Page 11 of 33
PH4.7 | PH4.7 | Hypertension Pharmacotherapy — SDL Guide
Learning Objectives
- Classify antihypertensive drug classes by mechanism and describe the pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of each.
- Devise a pharmacological management plan for hypertension with comorbidities including diabetes mellitus, CKD, heart failure, and pregnancy.
- Distinguish hypertensive emergency from hypertensive urgency and select appropriate agents for each.
- Identify absolute contraindications to specific antihypertensive drug classes in pregnancy and other high-risk settings.
INSTRUCTIONS
Hypertension affects over 1 billion people globally and is the single leading cause of premature cardiovascular death. Despite highly effective drugs, blood pressure control rates remain below 50% in most populations — partly because of too many choices, partly because of drug inertia, and often because of missed comorbidity-driven opportunities to select the drug that does double duty. This SDL provides the pharmacological framework for rational antihypertensive prescribing: mechanism by mechanism, comorbidity by comorbidity, and emergency by emergency.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 39 (Antihypertensive Drugs) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th ed., Ch. 27 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old woman is rushed to the emergency department by her family. She has had a severe headache since this morning and is confused. BP is 210/130 mmHg. Fundoscopy shows papilloedema and flame-shaped haemorrhages (hypertensive retinopathy Grade IV). She is 28 weeks pregnant. ECG shows left ventricular hypertrophy changes. You need to lower her blood pressure urgently — but which drug do you choose? The wrong answer kills her or her baby. Meanwhile, her sister, also hypertensive, calls for advice: her home BP monitor reads 185/115 mmHg but she has no symptoms. Does she need the same emergency treatment? How are these two situations different?
WHY THIS MATTERS
Hypertension is the commonest chronic non-communicable disease managed in outpatient settings across all specialties — not just cardiology. Every internist, obstetrician, nephrologist, neurologist, and general physician initiates, adjusts, and troubleshoots antihypertensive therapy. The stakes are asymmetric: undertreated hypertension kills through stroke, MI, and kidney failure over years; inappropriately treated hypertensive urgency causes watershed cerebral infarction and renal failure within hours. The pharmacological choices in pregnancy carry the additional responsibility of fetal safety — getting it wrong causes neonatal harm or death. This SDL builds the decision framework that will guide thousands of clinical encounters throughout your career.
RECALL
Recall the haemodynamic equation: Blood pressure = Cardiac output × Total peripheral resistance. Every antihypertensive drug class acts by reducing CO, TPR, or both.
- Cardiac output = heart rate × stroke volume; reduced by: beta-blockers (↓HR, ↓contractility), diuretics (↓plasma volume → ↓preload → ↓SV).
- Total peripheral resistance = vasomotor tone of arterioles; reduced by: CCBs (block Ca²⁺ entry → vasodilation), ACEi/ARBs (↓Ang II → reduce vasoconstriction), α1-blockers (block adrenergic vasoconstriction), direct vasodilators (hydralazine, nitroprusside).
- Sympathetic nervous system (PY): α1 stimulation → vasoconstriction (arterioles, veins); β1 stimulation → ↑HR + ↑contractility; β2 stimulation → bronchodilation + vasodilation. Adrenergic drugs modulate these pathways.
- Target organ damage in hypertension: Brain — hypertensive encephalopathy, ischaemic stroke, haemorrhagic stroke; Heart — LV hypertrophy, coronary artery disease, HF; Kidneys — nephrosclerosis, CKD, ESRD; Eyes — retinopathy grades I–IV (Keith-Wagener-Barker).
Pathophysiology of Hypertension: The Pressure–Damage Cascade
Hypertension (sustained blood pressure ≥140/90 mmHg) is defined by the persistent elevation of systolic and/or diastolic pressure beyond levels associated with end-organ protection. The vast majority (~90–95%) of cases are essential (primary) hypertension, in which no single reversible cause is identified; the remainder are secondary hypertension — caused by identifiable conditions including primary hyperaldosteronism (most common secondary cause), renal parenchymal disease, renovascular disease (renal artery stenosis), phaeochromocytoma, Cushing's syndrome, aortic coarctation, and primary hypothyroidism. Secondary causes must be considered in: young patients, resistant hypertension (BP uncontrolled on 3+ drugs including a diuretic), hypokalaemia (suggests hyperaldosteronism), renal bruits, or rapid onset.
In essential hypertension, three pathophysiological mechanisms predominate in varying proportions across patients: (1) increased sympathetic nervous system activity — elevated catecholamines increase HR and vasoconstriction; (2) RAAS overactivation — Ang II drives vasoconstriction, aldosterone-mediated Na retention, and vascular remodelling; (3) impaired renal pressure-natriuresis — the kidney fails to excrete adequate sodium at normal pressures, requiring a higher pressure setpoint to achieve equilibrium. Most antihypertensive drugs target one or more of these mechanisms.
Untreated or inadequately treated hypertension causes progressive target-organ damage through multiple mechanisms: (1) in the brain — accelerated atherosclerosis + small-vessel lipohyalinosis → lacunar infarcts, white matter disease; acute BP surges rupture Charcot-Bouchard aneurysms → intracerebral haemorrhage; (2) in the heart — chronic pressure overload → LV hypertrophy, diastolic dysfunction, eventual systolic failure; hypertension accelerates coronary atherosclerosis → ischaemic heart disease; (3) in the kidneys — high intraglomerular pressure → glomerulosclerosis → proteinuria → CKD progression (hypertensive nephrosclerosis); (4) in the eyes — retinal arteriolar changes from copper-wire appearance (Grade I) to papilloedema (Grade IV hypertensive retinopathy) correspond to severity and acuity.
The J-curve phenomenon: extremely low treated BP (<70 mmHg diastolic in coronary artery disease patients) may worsen coronary perfusion — a consideration in elderly patients with isolated systolic hypertension, though the clinical significance remains debated.
Therapeutic Goals: BP Targets and Treatment Strategy
The principal therapeutic goal in hypertension is to prevent the target-organ damage described above by maintaining blood pressure below thresholds associated with adverse outcomes. These thresholds vary by guideline and patient risk category.
Standard BP targets: Most guidelines recommend <140/90 mmHg as the general target for most adults. For high-risk patients (established CVD, DM, CKD with proteinuria), a target of <130/80 mmHg is recommended by guidelines (ACC/AHA 2017, based on SPRINT trial showing benefit of intensive control). For elderly patients (>80 years), a systolic target of 130–150 mmHg is pragmatically reasonable, with care to avoid hypotension.
Lifestyle modification is mandatory before and alongside pharmacotherapy and can reduce BP by 4–11 mmHg: sodium restriction (<5 g/day of salt; DASH diet reduces BP 8–14 mmHg); weight reduction (1 mmHg per kg weight lost); aerobic exercise (3–5 sessions/week, 30 min each); moderation of alcohol; smoking cessation (though direct BP effect is modest).
Drug initiation: Start pharmacotherapy when: BP ≥160/100 mmHg (start immediately with drugs); BP ≥140/90 with end-organ damage, established CVD, diabetes, or CKD; BP 130–139/80–89 with very-high CVD risk. In patients with BP 140–159/90–99 and low-to-moderate CV risk, a trial of 3 months of lifestyle modification before pharmacotherapy is acceptable.
Monotherapy vs combination: Monotherapy controls BP in <50% of patients (reflects the multifactorial pathophysiology). Combination therapy is necessary for most patients, particularly those with BP >20/10 mmHg above target at initiation. Preferred first-line combinations: ACEi + CCB (ACCOMPLISH trial evidence); ARB + diuretic; ACEi + diuretic. Combinations to avoid: ACEi + ARB (ONTARGET); beta-blocker + non-dihydropyridine CCB (heart block risk).
Classification of Antihypertensive Drugs
Antihypertensive drugs are classified into eight mechanistic classes, reflecting the multiple pathways that regulate blood pressure. Understanding the mechanism of each class allows you to predict ADRs, contraindications, and complementary drug combinations.
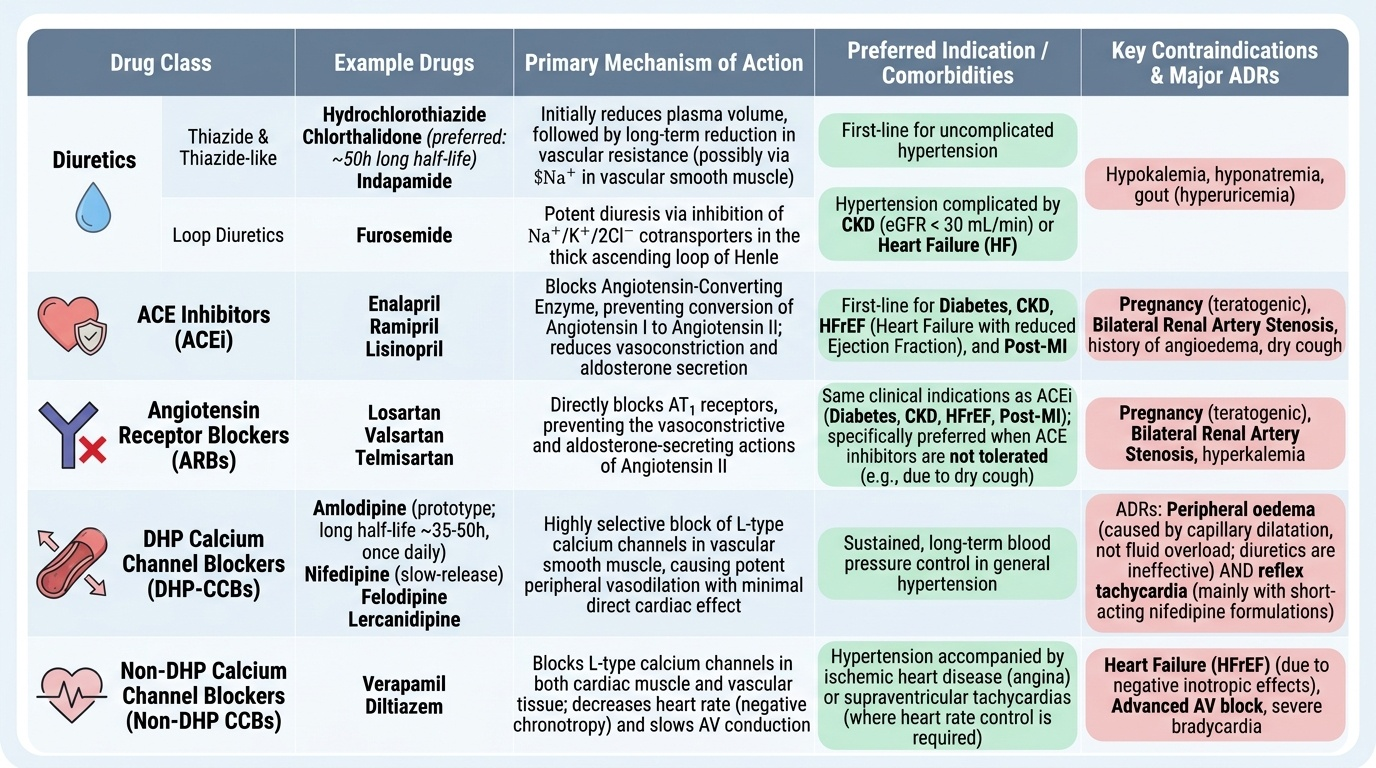
Provided image
1. Diuretics: Thiazide and thiazide-like diuretics (hydrochlorothiazide, chlorthalidone, indapamide) — first-line for uncomplicated hypertension; reduce plasma volume initially, then reduce vascular resistance by unclear mechanism (possibly reduced Na in vascular smooth muscle). Chlorthalidone is preferred over HCTZ (longer half-life ~50 vs ~10h; better ambulatory BP control; ALLHAT evidence). Loop diuretics (furosemide) — for HTN complicated by CKD (eGFR <30) or HF.
2. ACE inhibitors and 3. ARBs: As described in cvs1-raas SDL. First-line in diabetes, CKD, HFrEF, post-MI. Preferred: ACEi (enalapril, ramipril, lisinopril); ARBs when ACEi not tolerated (losartan, valsartan, telmisartan).
4. Calcium channel blockers (CCBs): Two pharmacologically distinct subclasses with very different indications:
- Dihydropyridines (DHP): amlodipine, nifedipine, felodipine, lercanidipine — primarily vascular smooth muscle selectivity; little cardiac effect. Amlodipine (once daily, long half-life ~35–50 h) is the prototype for sustained antihypertensive use. ADRs: peripheral oedema (capillary dilatation, not fluid overload — diuretic does not help), reflex tachycardia (short-acting nifedipine — use slow-release).
- Non-dihydropyridines (non-DHP): verapamil, diltiazem — block cardiac and vascular calcium channels; reduce HR (negative chronotropy), AV conduction (negative dromotropy), and contractility (negative inotropy). Used in angina and supraventricular arrhythmias, NOT in HFrEF. Contraindicated in combination with beta-blockers (risk of complete heart block and bradycardia).
5. Beta-blockers: Discussed below.
6. Central α2-agonists: Methyldopa (α2 agonist in nucleus tractus solitarius → reduces sympathetic outflow; drug of choice in pregnancy); clonidine (α2 agonist + imidazoline-1 receptor, centrally). ADRs: sedation, dry mouth, rebound hypertension on abrupt withdrawal (clonidine).
7. Direct vasodilators: Hydralazine (directly relaxes arteriolar smooth muscle — mechanism unclear, possibly via NO; reflex tachycardia + fluid retention → must be combined with BB and diuretic; lupus-like syndrome at high doses); minoxidil (K-channel opener; hypertrichosis — used topically for alopecia; reserved for resistant HTN); nitroprusside (IV only, emergency use).
8. Alpha-1 blockers: Prazosin, doxazosin — block α1-adrenergic receptors on arteriolar smooth muscle. First-dose hypotension (postural syncope — warn patients). Not first-line for HTN; useful in HTN + benign prostatic hyperplasia (reduce urethral tone).
SELF-CHECK
A 54-year-old man with hypertension, chronic stable angina, and left ventricular ejection fraction of 35% is started on antihypertensive therapy. Which drug class is MOST appropriate?
A. Verapamil (non-dihydropyridine CCB)
B. Chlorthalidone (thiazide diuretic) alone
C. Carvedilol (non-selective beta-blocker with α1 blockade)
D. Amlodipine (dihydropyridine CCB)
Reveal Answer
Answer: C. Carvedilol (non-selective beta-blocker with α1 blockade)
Carvedilol is a non-selective β-blocker with α1-blocking activity. In this patient with HFrEF (EF 35%), a beta-blocker (carvedilol, bisoprolol, or metoprolol succinate) is a cornerstone of therapy — evidence-based for mortality reduction in HFrEF (COPERNICUS for carvedilol). It also treats angina. Verapamil (non-DHP CCB) is contraindicated in HFrEF — its negative inotropic effect worsens systolic function. Chlorthalidone alone does not address the HFrEF or angina. Amlodipine is acceptable in HFrEF (PRAISE trial showed safety) but lacks the mortality benefit of beta-blockers in HFrEF.