Page 14 of 34
PH3.5 | PH3.5 | Antidepressants and Antipsychotics — SDL Guide — SDL Guide (Part 2)
Antidepressants — PK, PD, Uses, and ADRs
SSRIs are the first-line pharmacological treatment for major depressive disorder, generalised anxiety disorder, panic disorder, OCD, PTSD, and social anxiety disorder. Their selectivity for SERT reduces the non-serotonin-related adverse effects of older antidepressants. ADRs: GI effects (nausea, diarrhoea — usually transient), sexual dysfunction (reduced libido, anorgasmia — common and often not spontaneously reported), insomnia or somnolence, serotonin discontinuation syndrome (dizziness, 'brain zaps', irritability on abrupt cessation — taper doses on stopping). Fluoxetine has the longest t½ (and active metabolite norfluoxetine) — least discontinuation syndrome. SSRIs combined with MAOIs or pethidine/tramadol can produce serotonin syndrome (see below).
SNRIs share SSRI-class effects plus noradrenergic effects: effective for depression and neuropathic pain (duloxetine is approved for diabetic neuropathic pain). ADR additions over SSRIs: hypertension (NA-mediated), urinary hesitancy.
TCAs (amitriptyline, imipramine, clomipramine): more effective for severe depression and neuropathic pain than SSRIs in some patients, but multiple receptor actions produce: anticholinergic effects (dry mouth, constipation, urinary retention, tachycardia, glaucoma precipitation), antihistamine effects (sedation, weight gain), α₁-block (postural hypotension), Na⁺-channel block (QRS widening, ventricular arrhythmias — FATAL IN OVERDOSE). TCA overdose is a medical emergency: sodium bicarbonate IV (alkalinisation reverses Na⁺-channel block) + supportive care. TCAs are absolutely contraindicated in patients at risk for suicide due to their lethal overdose profile.
MAOIs: phenelzine and tranylcypromine irreversibly inhibit both MAO-A and MAO-B — dangerous tyramine interaction ('cheese reaction'): tyramine in food (aged cheese, red wine, yeast extract, fermented meats) is normally metabolised by intestinal/hepatic MAO-A; with MAO inhibited, dietary tyramine is absorbed → stimulates sympathetic nerve endings → massive noradrenaline release → hypertensive crisis (severe occipital headache, diaphoresis, hypertension, risk of stroke/haemorrhage). Moclobemide (RIMA) is reversible and selective for MAO-A — tyramine can competitively displace it from MAO-A, making the tyramine interaction much less severe. MAOIs require a washout period of at least 14 days before starting SSRIs/TCAs (and vice versa); fluoxetine requires 5 weeks washout before starting an MAOI (due to long t½ of norfluoxetine).
Mirtazapine: blocks presynaptic α₂ autoreceptors (increases NA and 5-HT release) + 5-HT₂ and 5-HT₃ antagonism (reduces GI side-effects). Sedating (H₁ block) and promotes appetite/weight gain — useful in depressed patients with insomnia and weight loss. Lower serotonin syndrome risk than SSRIs.
| Class | Example | Mechanism | Key ADRs |
|---|---|---|---|
| SSRI | Fluoxetine, Sertraline | SERT block | Sexual dysfunction, GI, discontinuation syndrome |
| SNRI | Venlafaxine, Duloxetine | SERT + NET block | Hypertension, urinary hesitancy |
| TCA | Amitriptyline | 5HT+NA + anticholinergic + Na-block | Fatal overdose (arrhythmia), anticholinergic effects |
| MAOI (irreversible) | Phenelzine | MAO-A+B inhibition | Tyramine hypertensive crisis, multiple drug interactions |
| RIMA | Moclobemide | Reversible MAO-A inhibition | Safer tyramine interaction |
| NaSSA | Mirtazapine | α₂-block + 5HT2/3 block | Sedation, weight gain |
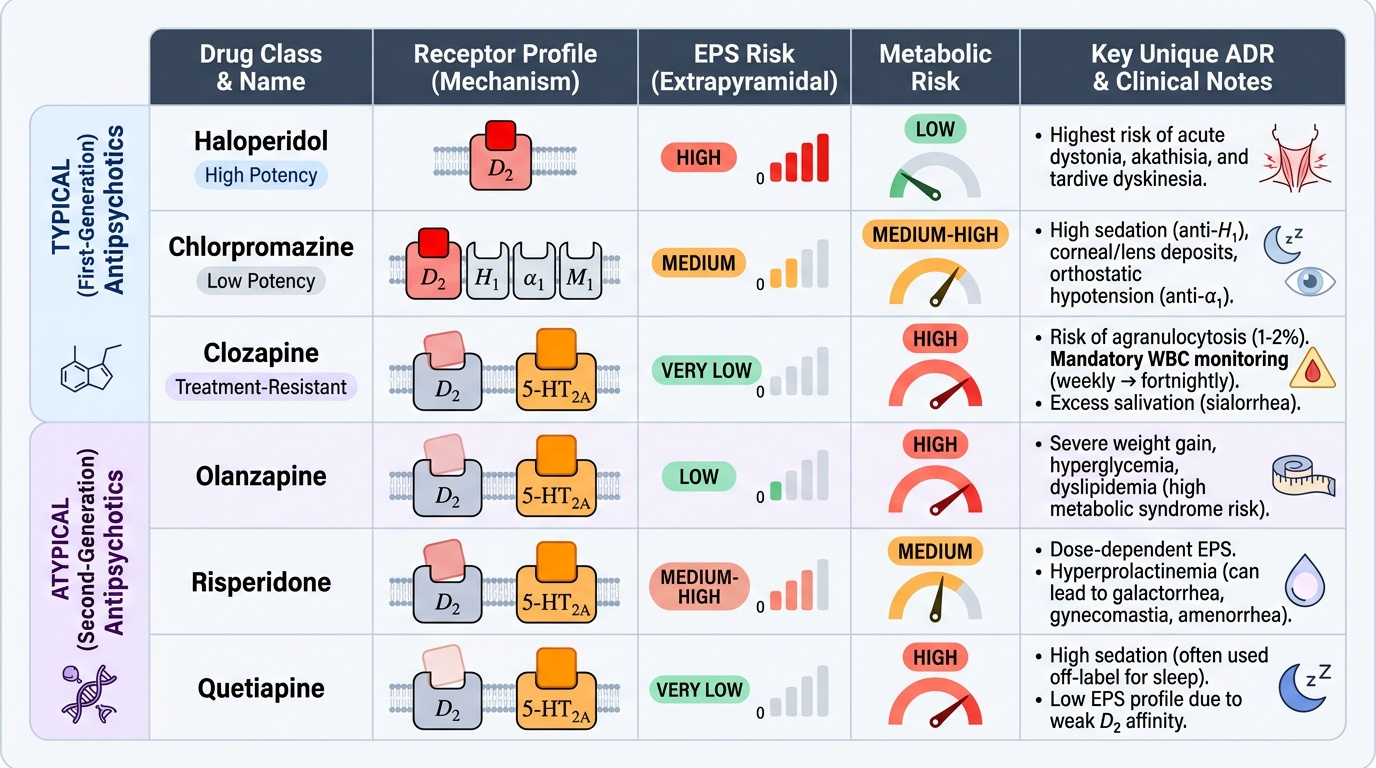
Antipsychotics — PK, PD, Uses, and ADRs
Typical antipsychotics (chlorpromazine, haloperidol, fluphenazine) act primarily by blocking D2 receptors across all four dopamine pathways: mesolimbic (therapeutic — reduces positive symptoms), mesocortical (worsens negative symptoms), nigrostriatal (EPS), and tuberoinfundibular (hyperprolactinaemia → galactorrhoea, menstrual irregularities). High-potency typicals (haloperidol) have high EPS risk; low-potency typicals (chlorpromazine) have more sedation and anticholinergic effects.
Extrapyramidal side-effects (EPS) of typical antipsychotics:
- Acute dystonia (hours-days): painful muscle spasm (torticollis, oculogyric crisis) — treat with IM/IV anticholinergic (benztropine or trihexyphenidyl)
- Akathisia (days-weeks): subjective restlessness — treat with propranolol or BZD
- Drug-induced parkinsonism (weeks-months): tremor, rigidity, bradykinesia — treat with anticholinergics (NOT levodopa, which does not help drug-induced parkinsonism and is not used for this indication)
- Tardive dyskinesia (TD) (months-years): repetitive involuntary orofacial movements — largely irreversible; treat with VMAT2 inhibitors (valbenazine, deutetrabenazine); prevent by using lowest effective dose for shortest time
Neuroleptic malignant syndrome (NMS): rare but life-threatening reaction to antipsychotics — tetrad: hyperthermia + muscle rigidity + autonomic instability + altered consciousness. Mechanism: dopamine receptor blockade in the hypothalamus and basal ganglia. Distinguish from serotonin syndrome (which features clonus and hyperreflexia rather than rigidity). Treatment: stop antipsychotic, supportive care, dantrolene (muscle relaxant, as in MH), bromocriptine (D2 agonist).
Atypical antipsychotics (clozapine, olanzapine, risperidone, quetiapine, aripiprazole) block D2 + 5HT2A receptors (and various others). Lower EPS (less nigrostriatal D2 blockade relative to mesolimbic), more metabolic side-effects:
- Clozapine: most effective antipsychotic overall; reserved for treatment-resistant schizophrenia (failed ≥2 antipsychotic trials). Risk of agranulocytosis (~1-2%) — mandatory WBC monitoring (weekly for 18 weeks, then fortnightly while on treatment; stop if WBC <3,000 or ANC <1,500). Also: sedation, weight gain, metabolic syndrome, salivation (paradoxical — muscarinic agonism), seizures at high doses, myocarditis.
- Olanzapine: effective, high metabolic risk (weight gain, diabetes, dyslipidaemia). IM formulation for acute agitation.
- Risperidone: moderate EPS risk (higher than other atypicals at high doses), raised prolactin.
- Quetiapine: sedating (useful at night), low EPS and low prolactin — frequently used in elderly with dementia-related psychosis.
Provided image
Management Plans for Depression and Psychotic Disorders
Depression management plan:
First-line pharmacological treatment: SSRI (e.g., sertraline or escitalopram). Counsel the patient that clinical response takes 2-4 weeks — early discontinuation is the most common cause of treatment failure. Assess response at 4-6 weeks: if partial response, increase dose; if no response, switch to another SSRI or to an SNRI.
If two adequate SSRI trials fail: escalate to augmentation (add lithium, atypical antipsychotic, or buspirone) or switch to SNRI → mirtazapine → TCA (with adequate patient safety assessment — avoid in suicidal patients). MAOIs are reserved for TCA-refractory cases with appropriate washout.
Duration: continue for ≥6 months after remission for a first depressive episode; 2 years after a second episode; indefinite for recurrent (3+) episodes.
Crucial safety rule: do not co-prescribe two serotonergic agents without careful assessment — specifically, never combine an SSRI (or SNRI or TCA) with an MAOI. Washout periods must be observed.
Psychosis/schizophrenia management plan:
Acute phase: IM haloperidol (or IM olanzapine) for rapid control of agitation and psychosis. Oral lorazepam as an adjunct to reduce agitation.
Stabilisation and maintenance: oral atypical antipsychotic (olanzapine, risperidone, quetiapine, amisulpride) — selected based on metabolic risk, EPS risk, and patient preference. Continue maintenance for ≥2 years after first episode; longer for recurrent psychosis.
Treatment-resistant schizophrenia (failed ≥2 adequate antipsychotic trials): clozapine — mandatory WBC monitoring protocol must be in place before initiating.
Poor adherence: depot (long-acting injectable) antipsychotics (fluphenazine decanoate, risperidone microspheres, paliperidone palmitate) given every 2-4 weeks — bypass the need for daily oral medication.
- Depression: SSRI first-line → 4-6 week assessment → switch/augment → TCA/MAOI last resort
- Psychosis acute: IM haloperidol/olanzapine; maintenance: oral atypical; resistant: clozapine
- Never SSRI + MAOI concurrently; 14-day washout between them (5 weeks for fluoxetine)
SELF-CHECK
A patient on phenelzine (an irreversible MAOI) for depression eats a large portion of aged cheddar cheese at a dinner party. Within 30 minutes she develops a severe occipital headache, flushing, palpitations, and a BP of 220/130 mmHg. What is the mechanism of this reaction?
A. Phenelzine directly stimulates α₁ receptors in blood vessel walls, raising blood pressure
B. Dietary tyramine, normally metabolised by intestinal MAO-A, is absorbed intact and releases noradrenaline from sympathetic nerve terminals — causing a hypertensive crisis (tyramine reaction)
C. Phenelzine inhibits CYP2D6, preventing tyramine hepatic metabolism and causing its accumulation
D. Phenelzine blocks COMT, preventing adrenaline breakdown and causing a catecholamine surge
Reveal Answer
Answer: B. Dietary tyramine, normally metabolised by intestinal MAO-A, is absorbed intact and releases noradrenaline from sympathetic nerve terminals — causing a hypertensive crisis (tyramine reaction)
This is the classic MAOI tyramine ('cheese') reaction. Tyramine is a monoamine found in fermented/aged foods. Normally, dietary tyramine is metabolised by MAO-A in the gut wall and liver before reaching systemic circulation. Phenelzine irreversibly inhibits MAO-A (and MAO-B) — tyramine escapes this first-pass metabolism, enters the circulation, and triggers massive noradrenaline release from sympathetic nerve endings (indirect sympathomimetic effect), causing severe hypertension. Management: IV phentolamine (α-blocker) or IV labetalol. Moclobemide (reversible MAO-A inhibitor = RIMA) has a much safer tyramine interaction because dietary tyramine can displace moclobemide from MAO-A.
SELF-CHECK
A patient on clozapine for treatment-resistant schizophrenia develops fever and sore throat on routine follow-up. WBC is 2,100/mm³ and neutrophils are 800/mm³. What is the appropriate pharmacological action?
A. Reduce the dose of clozapine and add a prophylactic antibiotic
B. Stop clozapine immediately — agranulocytosis; do not rechallenge
C. Switch to haloperidol and add G-CSF to stimulate WBC production
D. Continue clozapine but increase WBC monitoring to weekly
Reveal Answer
Answer: B. Stop clozapine immediately — agranulocytosis; do not rechallenge
This presentation is consistent with clozapine-induced agranulocytosis (WBC <3,000, neutrophils <1,500). Clozapine must be stopped immediately — this is a mandatory criterion in all monitoring protocols. Agranulocytosis risk with clozapine is ~1-2% (compared to <0.1% with other antipsychotics). The patient must not be rechallenged with clozapine, as rechallenge carries extreme risk of fatal agranulocytosis. Supportive management includes G-CSF in severe cases and treating any infections. All patients starting clozapine must be registered with the manufacturer's monitoring programme; WBC is checked weekly for 18 weeks, then fortnightly.
SELF-CHECK
How does serotonin syndrome differ pharmacologically from neuroleptic malignant syndrome (NMS)?
A. Serotonin syndrome is caused by excess dopamine; NMS is caused by excess serotonin
B. Serotonin syndrome (excess 5HT: agitation, clonus, hyperreflexia, diaphoresis) is caused by serotonergic drugs (SSRI+MAOI etc.); NMS (dopamine receptor blockade: hyperthermia, lead-pipe rigidity, autonomic instability) is caused by antipsychotics
C. They are clinically identical syndromes caused by different drug classes but managed the same way
D. Serotonin syndrome exclusively causes hypotension; NMS exclusively causes hypertension
Reveal Answer
Answer: B. Serotonin syndrome (excess 5HT: agitation, clonus, hyperreflexia, diaphoresis) is caused by serotonergic drugs (SSRI+MAOI etc.); NMS (dopamine receptor blockade: hyperthermia, lead-pipe rigidity, autonomic instability) is caused by antipsychotics
Serotonin syndrome results from excess serotonergic activity (e.g., SSRI + MAOI combination) and presents with agitation, confusion, clonus (repetitive muscle contractions), tremor, hyperreflexia, diaphoresis, hyperthermia, and tachycardia — the hallmarks are neuromuscular hyperexcitability (clonus). NMS results from dopamine receptor blockade by antipsychotics and presents with hyperthermia, 'lead-pipe' muscle rigidity (not clonus), autonomic instability, and altered consciousness — the hallmark is rigidity. Treatment differs: serotonin syndrome = stop serotonergic agents, cyproheptadine (5HT antagonist); NMS = stop antipsychotic, dantrolene (muscle relaxant), bromocriptine.
CLINICAL PEARL
Never start an SSRI or TCA while a patient is on an MAOI — or vice versa — without the appropriate washout period. The minimum washout between an MAOI and an SSRI (or vice versa) is 14 days. Fluoxetine requires 5 weeks washout before starting an MAOI (because its active metabolite norfluoxetine has a half-life of 4-16 days). This interaction causes serotonin syndrome and is potentially fatal. Also remember: TCA overdose triad is anticholinergic + arrhythmia + seizures — treat with sodium bicarbonate IV (1-2 mEq/kg to alkalinise plasma) to reverse the Na⁺-channel block causing QRS widening and ventricular arrhythmias.