Page 1 of 34
PH3.1 | PH3.1 | General Anaesthetics and Pre-Anaesthetic Medication — SDL Guide — SDL Guide
Learning Objectives
- Classify general anaesthetics into inhalational and intravenous categories with key agents in each
- Describe the salient pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of major general anaesthetic agents
- Identify the rationale for and classes of pre-anaesthetic medication
- Apply pharmacological principles to choose appropriate anaesthetic agents for specific clinical scenarios
INSTRUCTIONS
General anaesthesia underlies every major surgical intervention. Understanding which agents to use — and which to avoid — in specific patients (paediatrics, haemodynamic instability, raised intracranial pressure, malignant hyperthermia susceptibility) is both a patient-safety imperative and a core pharmacology competency. This module builds the pharmacological framework needed for rational, scenario-based agent selection.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 26 (General Anaesthetics) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 20 (General Anaesthesia) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old child requires an elective tonsillectomy. The anaesthetist needs to induce anaesthesia without IV access — the child is terrified of needles. She selects sevoflurane for inhalational induction because of its pleasant, non-pungent odour and rapid onset. Within seconds the child is breathing comfortably, unconscious. This smooth induction is possible because the anaesthetist understands blood-gas partition coefficients, MAC, and the distinct profiles of each inhalational agent — the same pharmacological reasoning that prevents a tragedy in a MH-susceptible patient or avoids raised ICP in a neurosurgery case.
WHY THIS MATTERS
Every surgical patient you will encounter will have been exposed to general anaesthesia or will require it. As a prescriber you need to understand why the anaesthetist selected each drug in the pre-operative medication chart, why halothane is rarely used in modern practice, and why ketamine is avoided in a hypertensive patient. Adverse events — malignant hyperthermia, emergence agitation, diffusion hypoxia — occur rapidly and require immediate recognition and management. The pharmacological principles in this module are the basis for writing a rational pre-anaesthetic prescription and communicating safely with the anaesthetic team.
RECALL
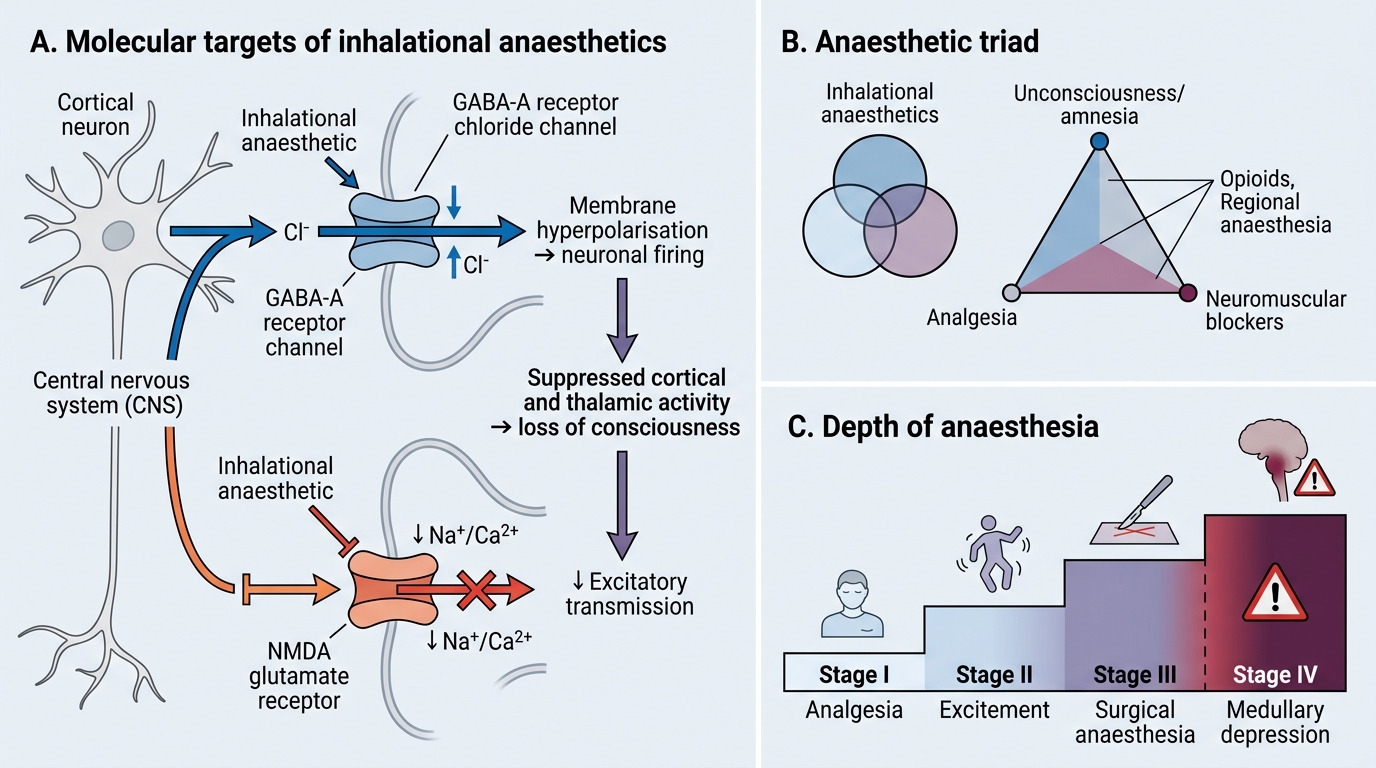
Before proceeding, recall from your Year-1 physiology: the GABA-A receptor is a ligand-gated Cl⁻ channel — when GABA binds, Cl⁻ flows in, hyperpolarising the neuron. The NMDA receptor is a voltage- and ligand-gated cation channel mediating fast excitatory transmission; Mg²⁺ normally blocks it at resting membrane potential. Recall that lipid solubility determines CNS penetration speed (the partition coefficient principle). These are the molecular targets and biophysical principles upon which general anaesthetic pharmacology rests. Also recall the classification of neuromuscular blocking agents (depolarising: succinylcholine; non-depolarising: rocuronium) — these are used alongside GAs to achieve muscle relaxation (the third limb of the anaesthetic triad).
Neuropharmacology of Anaesthesia — Mechanism Overview
General anaesthesia is a reversible, drug-induced state of unconsciousness, analgesia, amnesia, and immobility sufficient to permit surgery. Despite decades of research, no single unifying molecular theory explains all anaesthetic actions, but two receptor systems dominate: enhancement of GABA-A-mediated inhibition (potentiating Cl⁻ influx) and inhibition of NMDA-receptor-mediated excitation. Most inhalational agents and IV barbiturates/propofol/benzodiazepines act predominantly on GABA-A receptors, increasing the frequency (benzodiazepines) or duration (barbiturates, inhalational) of Cl⁻ channel opening. Ketamine, uniquely, is an NMDA-receptor antagonist, blocking the ion channel in a non-competitive, voltage-dependent manner; this produces a dissociative state rather than classical loss of consciousness.
The depth of anaesthesia is traditionally described in four stages (Guedel's stages for ether, now adapted): Stage I (analgesia), Stage II (excitement/delirium — a danger zone for vomiting and airway complications), Stage III (surgical anaesthesia, divided into four planes), and Stage IV (medullary depression — cardiovascular and respiratory arrest). Modern balanced anaesthesia, using multiple agents, navigates directly from Stage I to Stage III and reverses rapidly, avoiding the prolonged Stage II seen with ether.
The anaesthetic triad — unconsciousness, analgesia, and muscle relaxation — reflects the fact that no single drug optimally achieves all three goals. Unconsciousness is produced by the GA; analgesia requires opioid supplements (or ketamine); muscle relaxation is provided by neuromuscular blocking drugs. This balanced approach reduces the total dose of each agent, minimising adverse effects while achieving the required surgical conditions.
Inhalational Anaesthetics: CNS Mechanism and Depth of Anaesthesia
Goals of General Anaesthesia and the Anaesthetic Triad
The overarching therapeutic goal of general anaesthesia is to achieve a controlled, reversible state that allows surgical intervention to proceed safely, with the patient experiencing no awareness, pain, or distressing movement — and to recover from that state smoothly, rapidly, and without lasting harm. This goal is framed pharmacologically by the anaesthetic triad: the three distinct physiological endpoints that must be simultaneously achieved.
The first limb — unconsciousness and amnesia — protects the patient from psychological trauma. It is mediated primarily by the general anaesthetic agent (inhalational or IV). The second limb — analgesia — is critical because the anaesthetic state alone does not suppress the pain pathways that produce haemodynamic responses (tachycardia, hypertension) to surgical stimuli; opioids or regional anaesthesia provide this. The third limb — muscle relaxation — is essential for intubation and for relaxing the abdominal wall in laparotomy; it is achieved with neuromuscular blocking agents, not the anaesthetic itself.
Understanding the triad explains why modern general anaesthesia is always balanced (polypharmacy by design): a lower dose of each agent reduces toxicity from any single drug and allows each drug to do what it does best. The anaesthetist's skill lies in titrating all three limbs simultaneously and reversing each safely — a process that requires knowing the PK of every agent in play.
- Unconsciousness: inhalational GA or IV induction agent (propofol, thiopental, ketamine)
- Analgesia: opioid (fentanyl, morphine) or ketamine (has intrinsic analgesic property)
- Muscle relaxation: succinylcholine (depolarising) or rocuronium/vecuronium (non-depolarising)
Classification of General Anaesthetics
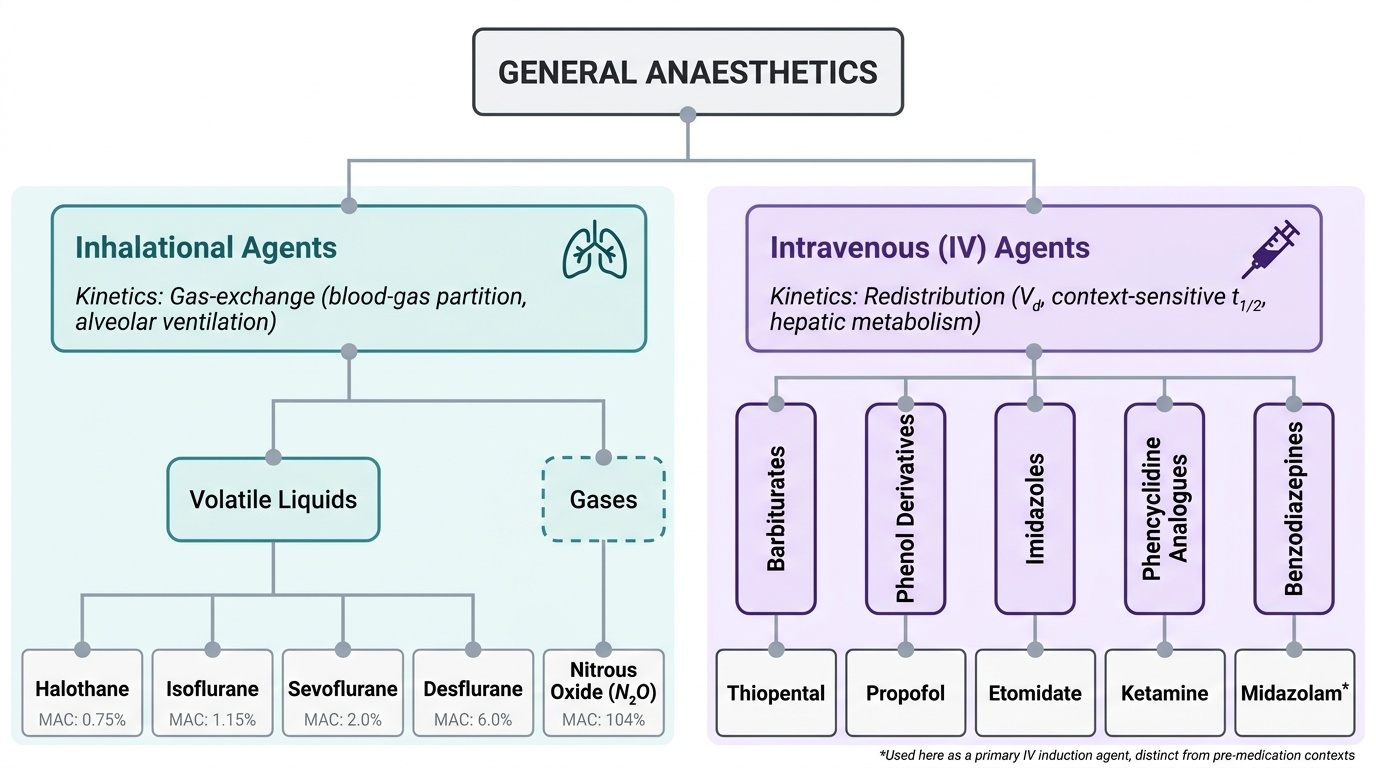
General anaesthetics are classified by their route of administration into two broad groups: inhalational agents (administered as gases or vapours via the respiratory tract) and intravenous agents (administered directly into the bloodstream). This classification is clinically and pharmacokinetically meaningful: inhalational agents are governed by gas-exchange pharmacokinetics (blood-gas partition coefficient, MAC, alveolar ventilation), while IV agents behave according to redistribution kinetics (Vd, hepatic metabolism, context-sensitive half-life).
Within inhalational agents, the sub-classification is further divided into volatile liquids (administered as vapour) and gases (administered directly). Among IV agents, chemically diverse drugs (barbiturates, phenol-derivatives, imidazoles, phencyclidine analogues, benzodiazepines) are grouped by mechanism and structural class. Note that benzodiazepines used as pre-anaesthetic medications are a distinct use-context — in this classification, midazolam appears as an IV GA in its own right, not as a pre-med.
Provided image
| Class | Sub-class | Key Agents |
|---|---|---|
| Inhalational | Volatile liquids | Halothane, Isoflurane, Sevoflurane, Desflurane |
| Inhalational | Gaseous | Nitrous oxide (N₂O) |
| Intravenous | Barbiturate | Thiopental |
| Intravenous | Phenol derivative | Propofol |
| Intravenous | Imidazole | Etomidate |
| Intravenous | NMDA antagonist | Ketamine |
| Intravenous | Benzodiazepine | Midazolam |