Page 8 of 34
PH3.3 | PH3.3 | Antiseizure Drugs and Uncontrolled Seizure Management — SDL Guide — SDL Guide (Part 2)
Major Antiseizure Drugs — PK, PD, Uses, and ADRs
Phenytoin: Na⁺ channel blocker. Uses: focal and generalised tonic-clonic seizures, status epilepticus (IV). Unique PK: zero-order (saturation) kinetics at therapeutic concentrations — small dose increments cause disproportionately large rises in plasma level, making titration hazardous. Therapeutic range: 10-20 µg/mL. ADRs: dose-related (nystagmus → ataxia → confusion → cardiac arrhythmias); chronic effects — gingival hyperplasia, hirsutism, coarsening of facial features, peripheral neuropathy, megaloblastic anaemia (folate antagonism), osteomalacia (CYP induction → vitamin D metabolism). Teratogen (fetal hydantoin syndrome — cleft palate, cardiac defects). Strong CYP inducer. IV phenytoin: cardiotoxic (hypotension, arrhythmias) — must be given slowly (≤50 mg/min); fosphenytoin (water-soluble prodrug) is preferred for IV loading.
Carbamazepine: Na⁺ channel blocker. First-line for focal/partial seizures and trigeminal neuralgia. Auto-induction: induces its own CYP3A4 metabolism over 2-4 weeks, requiring dose adjustment. ADRs: diplopia, ataxia, aplastic anaemia/agranulocytosis (rare but serious), hyponatraemia (SIADH), hepatotoxicity. Stevens-Johnson syndrome/TEN risk — especially in HLA-B1502 carriers (South/Southeast Asian populations — genetic testing recommended before prescribing). Strong CYP inducer → reduces levels of OCPs, warfarin, other ASDs. Avoid in absence and myoclonic seizures.
Valproate (Sodium valproate): broad-spectrum — Na⁺ block + T-type Ca²⁺ block + increased GABA synthesis/decreased degradation. Effective for absence, tonic-clonic, myoclonic, and focal seizures. Teratogen: neural tube defects (spina bifida ~1-2%), autism spectrum disorder in offspring — contraindicated in pregnancy unless no alternative; mandatory folic acid supplementation if used. ADRs: weight gain, hair loss (alopecia, usually transient), tremor, hepatotoxicity (rare but potentially fatal — especially in children under 2 on polytherapy), thrombocytopaenia, PCOS-like syndrome in women.
Ethosuximide: T-type Ca²⁺ blocker — first-line for childhood absence seizures (along with valproate); ineffective for other seizure types. Well tolerated. ADRs: GI upset (nausea, vomiting), hiccups, drowsiness, lupus-like syndrome (rare).
Levetiracetam: SV2A binding — unique mechanism, minimal drug interactions (no CYP induction/inhibition), broad-spectrum. Increasingly first-line for many seizure types. ADRs: behavioural changes (irritability, aggression, depression — clinically important), somnolence. Renal excretion (dose-adjust in renal impairment).
Lamotrigine: Na⁺ channel blocker (+ mild Ca²⁺). Broad-spectrum, well tolerated. Preferred in women of childbearing potential (safer than valproate in pregnancy). ADR: Stevens-Johnson syndrome (especially with rapid titration or when combined with valproate — valproate inhibits lamotrigine metabolism via glucuronidation, increasing lamotrigine levels); must titrate slowly.
Phenobarbitone: barbiturate, GABA-A enhancer (↑duration of Cl⁻ channel opening). First-line for neonatal seizures, used in febrile convulsions and in resource-limited settings for epilepsy. Long half-life (80-100h), once-daily dosing. Strong CYP inducer — multiple drug interactions. ADRs: sedation, cognitive impairment, paradoxical hyperactivity in children, dependence, enzyme induction.
| Drug | Mechanism | Seizure Types | Key ADRs |
|---|---|---|---|
| Phenytoin | Na⁺ block | Focal, TC, SE | Zero-order kinetics, gingival hyperplasia, folate deficiency |
| Carbamazepine | Na⁺ block | Focal, TC, trigeminal neuralgia | SJS risk (HLA-B1502), hyponatraemia, CYP inducer |
| Valproate | Na⁺ + Ca²⁺ + GABA | Broad-spectrum | Teratogen (NTD), hepatotoxicity, weight gain |
| Ethosuximide | T-Ca²⁺ block | Absence ONLY | GI upset, hiccups |
| Levetiracetam | SV2A | Broad-spectrum | Behavioural changes |
| Lamotrigine | Na⁺ block | Broad-spectrum | SJS (slow titration), valproate interaction |
| Phenobarbitone | GABA-A | Neonatal, general | Sedation, CYP inducer, dependence |
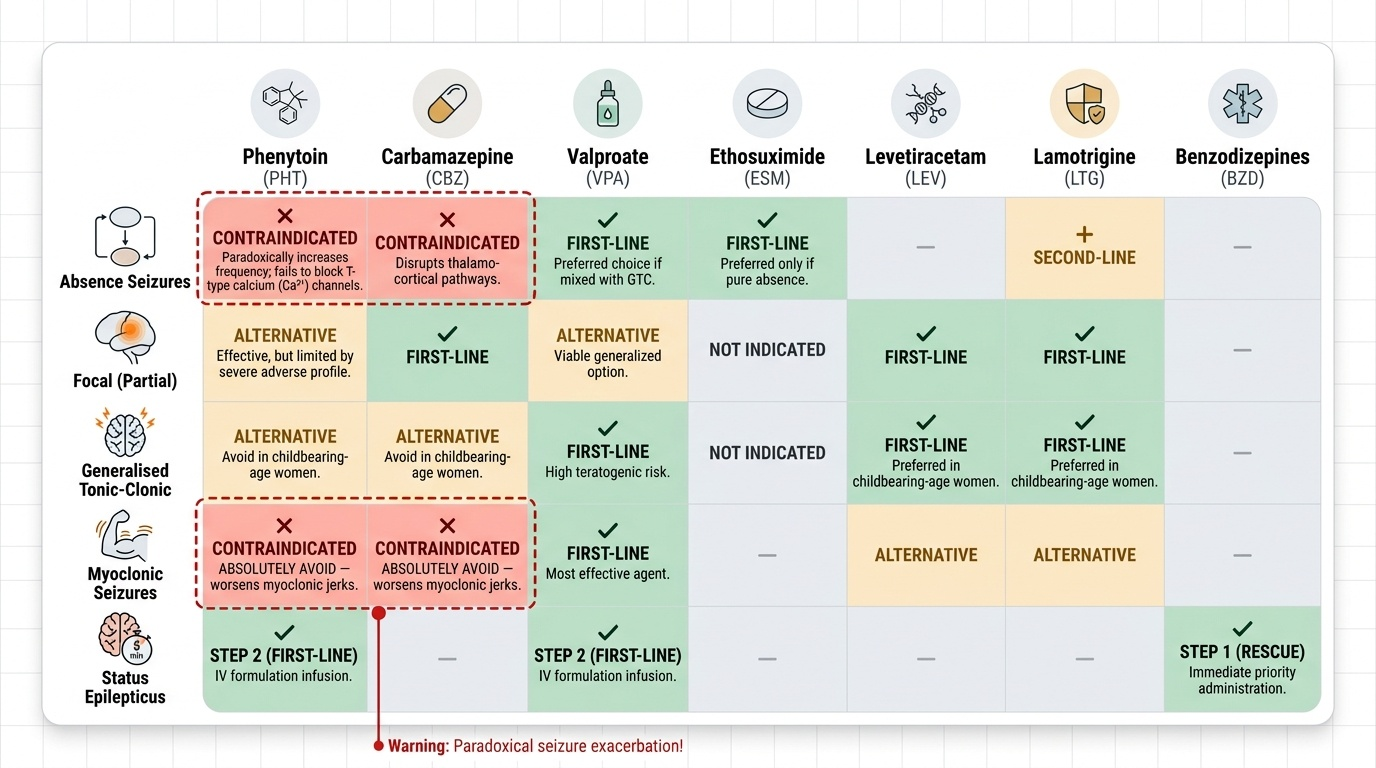
Drug-Seizure Type Matrix — Which Drug for Which Seizure
The single most clinically consequential knowledge in antiseizure pharmacology is the drug-seizure type matrix — which agents are first-line, which are adjuncts, and critically, which agents worsen specific seizure types. This matrix is the basis for rationale clinical decision-making and is a common examination scenario.
Absence seizures (childhood): first-line = ethosuximide (if absence only) or valproate (if mixed absence + generalised TC). Lamotrigine is second-line. Phenytoin and carbamazepine are contraindicated — they can paradoxically increase absence seizure frequency by disrupting thalamo-cortical inhibitory regulation without blocking the T-type Ca²⁺ current that drives absence.
Focal (partial) seizures: carbamazepine, lamotrigine, or levetiracetam are first-line. Phenytoin is effective but rarely first-line (adverse effect profile). Valproate is an option. Oxcarbazepine is an alternative to carbamazepine with fewer drug interactions.
Generalised tonic-clonic (GTC): valproate, levetiracetam, or lamotrigine. Phenytoin or carbamazepine are alternatives (but avoid in women of childbearing age when valproate is used — teratogenicity; prefer lamotrigine/levetiracetam).
Myoclonic seizures (e.g., juvenile myoclonic epilepsy — JME): valproate is most effective; levetiracetam and lamotrigine are alternatives. Phenytoin and carbamazepine WORSEN myoclonic seizures — absolutely avoid.
Status epilepticus (SE): covered in detail in the next section — stepwise BZD → IV phenytoin/valproate → anaesthetic agents.
Provided image
Status Epilepticus — Stepwise Management Plan
Status epilepticus (SE) is defined as a seizure lasting ≥5 minutes or two or more seizures without recovery of consciousness between them. Convulsive SE causes progressive neuronal injury due to metabolic exhaustion, hyperthermia, and excitotoxicity — mortality and morbidity increase with every minute of untreated SE. Immediate, stepwise pharmacological management is a clinical imperative.
The management algorithm follows three phases, determined by time elapsed:
Phase 1 — First-line (0-5 minutes, immediate): IV lorazepam (0.1 mg/kg IV, preferred — longer duration of anticonvulsant effect than diazepam) or IV diazepam (0.15-0.2 mg/kg IV or 0.5 mg/kg PR in children). IM midazolam (0.2 mg/kg) is an alternative when IV access is unavailable. BZDs work rapidly by enhancing GABA-A inhibitory tone. If the seizure stops — monitor for recurrence.
Phase 2 — Second-line (5-30 minutes, if BZD fails): IV phenytoin (20 mg/kg at ≤50 mg/min in saline — not dextrose; must monitor cardiac rhythm) or IV fosphenytoin (safer cardiovascular profile, can be given faster). Alternatively, IV valproate (25-40 mg/kg IV, preferred if phenytoin unavailable or in generalised epilepsy patients). IV levetiracetam is increasingly used as an alternative second-line agent.
Phase 3 — Refractory SE (>30-45 minutes, if second-line fails): anaesthetic doses — IV propofol infusion, IV midazolam infusion, or IV thiopental (barbiturate coma). These require intubation, ventilation, and EEG monitoring (target: burst-suppression pattern).
Supportive measures at all phases: airway protection (position, suction, intubation if needed), IV access, glucose (50 mL of 50% dextrose if hypoglycaemia suspected — but give thiamine first if alcoholism suspected), oxygen, monitoring of vital signs, investigation of underlying cause.
- 0-5 min: IV lorazepam or IV diazepam (or IM midazolam)
- 5-30 min (BZD failed): IV phenytoin/fosphenytoin OR IV valproate
- >30 min (refractory): anaesthetic agents (propofol/thiopental/midazolam infusion) + intubation + EEG
SELF-CHECK
A 9-year-old child has multiple daily episodes of brief staring and eye-blinking, each lasting about 15 seconds, with no post-ictal confusion. EEG shows 3 Hz spike-and-wave discharge. What is the first-line pharmacological treatment?
A. Phenytoin — most effective anticonvulsant for generalised seizures
B. Carbamazepine — first-line for all childhood seizures
C. Ethosuximide — first-line for absence seizures (T-type Ca²⁺ channel blocker)
D. Diazepam — benzodiazepine effective for acute seizure termination
Reveal Answer
Answer: C. Ethosuximide — first-line for absence seizures (T-type Ca²⁺ channel blocker)
The clinical picture (brief staring, eye-blinking, no post-ictal confusion, 3 Hz spike-and-wave on EEG) is typical of childhood absence epilepsy. Ethosuximide is first-line — it selectively blocks T-type Ca²⁺ channels in thalamic relay neurons, interrupting the thalamo-cortical oscillation that generates absence seizures. Valproate (broad-spectrum) is an alternative when absence coexists with other generalised seizure types. Phenytoin and carbamazepine are contraindicated — they can paradoxically worsen absence seizure frequency.
SELF-CHECK
A patient with tonic-clonic seizures has a serum phenytoin level of 25 µg/mL (therapeutic range: 10-20 µg/mL). She reports nystagmus and ataxia. What is the BEST explanation for why a small dose increment produced such a large rise in drug level?
A. Phenytoin has first-order kinetics — small changes in dose always produce proportional changes in level
B. Phenytoin has zero-order (saturation) kinetics at therapeutic concentrations — the drug-metabolising enzyme is saturated, so small dose increases produce disproportionately large rises in plasma level
C. Phenytoin undergoes auto-induction, which reduced its own metabolism at higher doses
D. Phenytoin is 100% renally excreted — any dose above renal threshold accumulates
Reveal Answer
Answer: B. Phenytoin has zero-order (saturation) kinetics at therapeutic concentrations — the drug-metabolising enzyme is saturated, so small dose increases produce disproportionately large rises in plasma level
Phenytoin undergoes zero-order (Michaelis-Menten saturation) kinetics at therapeutic concentrations — the hepatic hydroxylating enzyme (CYP2C9) becomes saturated within the therapeutic range. Above this saturation point, a small increase in dose causes a disproportionately large increase in plasma concentration, because the enzyme cannot eliminate the additional drug at a fixed rate. This makes phenytoin titration particularly hazardous and requires therapeutic drug monitoring.
SELF-CHECK
A 25-year-old woman with generalised epilepsy is planning a pregnancy. She is currently on sodium valproate. What is the most important pharmacological concern and the preferred alternative?
A. Valproate causes aplastic anaemia — switch to phenobarbitone
B. Valproate is a potent teratogen (neural tube defects, autism spectrum disorder) — switch to lamotrigine or levetiracetam with folic acid supplementation
C. Valproate interacts with folate supplements — advise against folate use during pregnancy
D. Valproate has no teratogenic risk if the dose is kept below 500 mg/day
Reveal Answer
Answer: B. Valproate is a potent teratogen (neural tube defects, autism spectrum disorder) — switch to lamotrigine or levetiracetam with folic acid supplementation
Valproate is associated with a ~1-2% risk of neural tube defects (spina bifida, anencephaly) and with autism spectrum disorder in offspring (up to 10-fold increased risk). It should be avoided in women of childbearing potential unless no safer alternative is effective. Lamotrigine or levetiracetam are the preferred alternatives in pregnancy. High-dose folic acid supplementation (5 mg/day) is recommended for ANY woman with epilepsy planning pregnancy. The risk is not dose-dependent in a way that makes 'low-dose valproate' safe — fetal risk exists across the therapeutic range.
CLINICAL PEARL
Never give phenytoin or carbamazepine in suspected absence or myoclonic epilepsy — these drugs can dramatically worsen these seizure types. Always clarify the seizure type before prescribing. In clinical practice, when in doubt use valproate (broad-spectrum) or levetiracetam (broad-spectrum, minimal interactions) while awaiting EEG confirmation. Also: valproate inhibits lamotrigine glucuronidation — if both are prescribed, lamotrigine dose must be halved (otherwise SJS risk from lamotrigine toxicity). This interaction is a classic drug-drug interaction examination question.