Page 12 of 33
PH4.7 | PH4.7 | Hypertension Pharmacotherapy — SDL Guide (Part 2)
First-Line Antihypertensives: Thiazides, ACEi/ARBs, and CCBs
The three first-line antihypertensive drug classes — thiazide diuretics, ACEi/ARBs, and dihydropyridine CCBs — form the backbone of evidence-based hypertension management. Each has distinct pharmacokinetic properties, mechanisms, and indication profiles.
Thiazide and thiazide-like diuretics: The ALLHAT trial (33,357 high-risk hypertensive patients) compared chlorthalidone against amlodipine and lisinopril and found chlorthalidone non-inferior or superior for most outcomes, establishing thiazides as first-line. Chlorthalidone is preferred over hydrochlorothiazide (HCTZ) in clinical practice because of its longer half-life (~50 h vs ~10 h), once-daily dosing, and better evidence base. Indapamide has vasodilatory properties and fewer metabolic effects than HCTZ, making it useful in patients with glucose intolerance.
Thiazide ADRs relevant to antihypertensive use: hypokalaemia (supplement potassium, combine with ACEi/ARB which retain K), hyponatraemia (risk in elderly women), hyperuricaemia (may precipitate gout), hyperglycaemia (impair insulin secretion via hypokalaemia; relevant in pre-diabetes), erectile dysfunction (common but under-reported), mild dyslipidaemia (dose-dependent).
Dihydropyridine CCBs (amlodipine): Amlodipine is the most widely prescribed antihypertensive globally — once-daily dosing, no food interactions, effective across all age groups and ethnicities (particularly effective in elderly patients and in those of Black African ancestry, in whom RAAS-based drugs are less effective as monotherapy). The ACCOMPLISH trial demonstrated amlodipine + benazepril (ACEi) to be superior to HCTZ + benazepril for cardiovascular outcomes — supporting the ACEi + DHP-CCB combination as a preferred first-line choice. Key ADR: peripheral oedema (40% at high doses) — dose-related, non-inflammatory (distinguish from diuretic-responsive cardiac oedema); leg elevation helps.
ACEi and ARBs as antihypertensives: Covered pharmacologically in cvs1-raas SDL. In hypertension without compelling indications, they are equivalent first-line options. ACEi (particularly ramipril, enalapril) have slightly more outcome data; ARBs (particularly losartan, telmisartan) offer better tolerability (no cough). RAAS-based drugs are less effective in Black African patients (lower renin activity) as monotherapy — use CCB or diuretic first, or combine early.
Beta-Blockers, Central Agents, and Direct Vasodilators
Beta-adrenergic blockers lower BP primarily by reducing cardiac output (↓HR and ↓contractility via β1 blockade) and by reducing renin secretion from juxtaglomerular cells. They are no longer considered first-line monotherapy for uncomplicated hypertension (ASCOT-BPLA trial showed atenolol + bendroflumethiazide inferior to amlodipine + perindopril for CV outcomes), but they are strongly indicated as antihypertensives in the context of:
- HFrEF (carvedilol, bisoprolol, metoprolol succinate — COPERNICUS, CIBIS-II, MERIT-HF trials)
- Post-MI (reduce remodelling and arrhythmias)
- Angina pectoris (reduce myocardial oxygen demand)
- Tachyarrhythmias with hypertension
Beta-blocker subclassification:
- Cardioselectivity (β1-selectivity): atenolol, bisoprolol, metoprolol, nebivolol — relatively selective for β1 at therapeutic doses; safer in asthma (less β2 blockade) and less dyslipidaemia (less β2 blockade reduces LPL suppression). Selectivity is dose-dependent — at high doses, cardioselective agents also block β2.
- Non-selective: propranolol (β1+β2), nadolol, carvedilol (β1+β2+α1), labetalol (β1+β2+α1) — avoid in asthma/COPD; propranolol also lipophilic (penetrates CNS → nightmares, depression).
- Intrinsic sympathomimetic activity (ISA): pindolol, acebutolol — partial agonists; less resting bradycardia; less useful in post-MI.
- Nebivolol: β1-selective + stimulates NO release from endothelium (additional vasodilatory mechanism).
Beta-blocker ADRs: bradycardia, AV block, cold extremities, fatigue, impotence, hypoglycaemia masking (in insulin-dependent diabetes — mask tachycardia warning sign; hypoglycaemia sweating is preserved since it is α-mediated). Contraindications: acute decompensated HF, severe asthma/COPD, second- or third-degree AV block, sick sinus syndrome.
Central α2-agonists — methyldopa: Acts on α2-adrenergic receptors in the central nervous system (nucleus tractus solitarius and brainstem) → reduces sympathetic outflow → lower BP + HR. Drug of choice for oral antihypertensive in pregnancy (longest safety record in pregnancy; no evidence of fetal harm in multiple trials). ADRs: sedation, dry mouth, positive Coombs test (autoimmune haemolytic anaemia with chronic use), hepatitis (rare). Clonidine (α2 + imidazoline-1 agonist): causes rebound hypertension on abrupt withdrawal — must be tapered; used in hypertensive urgency and opioid withdrawal.
Direct vasodilators — hydralazine: Directly relaxes arteriolar smooth muscle (exact mechanism unclear; may involve guanylyl cyclase activation). Causes reflex tachycardia and fluid retention → always combined with a beta-blocker and diuretic. IV hydralazine is used in severe PIH. Chronic high doses (>200 mg/day) cause a drug-induced lupus-like syndrome (anti-histone antibodies, arthralgia, rash) — more common in slow acetylators. Minoxidil (K-channel opener, more potent vasodilator) causes marked hypertrichosis (hair growth — exploited in topical form for alopecia) and pericardial effusion at high doses; reserved for resistant hypertension. Sodium nitroprusside (IV only): releases NO directly → balanced arterial and venous dilation; fastest-acting antihypertensive for hypertensive emergency; requires ICU monitoring; prolonged infusion releases cyanide (metabolised to thiocyanate — toxic; monitor with serum thiocyanate if infused >48h).
SELF-CHECK
A 30-year-old woman at 32 weeks of gestation presents with BP 170/108 mmHg, headache, and 3+ proteinuria. She has no symptoms of severe hypertension (no blurred vision, no epigastric pain). Which drug is MOST appropriate for acute BP control?
A. Oral enalapril 5 mg immediately
B. IV labetalol 20 mg bolus
C. IV sodium nitroprusside
D. Oral chlorthalidone 25 mg
Reveal Answer
Answer: B. IV labetalol 20 mg bolus
This patient has severe pregnancy-induced hypertension (PIH: BP ≥160/110 mmHg in pregnancy). IV labetalol (α1+β blocker) is a first-line agent for acute hypertensive emergency in pregnancy — it is safe for mother and fetus. Enalapril (ACEi) is ABSOLUTELY CONTRAINDICATED in pregnancy — teratogenic from the first trimester, causes oligohydramnios, renal tubular dysplasia, and fetal growth restriction. Sodium nitroprusside is contraindicated in pregnancy (cyanide toxicity to fetus). Chlorthalidone is not indicated for acute treatment (oral thiazides are not appropriate for hypertensive emergency).
CLINICAL PEARL
The ACEi/ARB pregnancy trap — an absolute prohibition: ACE inhibitors and angiotensin receptor blockers are ABSOLUTELY CONTRAINDICATED in pregnancy at any trimester. In the first trimester, they may cause congenital abnormalities (cardiovascular and CNS defects). In the second and third trimesters, their effects on fetal RAAS cause oligohydramnios (leads to limb contractures, pulmonary hypoplasia, and facial anomalies — the 'ACE inhibitor fetopathy'), renal tubular dysgenesis (neonatal AKI + anuria), hypocalvaria (deficient skull ossification), and intrauterine growth restriction. Any woman of childbearing potential prescribed an ACEi or ARB must be counselled about this risk and switched to a safe alternative (methyldopa, labetalol, nifedipine, hydralazine) immediately on confirmed pregnancy. This is not a theoretical risk — real cases of neonatal death have been attributed to ACEi/ARB exposure in pregnancy.
Clinical Decision-Making: Comorbidity-Driven Prescribing
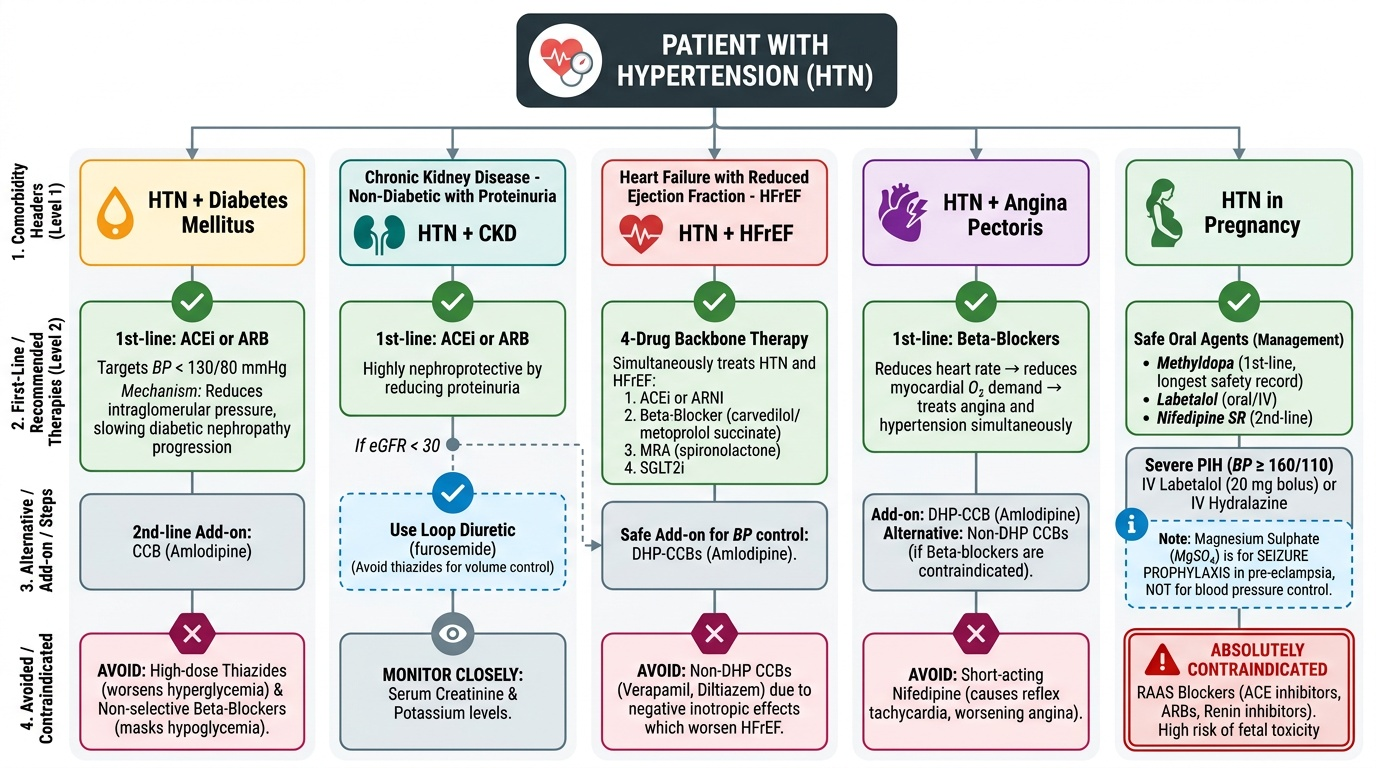
The most effective antihypertensive prescribing strategy integrates the patient's comorbidities to select drugs that simultaneously treat hypertension and the comorbid condition — achieving 'double duty' with a single agent. The following comorbidity-specific frameworks are essential.
HTN + Diabetes mellitus: ACEi or ARB is first-line — both treat hypertension AND reduce intraglomerular pressure → slow diabetic nephropathy progression (Lewis trial for ACEi in T2DM; IRMA-2, RENAAL for ARBs). Target BP <130/80 mmHg. Add CCB (amlodipine) as second agent. Avoid thiazides at high doses (worsens hyperglycaemia) and non-selective beta-blockers (mask hypoglycaemia warning).
HTN + CKD (non-diabetic with proteinuria): ACEi or ARB — nephroprotective by reducing proteinuria. If eGFR <30: loop diuretic (not thiazide) for volume control. Monitor creatinine + potassium closely.
HTN + HFrEF: Four-drug backbone (ACEi or ARNI + beta-blocker + MRA + SGLT2i) also treats hypertension. Avoid non-DHP CCBs (verapamil, diltiazem) — negative inotropy worsens HFrEF. DHP-CCBs (amlodipine) are safe in HFrEF if additional BP control needed.
HTN + Angina pectoris: Beta-blocker first-line (reduces HR → reduces myocardial O2 demand → treats angina + hypertension). Add DHP-CCB (amlodipine) if additional control needed. Avoid short-acting nifedipine (reflex tachycardia worsens angina). Non-DHP CCBs (verapamil, diltiazem) are alternatives if beta-blockers are contraindicated.
HTN in Pregnancy:
- Oral agents safe in pregnancy: methyldopa (first-line for chronic management; longest safety record), labetalol (oral or IV), nifedipine SR (second-line), hydralazine (oral or IV for acute).
- ABSOLUTELY CONTRAINDICATED in pregnancy: ACEi, ARBs, renin inhibitors (all RAAS blockers).
- For severe PIH (BP ≥160/110): IV labetalol (20 mg bolus, then infusion) or IV hydralazine (5–10 mg bolus).
- Magnesium sulphate (MgSO₄) is used for SEIZURE PROPHYLAXIS in pre-eclampsia/eclampsia — it is NOT an antihypertensive.
Hypertensive emergency (BP ≥180/120 with target-organ damage — encephalopathy, aortic dissection, acute MI, acute pulmonary oedema, eclampsia):
- Goal: reduce BP by no more than 20–25% in the first hour (prevent cerebral hypoperfusion); further reduction to 160/100 over next 2–6 hours; avoid rapid falls.
- Agents: IV labetalol (versatile — safe in most emergencies including pregnancy); IV nicardipine (DHP-CCB IV — for most hypertensive emergencies, including post-neurosurgery); IV sodium nitroprusside (most potent; needs ICU, cyanide monitoring if >48h); IV esmolol (short-acting β-blocker — aortic dissection first-choice to reduce HR + BP).
- Aortic dissection special case: esmolol (↓HR to 60 bpm) + nicardipine/nitroprusside (↓BP) — essential to blunt the aortic wall shear stress.
Hypertensive urgency (BP ≥180/120 WITHOUT target-organ damage):
- Oral agents: oral captopril (SL or oral, onset 15–30 min), oral labetalol (200 mg), oral clonidine (loading dose); outpatient setting acceptable.
- Goal: gradual BP reduction over 24–48 hours — do not lower rapidly (risk of watershed infarction).
Provided image
SELF-CHECK
A patient with hypertension and gout presents for antihypertensive initiation. Which drug is the MOST appropriate choice?
A. Hydrochlorothiazide 25 mg/day
B. Losartan 50 mg/day
C. Amlodipine 5 mg/day
D. Propranolol 40 mg twice daily
Reveal Answer
Answer: B. Losartan 50 mg/day
Losartan (ARB) has a unique uricosuric effect — its active metabolite EXP-3174 blocks urate reabsorption in the proximal tubule — making it the preferred antihypertensive in patients with gout. Hydrochlorothiazide (thiazide) causes hyperuricaemia by competing with urate for tubular secretion → worsens gout. Amlodipine is neutral for urate and would be acceptable, but losartan is preferred for its dual benefit. Propranolol (non-selective beta-blocker) causes metabolic effects (dyslipidaemia, worsens insulin resistance) and is not first-line for uncomplicated hypertension.
Self-Assessment: Antihypertensive Selection and Contraindications
Consolidate your prescribing knowledge with the following reference summaries.
Compelling indications for specific antihypertensive classes:
| Comorbidity | First-line | Avoid |
|---|---|---|
| Diabetes + nephropathy | ACEi or ARB | Thiazide high-dose, non-selective BB |
| HFrEF | ACEi/ARNI + BB (carvedilol/bisoprolol) | Non-DHP CCB (verapamil, diltiazem) |
| Post-MI | Beta-blocker + ACEi | — |
| Angina | Beta-blocker or DHP-CCB | Short-acting nifedipine |
| Isolated systolic HTN (elderly) | Thiazide or DHP-CCB | — |
| Gout | Losartan | Thiazide |
| Pregnancy (chronic) | Methyldopa, labetalol, nifedipine SR | ACEi, ARB (absolutely contraindicated) |
| Severe PIH (acute) | IV labetalol, IV hydralazine | ACEi, ARB, sodium nitroprusside (fetal cyanide) |
| BPH + HTN | Doxazosin (α1 blocker) | — |
| Asthma | DHP-CCB, ACEi, thiazide | Beta-blockers |
Hypertensive emergency vs urgency — management comparison:
| Feature | Emergency | Urgency |
|---|---|---|
| BP level | ≥180/120 mmHg | ≥180/120 mmHg |
| Target-organ damage | YES (encephalopathy, MI, pulmonary oedema, aortic dissection) | NO |
| Route | IV (hospital) | Oral (monitored setting) |
| BP reduction rate | 20–25% in 1st hour, then gradual | Gradual over 24–48h |
| Agents | IV labetalol, IV nicardipine, IV nitroprusside, IV esmolol | Oral captopril, oral labetalol, oral clonidine |