Page 13 of 34
PH3.5 | PH3.5 | Antidepressants and Antipsychotics — SDL Guide — SDL Guide
Learning Objectives
- Classify antidepressants (SSRIs, SNRIs, TCAs, MAOIs, others) and antipsychotics (typical/atypical) by mechanism
- Describe the pharmacokinetics, pharmacodynamics, uses, and adverse drug reactions of major agents in each class
- Devise a management plan for depressive and psychotic disorders using pharmacological principles
- Identify life-threatening adverse effects: serotonin syndrome, NMS, clozapine agranulocytosis, TCA overdose
INSTRUCTIONS
Depression and psychosis represent two of the most disabling neuropsychiatric conditions globally. Pharmacological management has transformed their prognosis, but the drugs carry serious adverse effect profiles — from the fatal cardiotoxicity of TCA overdose to the life-threatening agranulocytosis of clozapine. This module builds the pharmacological framework for safe, evidence-based treatment of depression and psychosis.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 30 (Antidepressants) and Ch 31 (Antipsychotics) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 16 (Drug Therapy of Depression and Anxiety Disorders) and Ch 14 (Antipsychotics) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old woman with major depression has been started on an SSRI by her family physician. She is also under the care of a pain specialist who adds tramadol for her chronic back pain, and a psychiatrist who adds phenelzine (an MAOI) for refractory depression, unaware of the other prescriptions. Within 24 hours she presents to the emergency department with hyperthermia (39.8°C), severe agitation, whole-body trembling, and clonus. This is serotonin syndrome — a pharmacodynamic drug interaction between her serotonergic agents that constitutes a medical emergency. It is the most dramatic example of why understanding antidepressant mechanisms and their dangerous interactions is essential clinical knowledge.
WHY THIS MATTERS
You will encounter patients on antidepressants and antipsychotics throughout every clinical rotation. You must know which SSRI is first-line for depression, why TCAs are dangerous in overdose (and are now rarely first-line), when to use clozapine (and why haematological monitoring is mandatory), how serotonin syndrome differs from neuroleptic malignant syndrome, and how to manage extrapyramidal side-effects of antipsychotics. These questions appear in clinical practice, in emergencies, and in examinations.
RECALL
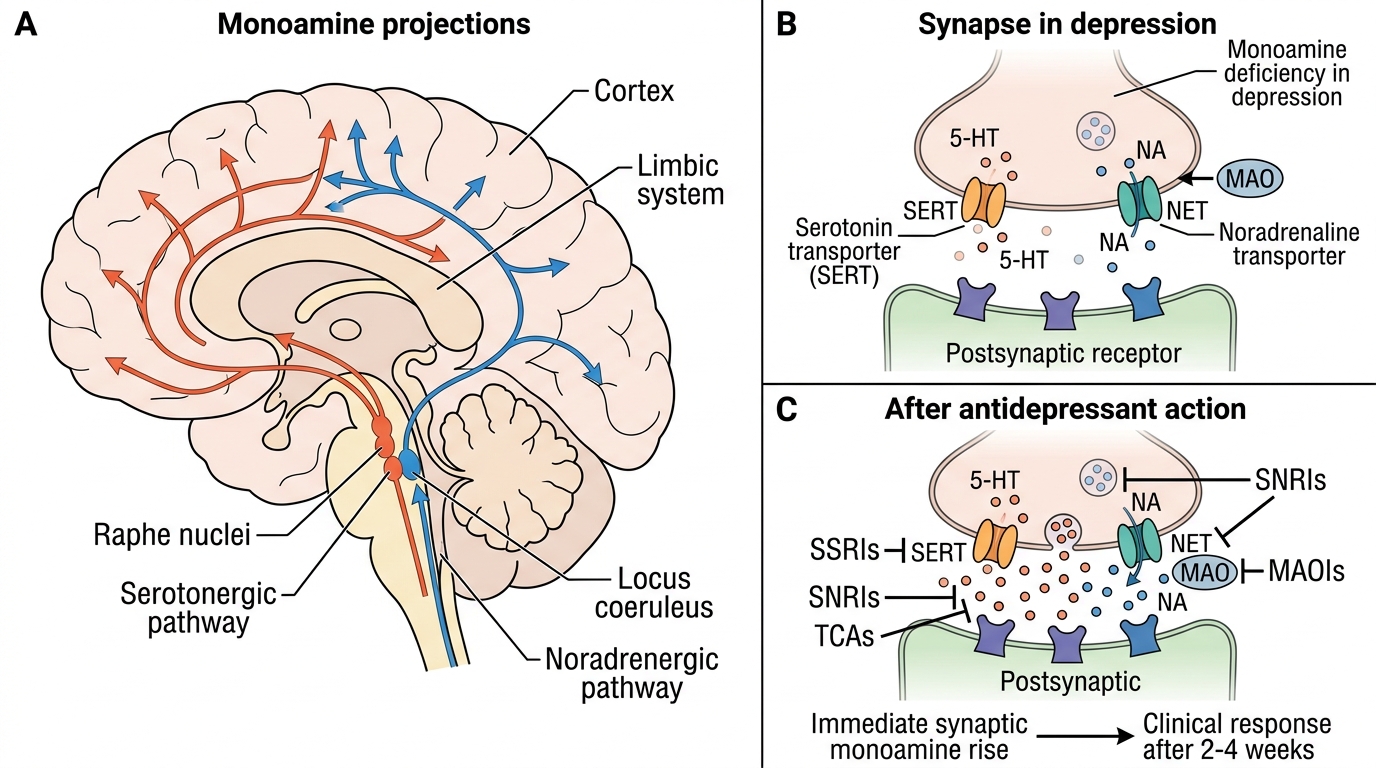
Recall from Year-1 physiology and biochemistry: monoamine neurotransmitters — serotonin (5-HT, synthesised from tryptophan via 5-HTP), noradrenaline (from tyrosine → DOPA → dopamine → NA), and dopamine (from DOPA) — are synthesised in brainstem nuclei and released into the synapse. After release, they are cleared primarily by reuptake transporters (SERT for 5-HT, NET for NA, DAT for dopamine) and metabolised by monoamine oxidase (MAO-A and MAO-B) and COMT. Recall the mesolimbic dopamine pathway (VTA → nucleus accumbens — reward) and the nigrostriatal pathway (substantia nigra → striatum — motor control) — blockade of the nigrostriatal pathway causes extrapyramidal side-effects.
Pathophysiology of Depression and Psychosis — Monoamine and Dopamine Hypotheses
Depression is pathophysiologically linked to the monoamine hypothesis: reduced functional activity of serotonin (5-HT) and noradrenaline (NA) neurotransmission in limbic-cortical circuits, particularly the prefrontal cortex, anterior cingulate, and hippocampus, is associated with the core features of depression — low mood, anhedonia, cognitive slowing, and neurovegetative symptoms (sleep, appetite, psychomotor disturbance). Evidence comes from: reserpine (depletes monoamine stores) causing depression; all effective antidepressants increase monoaminergic transmission; the delay in clinical effect (2-4 weeks despite immediate monoamine increase at the synapse) suggests downstream neuroplastic changes (BDNF upregulation, hippocampal neurogenesis) are the actual therapeutic mechanism.
Psychosis/schizophrenia is linked to the dopamine hypothesis: hyperactivity of the mesolimbic dopamine pathway (VTA → nucleus accumbens) generates positive symptoms (hallucinations, delusions, thought disorder — excess dopamine at D2 receptors); deficiency in the mesocortical pathway (VTA → prefrontal cortex) underlies negative symptoms (flat affect, alogia, avolition, social withdrawal). All effective antipsychotics block D2 receptors (or D2 + 5HT2A). The nigrostriatal pathway (substantia nigra → striatum) — when blocked by antipsychotics — produces extrapyramidal side-effects (EPS), including drug-induced parkinsonism.
IMPORTANT for internal consistency: antidepressants increase monoamine availability (block reuptake or block MAO); antipsychotics reduce dopaminergic excess (block D2). These are opposing pharmacological strategies for different target circuits — they are not interchangeable and are clearly distinct classes.
Monoamine Pathways and Antidepressant Mechanisms
Goals of Antidepressant and Antipsychotic Therapy
For depression, the therapeutic goals are: (1) response (≥50% reduction in symptom score), (2) remission (full symptom resolution), and (3) sustained recovery (maintained remission with prevention of relapse). Treatment must be continued for at least 6 months after remission because early discontinuation leads to relapse in >50% of patients. The monoamine mechanism explains a critical practical reality: the delay between starting an antidepressant (immediate synapse-level monoamine rise) and clinical response (2-4 weeks) — patients must be counselled about this delay.
For psychosis/schizophrenia, goals include: (1) acute phase — control of positive symptoms (agitation, hallucinations, aggression) with rapid-onset agents, (2) stabilisation — reduce positive and negative symptoms to functional baseline, (3) maintenance — prevent relapse using sustained antipsychotic therapy (often years). A critical safety constraint is that both classes of drugs carry life-threatening adverse effects that must be proactively monitored:
- Antidepressants: serotonin syndrome (if combined with other serotonergic agents or MAOIs), TCA cardiotoxicity in overdose
- Antipsychotics: neuroleptic malignant syndrome (NMS), clozapine agranulocytosis (mandatory WBC monitoring)
These safety constraints directly shape the management plan — they are not afterthoughts to the treatment choice.
Classification of Antidepressants and Antipsychotics
Antidepressants are classified by their molecular mechanism of action — this determines their adverse effect profile and dangerous interactions:
- SSRIs (Selective Serotonin Reuptake Inhibitors): fluoxetine, sertraline, escitalopram, paroxetine, fluvoxamine — block SERT (serotonin transporter) selectively. First-line for depression and most anxiety disorders.
- SNRIs (Serotonin-Noradrenaline Reuptake Inhibitors): venlafaxine, duloxetine — block both SERT and NET. First-line for depression and neuropathic pain.
- TCAs (Tricyclic Antidepressants): amitriptyline, imipramine, clomipramine — block 5-HT + NA reuptake + anticholinergic + antihistamine + α₁-adrenoceptor block + Na⁺-channel block. Effective but dangerous in overdose; now second or third-line.
- MAOIs (Monoamine Oxidase Inhibitors): phenelzine (irreversible, non-selective MAO-A+B); tranylcypromine (irreversible); moclobemide (reversible, selective MAO-A = RIMA). Reserved for TCA/SSRI-refractory depression.
- Others: mirtazapine (NaSSA — blocks α₂ autoreceptors + 5HT2/3 antagonist; sedating, weight gain), bupropion (NDRI — noradrenaline/dopamine reuptake inhibitor; used in depression + smoking cessation; lowers seizure threshold).
Antipsychotics are classified as:
1. Typical (1st-generation): chlorpromazine (low potency, sedating), haloperidol (high potency, high EPS) — primarily D2 receptor blockers.
2. Atypical (2nd-generation): clozapine, olanzapine, risperidone, quetiapine, aripiprazole — block D2 + 5HT2A (and other receptors). Lower EPS risk than typicals; higher metabolic side-effect risk.