Page 2 of 34
PH3.1 | PH3.1 | General Anaesthetics and Pre-Anaesthetic Medication — SDL Guide — SDL Guide (Part 2)
Inhalational Agents — PK, PD, Uses, and ADRs
Inhalational agents exert their effect through the lungs. The key pharmacokinetic parameter governing speed of onset and recovery is the blood-gas partition coefficient (λ): a low λ means the agent is poorly soluble in blood and quickly reaches equilibrium between alveolar gas and arterial blood, producing faster induction and faster recovery. MAC (Minimum Alveolar Concentration) is the standard measure of potency: the alveolar concentration of an agent at 1 atmosphere that prevents 50% of patients from moving in response to a standard surgical stimulus. Lower MAC = higher potency.
High λ agents (halothane, ether) are slow onset and slow recovery. Low λ agents (desflurane, sevoflurane) are fast. Sevoflurane's low pungency makes it ideal for inhalational induction (especially in children); desflurane is pungent and airway-irritating, making it unsuitable for induction but useful for maintenance where rapid emergence is desired.
Halothane: the oldest modern volatile agent. Sensitises the myocardium to catecholamines (ventricular arrhythmias), potent trigger of malignant hyperthermia (in RYR1-mutation patients), and causes immune-mediated hepatotoxicity (halothane hepatitis), particularly with repeated exposures. Largely superseded by sevoflurane and isoflurane.
Isoflurane: low hepatotoxicity, mild coronary steal phenomenon (in patients with coronary artery disease), good muscle relaxant potentiation.
Sevoflurane: most commonly used for inhalational induction (pleasant smell, low λ, non-irritant), safe in paediatrics, can produce compound A (nephrotoxic in animal studies at high concentrations — low clinical risk at standard flow rates).
Desflurane: fastest emergence (lowest λ), excellent for prolonged cases requiring rapid wake-up; highly pungent — never used for induction.
Nitrous oxide (N₂O): MAC >100% (cannot produce surgical anaesthesia alone at safe concentrations); used as an adjuvant to reduce requirements for potent agents. Carries risk of diffusion hypoxia at recovery (rapid efflux dilutes alveolar O₂ — give 100% O₂ for 5 min at end of anaesthesia). Inactivates vitamin B₁₂ (methionine synthase inhibition) — prolonged exposure risks megaloblastic changes; avoid in patients with B₁₂ deficiency. Expands gas-filled cavities (pneumothorax, bowel obstruction) — a contraindication in those settings.
| Agent | MAC (%) | Blood:gas λ | Key Property | Notable ADR |
|---|---|---|---|---|
| Halothane | 0.75 | 2.4 | Bronchodilator | Hepatotoxicity, MH trigger |
| Isoflurane | 1.2 | 1.4 | Widely used maintenance | Coronary steal (mild) |
| Sevoflurane | 2.0 | 0.65 | Paediatric induction | Compound A at low flow |
| Desflurane | 6.0 | 0.42 | Fastest emergence | Airway irritant, pungent |
| Nitrous oxide | >100 | 0.47 | Adjuvant, analgesia | Diffusion hypoxia, B₁₂ inhibition |
Intravenous Agents — PK, PD, Uses, and ADRs
Intravenous agents produce anaesthesia by redistribution from brain to muscle and fat (highly lipid-soluble drugs). The initial dose produces rapid unconsciousness (within one arm-brain circulation time); recovery after a single bolus is mainly by redistribution (not metabolism), which is why single-dose thiopental has a short clinical action despite a long elimination half-life.
Thiopental: the prototype ultra-short-acting barbiturate. Highly lipid-soluble, rapid onset (30 seconds). Mechanism: potentiates GABA-A by prolonging Cl⁻ channel open time. Uses: IV induction, status epilepticus (refractory). ADRs: no analgesia (hyperalgesia at sub-anaesthetic doses — paradoxical pain facilitation), profound respiratory depression, laryngospasm on airway instrumentation, extravasation causes tissue necrosis (highly alkaline solution). Contraindicated in porphyria (induces ALA-synthase).
Propofol: phenol-derivative, GABA-A potentiator. Rapid induction and recovery (very short context-sensitive half-life). Advantages: anti-emetic property (reduces PONV), total intravenous anaesthesia (TIVA), used for procedural sedation. ADRs: pain on injection, profound hypotension (vasodilation + myocardial depression), apnoea at induction, propofol infusion syndrome (rare, prolonged high-dose ICU use: metabolic acidosis, cardiac failure).
Etomidate: imidazole, GABA-A potentiator. Haemodynamically neutral — does NOT drop blood pressure (unlike propofol/thiopental). Preferred for induction in haemodynamic instability (trauma, shock). ADRs: pain on injection, myoclonus (involuntary jerks at induction), adrenocortical suppression (single induction dose suppresses cortisol for 6-8 hours — avoid prolonged infusion in critically ill).
Ketamine: NMDA-receptor antagonist. Produces a unique dissociative anaesthesia — the patient appears awake (eyes open, reflexes preserved) but is unaware and analgesic. Preserves airway reflexes and causes bronchodilation (useful in severe asthma, emergency field anaesthesia). Produces sympathetic stimulation (tachycardia, hypertension, increased ICP) — contraindicated in hypertension, coronary artery disease, and raised intracranial pressure. ADRs: emergence reactions (hallucinations, vivid dreams — attenuated by benzodiazepine co-administration), excessive secretions (give anticholinergic pre-med), muscle rigidity.
Midazolam: benzodiazepine (GABA-A — increases frequency of Cl⁻ channel opening). Used as IV induction agent or as a pre-med/sedation adjuvant; amnesia property is valuable. Reversed by flumazenil (GABA-A antagonist). Respiratory depression is potentiated by opioids.
| Agent | Mechanism | Key Use | Key ADR |
|---|---|---|---|
| Thiopental | Barbiturate (GABA-A ↑duration) | Rapid induction | No analgesia, porphyria CI |
| Propofol | Phenol (GABA-A) | TIVA, anti-emetic | Hypotension, pain on injection |
| Etomidate | Imidazole (GABA-A) | Haemodynamic instability | Adrenal suppression, myoclonus |
| Ketamine | NMDA antagonist | Asthma, field anaesthesia | Raised ICP CI, emergence reactions |
| Midazolam | Benzodiazepine (GABA-A ↑frequency) | Pre-med, sedation | Respiratory depression |
Pre-Anaesthetic Medications — Rationale, Classes, and Agents
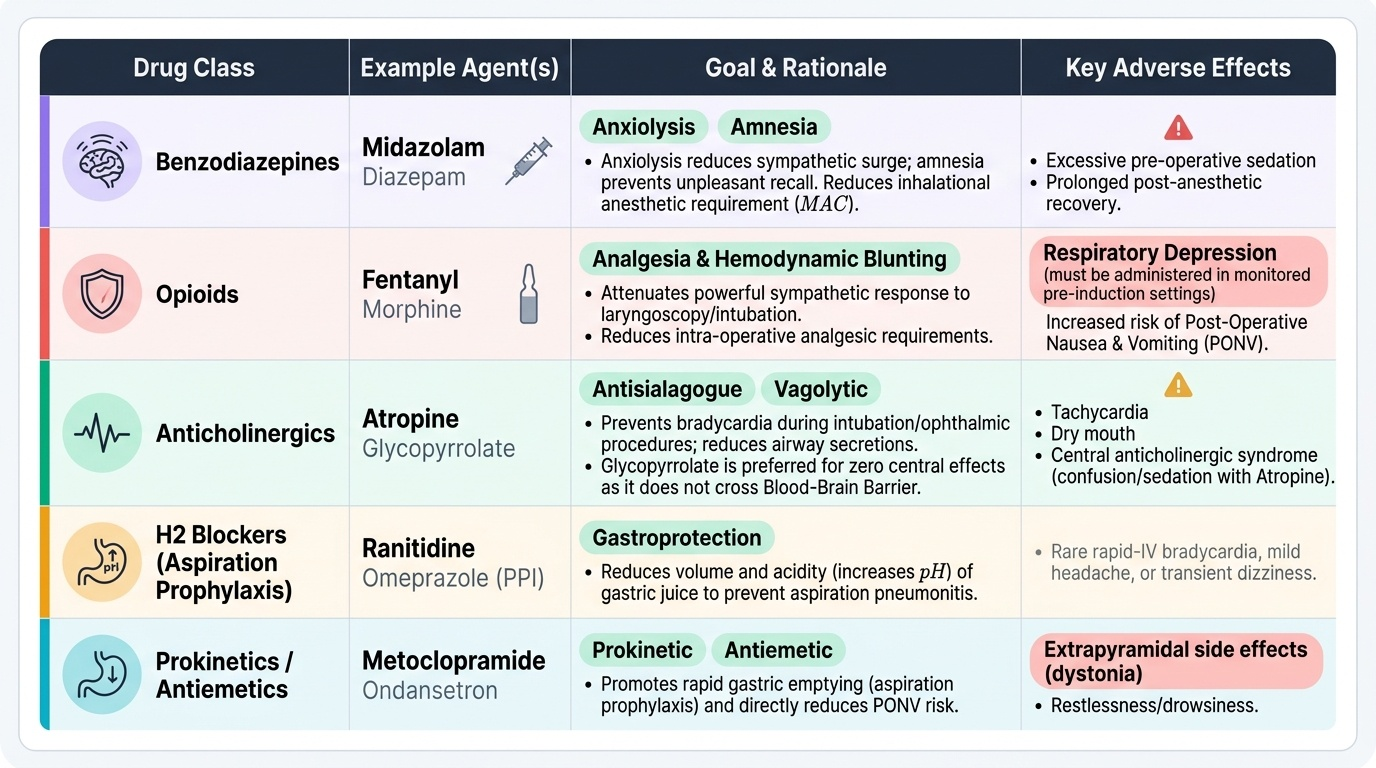
Pre-anaesthetic medication (premedication) refers to drugs given before anaesthesia to optimise the patient's condition and reduce perioperative risks. Each drug class serves a distinct, complementary purpose within the overall peri-operative management strategy.
The anticholinergic agents (atropine, glycopyrrolate) were historically essential to prevent ether-induced excessive secretions; in modern volatile anaesthetic practice their routine use is reduced, but they remain important to counter vagal bradycardia during intubation, laryngoscopy, or ophthalmic procedures. Glycopyrrolate does not cross the blood-brain barrier and therefore does not cause central anticholinergic effects (confusion, sedation) — preferred over atropine for antisialagogue purpose.
Benzodiazepines (oral diazepam the evening before, or IV midazolam 30 min before induction) serve dual roles: anxiolysis reduces the sympathetic surge during induction, and amnesia prevents recall of unpleasant pre-operative events. They also reduce the dose requirement (MAC) for the inhalational agent.
Opioid analgesics (morphine, fentanyl) given as pre-medication attenuate the haemodynamic response to intubation (laryngoscopy is a powerful sympathetic stimulus) and reduce intra-operative analgesic requirements. Risk: respiratory depression pre-induction — must be given in a monitored setting.
Antiemetic premedication (metoclopramide, ondansetron) reduces post-operative nausea and vomiting (PONV) risk. Aspiration prophylaxis — ranitidine or omeprazole (reduces gastric acidity) and metoclopramide (promotes gastric emptying) — is given before emergency surgery or in patients at risk (full stomach, GORD) to reduce Mendelson's syndrome risk.
Provided image
| Drug Class | Example Agent | Goal | Key Adverse Effect |
|---|---|---|---|
| Anticholinergic | Atropine, Glycopyrrolate | Reduce secretions, prevent bradycardia | Tachycardia, dry mouth |
| Benzodiazepine | Diazepam, Midazolam | Anxiolysis, amnesia | Respiratory depression |
| Opioid | Morphine, Fentanyl | Pre-emptive analgesia, attenuate intubation response | Respiratory depression, nausea |
| H₂ blocker / PPI | Ranitidine, Omeprazole | Reduce gastric acidity (aspiration prophylaxis) | Headache |
| Prokinetic/antiemetic | Metoclopramide, Ondansetron | Prevent PONV, promote gastric emptying | Extrapyramidal reactions (metoclopramide) |
SELF-CHECK
Which inhalational anaesthetic is the preferred choice for inhalational induction in children, and why?
A. Halothane — highest potency (lowest MAC)
B. Sevoflurane — pleasant odour, low blood:gas partition coefficient, non-airway-irritant
C. Desflurane — fastest onset due to lowest partition coefficient
D. Nitrous oxide — safest agent with no systemic toxicity
Reveal Answer
Answer: B. Sevoflurane — pleasant odour, low blood:gas partition coefficient, non-airway-irritant
Sevoflurane is preferred for inhalational induction in paediatrics because of its non-pungent, sweet smell (good patient acceptance), low blood:gas partition coefficient (0.65 — rapid equilibration and fast onset), and minimal airway irritability. Halothane, though potent, carries risk of hepatotoxicity and MH. Desflurane is the most pungent and causes airway irritation — it is never used for induction. N₂O alone cannot produce surgical anaesthesia (MAC >100%).
SELF-CHECK
A patient with suspected raised intracranial pressure requires emergency anaesthesia. Which IV induction agent should be AVOIDED and why?
A. Propofol — causes severe hypotension that reduces cerebral perfusion pressure
B. Ketamine — increases cerebral blood flow and ICP through sympathetic stimulation
C. Etomidate — suppresses cortisol, worsening neurological outcome
D. Thiopental — causes porphyria crisis in neurosurgical patients
Reveal Answer
Answer: B. Ketamine — increases cerebral blood flow and ICP through sympathetic stimulation
Ketamine stimulates the sympathetic nervous system, increasing cerebral blood flow and metabolic rate, which raises ICP. It is therefore contraindicated in patients with raised ICP. Propofol (preferred in neurosurgery — slightly reduces ICP) or thiopental (reduces ICP, used in refractory intracranial hypertension) are suitable alternatives. Etomidate's adrenal suppression is a consideration in prolonged critical illness, not a contraindication in isolated neurosurgery induction.
SELF-CHECK
Malignant hyperthermia (MH) is a life-threatening complication triggered by volatile anaesthetic agents and succinylcholine. What is the definitive treatment?
A. Propofol infusion — rapidly clears the triggering agent and restores GABA-A balance
B. Dantrolene — blocks ryanodine receptor-mediated Ca²⁺ release from sarcoplasmic reticulum
C. Haloperidol — controls the hypermetabolic state via D₂ receptor blockade
D. IV paracetamol — reduces hyperthermia by cyclooxygenase inhibition
Reveal Answer
Answer: B. Dantrolene — blocks ryanodine receptor-mediated Ca²⁺ release from sarcoplasmic reticulum
MH is caused by a mutation in the ryanodine receptor (RYR1) that leads to uncontrolled Ca²⁺ release from the sarcoplasmic reticulum when triggered by volatile GAs or succinylcholine, producing life-threatening hyperthermia, muscle rigidity, metabolic acidosis, and rhabdomyolysis. Dantrolene is the specific antidote — it blocks the ryanodine receptor (type 1), halting Ca²⁺ release. Immediate steps also include stopping the triggering agent, cooling, and correcting acidosis/hyperkalemia.
CLINICAL PEARL
Halothane is a potent trigger of malignant hyperthermia — in any patient with a family history of MH or an unexpectedly high temperature during anaesthesia, halt volatile agent and succinylcholine immediately and administer IV dantrolene (2.5 mg/kg, repeat up to 10 mg/kg). MH is fatal without prompt recognition. Additionally, etomidate's haemodynamic neutrality makes it the induction agent of choice in haemodynamic instability — but even a single induction dose suppresses cortisol production for 6-8 hours by blocking adrenal 11β-hydroxylase. Anticipate this in trauma or sepsis patients who may need stress-dose steroids post-induction.