Page 23 of 34
PH3.8 | PH3.8 | Alcohol Toxicity Management — SDL Guide — SDL Guide (Part 2)
Methanol Poisoning — PK, PD, and Management
Clinical presentation of methanol poisoning: the latent period of 6-24 hours (longer if ethanol was concurrently consumed) is followed by: nausea, vomiting, epigastric pain; CNS depression (headache, dizziness → coma); visual disturbance (blurring, photophobia, 'snowfield' vision → permanent blindness — due to formate toxicity to the optic nerve); high anion-gap metabolic acidosis (formate accumulation — serum HCO₃ low, pH low, anion gap high). The combination of metabolic acidosis and visual symptoms in a patient with alcohol/illicit spirit exposure is the diagnostic hallmark.
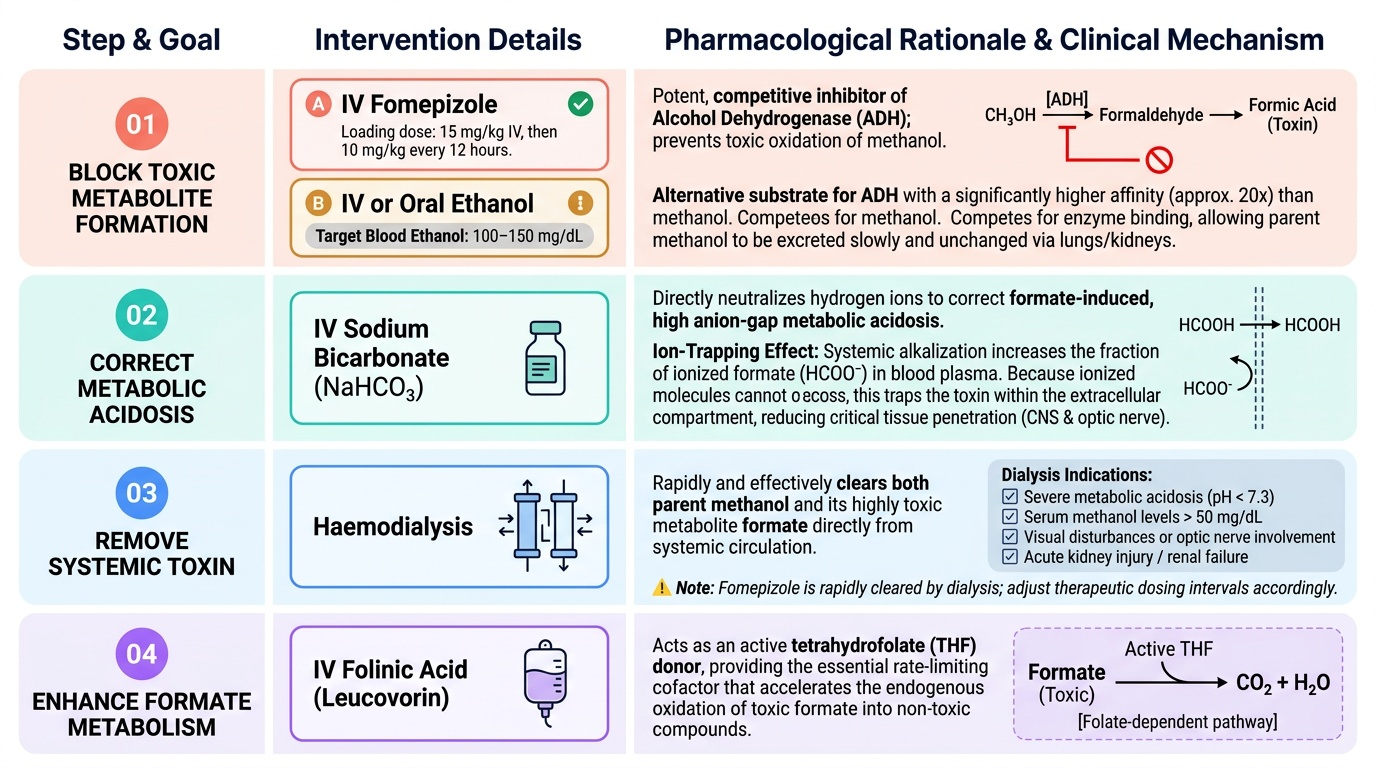
Stepwise pharmacological management:
Step 1 — Block further toxic metabolite formation: IV fomepizole (15 mg/kg loading dose IV, then 10 mg/kg every 12h) — ADH inhibitor, prevents further methanol → formaldehyde/formate conversion. If fomepizole unavailable: IV or oral ethanol (loading dose to achieve blood ethanol 100-150 mg/dL; maintain with infusion) — ethanol competes with methanol for ADH binding (higher affinity), directing ADH to metabolise ethanol while methanol is slowly excreted.
Step 2 — Correct metabolic acidosis: IV sodium bicarbonate — corrects the formate-induced high anion-gap metabolic acidosis; also reduces tissue distribution of formate (ionised at alkaline pH).
Step 3 — Remove toxin: Haemodialysis — removes both methanol and formate from the blood; indicated for severe acidosis (pH <7.3), renal failure, visual symptoms, high serum methanol level (>50 mg/dL). If fomepizole is being used, the dose must be adjusted during dialysis (rapidly cleared).
Step 4 — Enhance formate metabolism: IV folinic acid (leucovorin) — provides tetrahydrofolate cofactor needed for formate oxidation to CO₂; reduces formate accumulation.
Provided image
Chronic Ethanol Intoxication — Pharmacology and Management
Mechanism of ethanol's CNS effects: ethanol potentiates GABA-A receptors (increases Cl⁻ conductance — similar to BZDs, explaining cross-tolerance) and inhibits NMDA receptors (reduces glutamate-mediated excitation). This dual action explains ethanol's dose-dependent CNS effects: anxiolysis and disinhibition at low doses → sedation and incoordination → coma and respiratory depression at high doses.
Tolerance and dependence: chronic ethanol exposure causes: (1) GABA-A receptor down-regulation (reduced sensitivity — requires more ethanol for the same sedative effect); (2) NMDA receptor upregulation (more excitatory tone). When ethanol is abruptly withdrawn, the down-regulated GABA-A and upregulated NMDA create a state of neuronal hyperexcitability — withdrawal syndrome.
Alcohol withdrawal syndrome timeline and management:
- 6-24 hours: tremor, anxiety, nausea, diaphoresis, tachycardia — treat with oral BZD (diazepam or chlordiazepoxide)
- 6-48 hours: withdrawal seizures (generalised tonic-clonic) — treat with IV diazepam (10-20 mg); prevent with scheduled BZD tapering
- 48-96 hours: delirium tremens (DT) — severe autonomic instability, hallucinations, confusion; life-threatening; IV diazepam or lorazepam infusion; high-dependency unit care
Wernicke's encephalopathy (WE): thiamine (vitamin B₁) deficiency, common in chronic alcoholism (poor dietary intake + impaired absorption + increased utilisation). Classical triad: ophthalmoplegia + ataxia + confusion. Critical management rule: give parenteral thiamine BEFORE glucose in any confused/comatose alcoholic. Rationale: glucose metabolism requires thiamine; administering glucose without replacing thiamine first in a thiamine-depleted patient will consume the remaining thiamine stores, precipitating or worsening WE. Untreated WE → Korsakoff's psychosis (irreversible anterograde amnesia, confabulation).
Disulfiram: irreversible inhibitor of ALDH. When a patient on disulfiram ingests any alcohol, acetaldehyde accumulates → disulfiram-ethanol reaction (flushing, headache, palpitations, nausea, vomiting, hypotension, tachycardia, dyspnoea). This aversive reaction serves as a deterrent — the patient knows any alcohol ingestion will cause them to feel acutely unwell. Requires high patient motivation and supervision. Warn patients about hidden alcohol in food, medicines (mouthwash, cough syrup), and topical preparations. Naltrexone reduces the reward of drinking (blocks opioid-mediated mesolimbic dopamine activation); acamprosate reduces abstinence symptoms.
SELF-CHECK
A patient presents with severe metabolic acidosis, visual blurring, and a history of drinking illicit liquor at a festival. Methanol poisoning is suspected. What is the MOST IMPORTANT immediate pharmacological intervention and its mechanism?
A. IV sodium bicarbonate — correct the metabolic acidosis and prevent formate distribution
B. IV fomepizole (or oral ethanol if unavailable) — competitively inhibit alcohol dehydrogenase to prevent further conversion of methanol to the toxic metabolite formic acid
C. IV diazepam — prevent seizures from methanol-induced CNS excitation
D. Haemodialysis — the only intervention that removes methanol from the circulation
Reveal Answer
Answer: B. IV fomepizole (or oral ethanol if unavailable) — competitively inhibit alcohol dehydrogenase to prevent further conversion of methanol to the toxic metabolite formic acid
The most critical early pharmacological intervention in methanol poisoning is to STOP further formation of the toxic metabolite (formic acid) by inhibiting alcohol dehydrogenase (ADH). Fomepizole (IV, first-line ADH inhibitor) or ethanol (competitive ADH substrate if fomepizole unavailable — target blood ethanol 100-150 mg/dL) achieves this. Sodium bicarbonate corrects existing acidosis but does not prevent new formate formation. Haemodialysis removes methanol and formate but should accompany, not replace, ADH inhibition. The earlier fomepizole is given, the less formate is formed and the less optic nerve damage occurs.
SELF-CHECK
A 45-year-old man with chronic alcoholism is found unconscious and brought to the emergency department. Blood glucose is 2.1 mmol/L. A colleague wants to immediately push IV dextrose. What must you do FIRST and why?
A. Push IV dextrose immediately — hypoglycaemia causes brain damage and must be corrected first
B. Give IM/IV thiamine first, THEN give IV dextrose — glucose without thiamine in a thiamine-depleted alcoholic precipitates or worsens Wernicke's encephalopathy
C. Give IV naloxone first — opioid co-ingestion is common in alcoholics
D. Get a blood glucose — if >4 mmol/L, no need for glucose; if <4 mmol/L, push dextrose without thiamine
Reveal Answer
Answer: B. Give IM/IV thiamine first, THEN give IV dextrose — glucose without thiamine in a thiamine-depleted alcoholic precipitates or worsens Wernicke's encephalopathy
In a thiamine-depleted patient (chronic alcoholism), administering glucose without prior thiamine can precipitate or worsen Wernicke's encephalopathy. The mechanism: glucose metabolism in the brain requires thiamine (as a cofactor for pyruvate dehydrogenase and alpha-ketoglutarate dehydrogenase). In a borderline-thiamine-depleted patient, the metabolic demand of glucose administration consumes remaining thiamine stores, tipping the balance into deficiency. Therefore, parenteral thiamine (IV/IM, minimum 100-200 mg) MUST be given BEFORE or simultaneously with glucose in any confused or comatose alcoholic. Thiamine is safe, inexpensive, and the delay of seconds to minutes required for its administration is justified by prevention of irreversible Wernicke-Korsakoff syndrome.
SELF-CHECK
A patient with alcohol use disorder is started on disulfiram as part of a supervised deterrent programme. What is the mechanism of the disulfiram-ethanol reaction, and what warning must be given to the patient?
A. Disulfiram blocks alcohol dehydrogenase, preventing ethanol metabolism — ethanol accumulates and causes direct CNS toxicity
B. Disulfiram blocks aldehyde dehydrogenase (ALDH) — when ethanol is consumed, acetaldehyde accumulates causing flushing, tachycardia, nausea, and hypotension; even small amounts of alcohol in food or medicines can trigger the reaction
C. Disulfiram is a μ-opioid antagonist that blocks the rewarding effects of alcohol without causing any physical reaction
D. Disulfiram causes severe sedation when combined with alcohol, making the patient too drowsy to continue drinking
Reveal Answer
Answer: B. Disulfiram blocks aldehyde dehydrogenase (ALDH) — when ethanol is consumed, acetaldehyde accumulates causing flushing, tachycardia, nausea, and hypotension; even small amounts of alcohol in food or medicines can trigger the reaction
Disulfiram is an irreversible inhibitor of aldehyde dehydrogenase (ALDH). Normally, ethanol → acetaldehyde (by ADH) → acetate (by ALDH). With ALDH blocked, acetaldehyde accumulates in the blood after any alcohol ingestion — causing the disulfiram-ethanol reaction: flushing, headache, palpitations, nausea, vomiting, hypotension, and tachycardia. This is an aversive pharmacodynamic deterrent. Patients must be warned that the reaction can be triggered by even small alcohol amounts found in mouthwash, cough syrups, food marinades, and topical preparations — not just by drinking.
CLINICAL PEARL
Thiamine before glucose — always, in every confused or comatose alcoholic. This rule has no exceptions. Glucose first in a thiamine-depleted patient consumes the remaining thiamine to metabolise the glucose, precipitating acute Wernicke's encephalopathy (ophthalmoplegia, ataxia, confusion → coma). IV thiamine is given as 200-500 mg IV infusion over 30 minutes; IM is an alternative. Thiamine is extremely safe — there is no reason not to give it. The consequences of omitting it — irreversible Korsakoff's psychosis (anterograde amnesia, confabulation) — are devastating.