Page 4 of 34
PH3.2 | PH3.2 | Sedative and Hypnotic Agents — SDL Guide — SDL Guide
Learning Objectives
- Classify sedative-hypnotic agents by chemical class and differentiate their mechanisms of action
- Describe the pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of benzodiazepines, barbiturates, and Z-drugs
- Explain the pharmacological basis for selecting among sedative-hypnotics for specific clinical scenarios
- Identify the risks of dependence, withdrawal, and overdose, and describe their management
INSTRUCTIONS
Insomnia and anxiety-related sleep disturbances are among the most common presentations in clinical practice. The pharmacological management of these conditions requires careful selection among a spectrum of agents with very different mechanisms, safety profiles, and dependence liabilities. This module equips you with the reasoning framework to prescribe sedative-hypnotics rationally — including knowing when not to prescribe them.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 27 (Sedative-Hypnotics) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 17 (Hypnotics and Sedatives) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old woman with chronic back pain presents requesting 'sleeping pills'. She has been taking diazepam nightly for the past three months. She admits the tablets no longer work as well as they did and she feels anxious if she misses a dose. On examination, she is alert but slow to react. Her daughter reports that she fell twice in the past month. This scenario — benzodiazepine tolerance, dependence, and fall risk in an elderly patient — illustrates why the pharmacological basis for selecting and using sedative-hypnotics matters far beyond the simple act of writing a prescription.
WHY THIS MATTERS
You will encounter patients on sedative-hypnotics in every clinical setting — wards, outpatient clinics, emergency departments, and intensive care units. As a prescriber, you must know why a short-acting agent is preferred over a long-acting one for sleep-onset insomnia in an elderly patient, why barbiturates have been largely replaced by benzodiazepines and Z-drugs, and why flumazenil can rapidly reverse benzodiazepine overdose. The pharmacological distinctions between these drug classes are not academic — they determine patient safety and therapeutic success.
RECALL
Recall from Year-1 physiology and biochemistry: the GABA-A receptor is a pentameric ligand-gated ion channel that, when activated by GABA, allows Cl⁻ to flow inward, hyperpolarising the postsynaptic neuron. Recall that GABA is the principal inhibitory neurotransmitter of the CNS. Also recall the concept of receptor subunits — the GABA-A receptor is composed of α, β, and γ subunits in various combinations; this subunit composition determines which binding sites are present and which pharmacological effects a drug produces. These foundational principles explain why benzodiazepines, barbiturates, and Z-drugs — all acting on the GABA-A complex — produce subtly different pharmacological profiles.
Pathophysiology of Insomnia and Sleep Architecture
Normal sleep cycles between NREM (non-rapid eye movement, stages N1-N3) and REM (rapid eye movement) sleep, with roughly 90-minute cycle repetitions across the night. Deep slow-wave sleep (N3) predominates in the early night and is essential for physical restoration; REM sleep predominates in the later night and is essential for memory consolidation and emotional regulation. The circadian rhythm is orchestrated by the suprachiasmatic nucleus (SCN), which drives melatonin secretion from the pineal gland in darkness — melatonin signals the onset of the biological night and promotes sleep propensity.
Wakefulness is actively maintained by two complementary systems: the ascending reticular activating system (ARAS), driven by noradrenaline, serotonin, histamine, and acetylcholine, and the orexin (hypocretin) system from the lateral hypothalamus, which tonically activates the ARAS. Sleep onset requires suppression of both systems, orchestrated by GABAergic and galaninergic neurons in the ventrolateral preoptic area (VLPO).
Insomnia arises when this finely balanced arousal-sleep switch malfunctions — either due to hyperarousal of the ARAS (anxiety, pain, caffeine), inadequate VLPO inhibitory tone (ageing, stress), or disrupted circadian signalling. Understanding this pathophysiology explains why different pharmacological targets (GABA-A potentiation, melatonin agonism, orexin antagonism) offer different approaches to the same clinical problem.
- Sleep-onset insomnia: difficulty falling asleep → short-acting hypnotics, melatonin
- Sleep-maintenance insomnia: frequent awakenings → intermediate-acting hypnotics
- Terminal insomnia: early morning awakening → often a marker of depression, not primary insomnia
Goals of Sedative-Hypnotic Therapy
The therapeutic goal of sedative-hypnotic therapy is to restore adequate sleep quantity and quality — or to achieve anxiolytic sedation for procedural or peri-operative purposes — using the agent with the narrowest necessary pharmacological footprint, the shortest required duration, and the lowest dependence liability. This goal is grounded in the pharmacological principle of rational drug selection: the drug class, dose, duration, and timing of administration must match the specific clinical need.
Non-pharmacological approaches (sleep hygiene, stimulus control, cognitive behavioural therapy for insomnia [CBT-I]) are the first-line treatment for chronic insomnia — pharmacotherapy is reserved for short-term (≤4 weeks) use or for specific clinical indications (perioperative sedation, status epilepticus, acute anxiety states, alcohol withdrawal). The pharmacological basis for choosing among available agents depends on four clinical factors: (1) the desired duration of action (sleep-onset vs sleep-maintenance), (2) the specific indication (pure insomnia vs anxiety-related insomnia vs procedural sedation), (3) patient characteristics (age, hepatic function, dependence risk), and (4) the need for reversibility in overdose (benzodiazepines — reversible with flumazenil; barbiturates — no antidote).
- Short-term insomnia: short-acting BZD (temazepam) or Z-drug (zolpidem, zopiclone)
- Anxiety-related insomnia: intermediate BZD with anxiolytic properties
- Procedural sedation / pre-op: IV midazolam (rapid onset, retrograde amnesia)
- Status epilepticus: IV diazepam or lorazepam (anticonvulsant BZD use)
- Chronic insomnia: CBT-I first; ramelteon or suvorexant if pharmacotherapy needed (low dependence)
Classification of Sedative-Hypnotic Agents
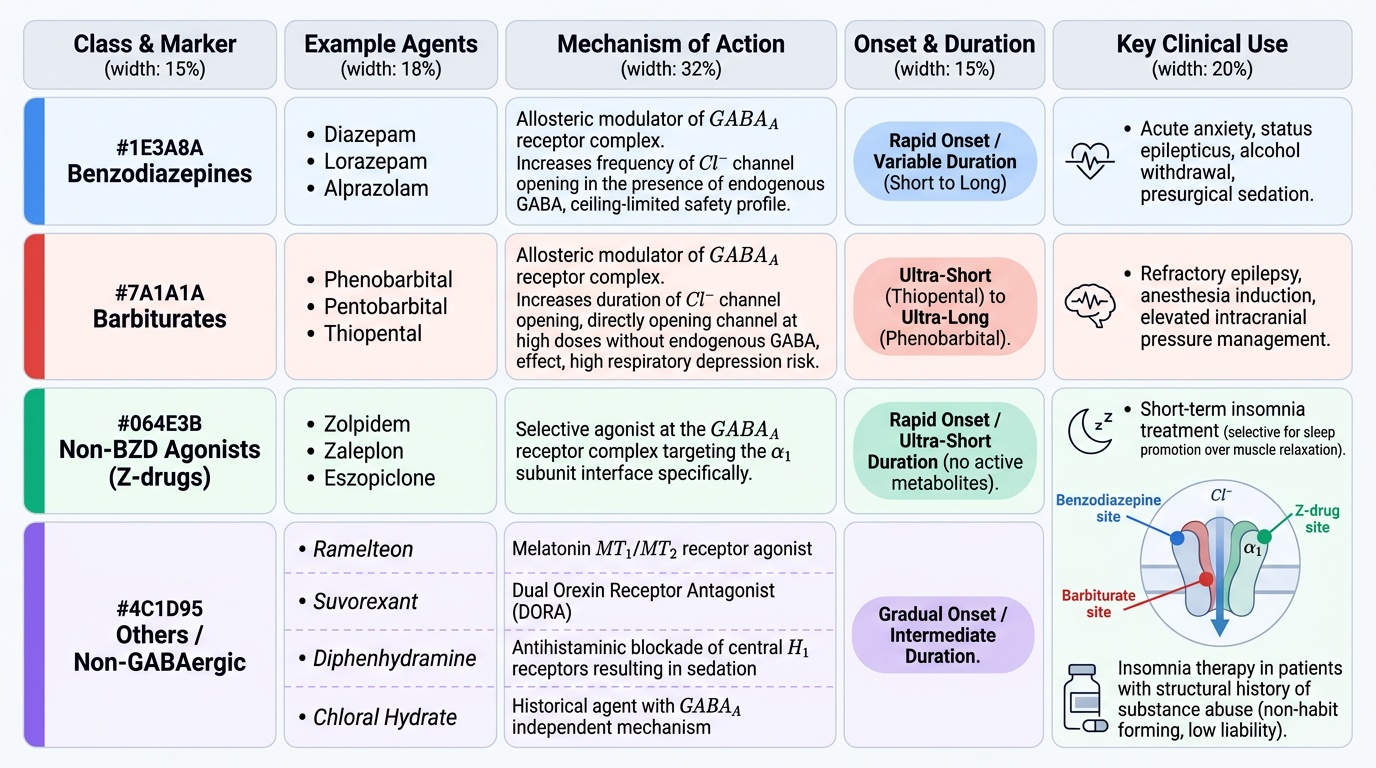
Sedative-hypnotic agents are classified by their chemical structure and primary molecular mechanism. The two major classes — benzodiazepines and barbiturates — both target the GABA-A receptor complex but through distinct binding sites and with very different pharmacological consequences. A third class, the non-benzodiazepine GABA-A agonists (Z-drugs), acts on the same receptor with greater subunit selectivity. A fourth group includes agents acting via other mechanisms: melatonin receptor agonists (ramelteon), orexin receptor antagonists (suvorexant), and older agents such as chloral hydrate (historical, GABA-A independent) and antihistamines (diphenhydramine — sedation via H1 blockade).
This classification matters clinically because it determines mechanism of overdose, reversal options, dependence liability, and drug interaction profiles. Benzodiazepines have a safer overdose profile than barbiturates because their GABA-A potentiation is ceiling-limited by endogenous GABA availability; barbiturates can open the Cl⁻ channel directly at high doses, producing dose-dependent respiratory depression without a ceiling.
Provided image