires appropriate lipophilicity (log P value).
A critical pharmacokinetic feature: after a drop is instilled, only 5–10% of the dose is actually absorbed through the cornea into the anterior chamber. The rest — approximately 90% — drains via the nasolacrimal duct to the nasal cavity, where the rich mucosal vasculature absorbs it directly into the systemic circulation, bypassing first-pass hepatic metabolism. This is why timolol eye drops can reach systemic blood levels comparable to oral timolol for some patients.
Punctal occlusion technique: after instilling the eye drop, the patient presses a fingertip gently over the inner corner of the eye (the punctal area, where the lacrimal canaliculus opens) for 2–3 minutes. This physically blocks nasolacrimal drainage and increases the time available for corneal absorption while reducing the volume of drug reaching systemic circulation by approximately 40–50%. This technique is particularly important for timolol in patients with cardiac or pulmonary disease.
Vehicle formulations:
- Eye drops (aqueous solution) — most common; rapid drainage; short contact time
- Ophthalmic ointments (petrolatum-based) — longer corneal contact time; useful for overnight use and for irritated eyes; blurs vision temporarily
- Ophthalmic gels — intermediate between drops and ointments; once-daily timolol gel-forming solution (Timoptol XE) improves compliance
- Ocular inserts (e.g. Pilopine HS — pilocarpine insert) — sustained delivery; once-weekly; high compliance
Clinical Decision-Making in Ocular Prescribing
Rational ocular prescribing requires integrating the mechanism of action, systemic contraindications, local tolerability, and the specific clinical scenario.
First-line in open-angle glaucoma:
Prostaglandin analogues (latanoprost, bimatoprost) are the preferred first-line agents in most current guidelines: most potent single-agent IOP reduction (25–35%), once-daily dosing (evening), and their adverse effects are primarily local (iris pigmentation, eyelash hypertrichosis) with no significant systemic contraindications except in patients with uveitis or diabetic macular oedema (controversial). Beta-blockers (timolol) remain a commonly used first-line alternative, particularly where cost is a concern, but are contraindicated in asthma and COPD.
Contraindication navigation:
- Timolol → asthma/COPD: use betaxolol (less β2 blockade) or switch to prostaglandin analogue
- Timolol → bradycardia/heart block/decompensated heart failure: use prostaglandin analogue or brimonidine
- Brimonidine → infant (<2 years): NEVER use — CNS depression risk; use topical CAI or beta-blocker instead
- Acetazolamide → sulfa allergy: use topical CAI (dorzolamide) — topical CAIs are also sulfonamides but cross-reactivity with systemic CAIs is less clearly established; use with caution
- Acetazolamide → sickle cell disease: contraindicated — metabolic acidosis worsens sickling and can cause retinal vascular occlusion
Acute angle-closure glaucoma emergency:
Immediate management: IV mannitol (1–2 g/kg over 30–45 min) to lower IOP rapidly + pilocarpine eye drops (miosis pulls iris away from angle) + acetazolamide 500 mg IV/oral + topical beta-blocker. Arrange urgent laser peripheral iridotomy as definitive treatment.
Step-up in open-angle glaucoma:
If single-agent fails to reach target IOP: add a second agent from a different class. Common combinations: prostaglandin + timolol (twice-daily combinations available, e.g. Xalacom); prostaglandin + brimonidine; CAI + beta-blocker. If two agents fail, consider laser trabeculoplasty or surgical trabeculectomy.
CLINICAL PEARL
Clinical Pearl: Teach patients the punctal occlusion technique for every ocular beta-blocker prescription. Simply telling a patient to put in their timolol drops twice a day is incomplete prescribing. Timolol absorbed via the nasolacrimal duct bypasses first-pass metabolism and reaches systemic circulation in clinically significant amounts. In elderly patients with undiagnosed mild heart disease or borderline COPD, this can cause symptomatic bradycardia, worsening heart failure, or bronchoconstriction. Demonstrating punctal occlusion — press the inner eye corner for 2–3 minutes after instilling the drop — reduces systemic absorption by ~40–50%. This technique is particularly critical for patients who have any cardiac or respiratory concern.