Page 7 of 34
PH3.3 | PH3.3 | Antiseizure Drugs and Uncontrolled Seizure Management — SDL Guide — SDL Guide
Learning Objectives
- Classify antiseizure drugs by mechanism of action and identify key agents in each class
- Describe the pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of major antiseizure drugs
- Match seizure type to appropriate drug(s) and identify agents that worsen specific seizure types
- Devise a stepwise pharmacological management plan for uncontrolled seizure (status epilepticus)
INSTRUCTIONS
Epilepsy affects approximately 50 million people worldwide. Wrong drug choice — prescribing phenytoin or carbamazepine for absence seizures — can paradoxically worsen seizure frequency. Recognising and correctly managing status epilepticus within minutes can prevent permanent brain injury. This module builds the pharmacological decision framework for rational antiseizure drug selection and emergency seizure management.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 29 (Antiepileptic Drugs) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 17 (Pharmacotherapy of the Epilepsies) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 10-year-old girl is brought to clinic because she 'stares into space' for 10-20 seconds several times a day, especially during schoolwork. Her teacher calls them 'daydreams'. Her mother mentions that a doctor at another facility prescribed carbamazepine last month. Since starting the drug, her episodes have become more frequent. You recognise these as absence seizures — and carbamazepine is one of the agents that can paradoxically worsen them. Stopping carbamazepine and starting ethosuximide or valproate (the correct drugs for absence seizures) dramatically improves her school performance. This case illustrates why the antiseizure drug-seizure type matrix is not optional knowledge — it is patient safety.
WHY THIS MATTERS
You will encounter patients with epilepsy in every clinical rotation and in practice. You must know which antiseizure drug is appropriate for which seizure type — and which drugs are contraindicated for certain types. You will be expected to write a management plan for status epilepticus (an emergency where incorrect or delayed pharmacological intervention causes irreversible brain injury). The pharmacokinetics of phenytoin (zero-order kinetics, narrow therapeutic window) and the teratogenicity of valproate (contraindicated in pregnant women except when essential) are examined in licensing assessments and have direct patient-care implications.
RECALL
Recall from Year-1 physiology: the action potential is driven by rapid Na⁺ influx through voltage-gated Na⁺ channels (depolarisation) followed by K⁺ efflux (repolarisation). Neuronal excitability depends on the balance between excitatory input (glutamate → NMDA/AMPA receptors → cation influx) and inhibitory input (GABA → GABA-A → Cl⁻ influx → hyperpolarisation). Also recall that thalamo-cortical circuits generate the 3 Hz spike-and-wave discharge of absence seizures, driven by abnormal T-type Ca²⁺ current in thalamic relay neurons. These physiological targets — Na⁺ channels, T-type Ca²⁺ channels, GABA-A receptors, glutamate receptors — are the molecular basis of antiseizure pharmacology.
Pathophysiology of Seizures — Abnormal Neuronal Excitability
A seizure is a transient episode of abnormal, excessive, or synchronous neuronal activity in the brain. The underlying pathophysiology involves a failure of the normal balance between neuronal excitation (glutamate/AMPA/NMDA) and inhibition (GABA/Cl⁻), resulting in a runaway positive feedback of neuronal firing. Three primary ionic mechanisms drive different seizure types:
Voltage-gated Na⁺ channels: high-frequency repetitive firing in tonic-clonic and partial seizures is sustained by rapid cycling of Na⁺ channels through resting → activated → inactivated states. Na⁺-channel-blocking drugs (phenytoin, carbamazepine) stabilise the inactivated state, preventing rapid re-opening and thereby limiting high-frequency firing without blocking normal (low-frequency) neuronal activity.
T-type Ca²⁺ channels in thalamic neurons: the characteristic 3 Hz spike-and-wave discharge of absence seizures is generated in thalamo-cortical loops by oscillatory low-threshold Ca²⁺ currents through T-type Ca²⁺ channels. Blocking these channels (ethosuximide) abolishes absence seizures without affecting fast Na⁺-channel-dependent firing — which is why ethosuximide is effective for absence but not for tonic-clonic seizures.
GABAergic inhibition failure: reduced GABAergic tone (due to GABA synthesis defects, receptor mutations, or drug withdrawal) removes the brake on neuronal firing. Drugs that enhance GABA-A (barbiturates, benzodiazepines, vigabatrin, tiagabine, gabapentin) restore inhibitory tone.
Seizures are classified by whether they involve one cerebral hemisphere (focal/partial — previously: partial) or both (generalised). Generalised seizures include: absence (brief behavioural arrest), tonic-clonic (grand mal — tonic phase followed by clonic phase), myoclonic (brief muscle jerks), and atonic ('drop attacks'). This classification drives drug selection: a drug effective for one type may be useless or harmful for another.
Therapeutic Goals and Principles of Antiseizure Therapy
The overarching therapeutic goal of antiseizure therapy is seizure freedom (complete seizure control) with the minimum effective drug dose, minimum adverse effects, and preserved quality of life. For a patient whose seizures are not life-threatening, adverse effects and teratogenicity may outweigh seizure risk; for a patient with status epilepticus, rapid pharmacological control is life-saving and adverse effects are secondary.
Key principles guiding drug selection include:
Seizure-type specificity: the single most important selection criterion. The choice of drug must match the seizure type because: (a) some drugs are ineffective for certain types, and (b) some drugs paradoxically worsen certain types (phenytoin and carbamazepine can worsen absence and myoclonic seizures by suppressing cortical inhibition without correcting the thalamic oscillation).
Spectrum (narrow vs broad): ethosuximide and carbamazepine are narrow-spectrum agents (effective for specific seizure types only). Valproate, levetiracetam, and lamotrigine are broad-spectrum (effective across multiple types).
Drug level monitoring: phenytoin requires therapeutic drug monitoring (target 10-20 µg/mL) due to its zero-order kinetics and narrow therapeutic window. Valproate and carbamazepine levels are measured when toxicity or non-compliance is suspected. Levetiracetam and lamotrigine generally do not require routine monitoring.
Special populations: valproate should be avoided in women of childbearing potential (teratogen: neural tube defects); lamotrigine is preferred in pregnancy. Phenobarbitone remains first-line in neonates. Drug interactions (enzyme induction by phenytoin, carbamazepine, phenobarbitone) must be considered in patients on multiple medications.
Classification of Antiseizure Drugs by Mechanism
Antiseizure drugs are best classified by their primary molecular mechanism, because this determines their seizure-type selectivity, interaction profiles, and ADR patterns.
1. Sodium channel blockers (use-dependent stabilisation of the inactivated state): phenytoin, carbamazepine, oxcarbazepine, lamotrigine, lacosamide, and valproate (as one of its multiple mechanisms). These drugs are effective for focal/partial seizures and generalised tonic-clonic seizures. They do NOT address the T-type Ca²⁺ mechanism of absence seizures and may paradoxically worsen them by disrupting cortical-thalamic regulation.
2. T-type Ca²⁺ channel blockers: ethosuximide — narrow-spectrum agent active only at thalamic T-type Ca²⁺ channels; effective for absence seizures only. Valproate also has T-type Ca²⁺ blocking activity (contributing to its broad-spectrum profile).
3. GABA enhancers: multiple sub-mechanisms — (a) GABA-A positive allosteric modulators: benzodiazepines (diazepam, lorazepam — IV for acute seizures/SE), phenobarbitone; (b) GABA transaminase inhibitors: vigabatrin (irreversible — visual field defects); (c) GABA re-uptake inhibitors: tiagabine; (d) GABA-B agonist: baclofen (not primary ASD). Gabapentin and pregabalin bind α₂δ subunit of voltage-gated Ca²⁺ channels (not GABA per se, despite the name) — useful adjuncts.
4. Glutamate/SV2A modulators: levetiracetam binds synaptic vesicle protein 2A (SV2A), inhibiting neurotransmitter exocytosis — a unique mechanism with broad-spectrum efficacy and minimal pharmacokinetic drug interactions. Topiramate has multiple mechanisms (Na⁺ block + GABA enhancement + AMPA/kainate antagonism + carbonic anhydrase inhibition).
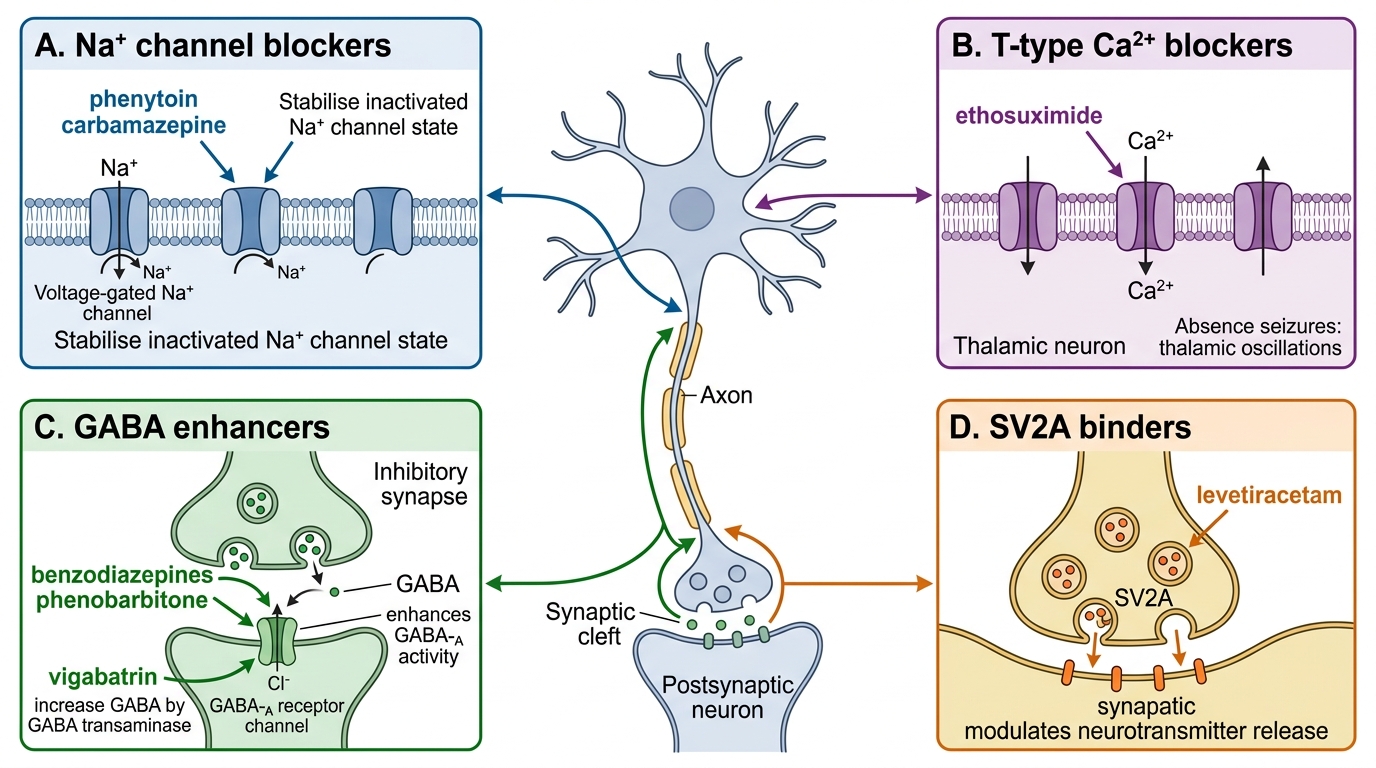
Mechanisms of Major Antiseizure Drug Classes