Page 14 of 33
PH4.8 | PH4.8 | Ischemic Heart Disease Pharmacotherapy — SDL Guide
Learning Objectives
- Classify drugs used for ischaemic heart disease and peripheral vascular disease by mechanism and describe their pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse effects.
- Explain the pharmacological management of chronic stable angina, acute coronary syndrome (STEMI and NSTEMI), and peripheral arterial disease.
- Devise a pharmacological management plan for a patient with acute STEMI including reperfusion strategy and long-term secondary prevention.
- Identify contraindications to fibrinolytic therapy and distinguish the major antithrombotic agents used in ACS.
INSTRUCTIONS
Ischaemic heart disease kills more people globally than any other single condition. As a junior doctor you will face two types of situations: the chronic patient with stable angina — where your goal is to relieve symptoms and prevent events — and the acute STEMI patient arriving in the emergency department where minutes to reperfusion determine whether viable myocardium survives. This SDL covers the pharmacology of anti-anginal drugs, acute coronary syndrome agents, and the long-term secondary prevention framework that reduces the risk of recurrent events.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 37 (Antianginal & Vasodilator Drugs), Ch. 34 (Antithrombotic Drugs) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th ed., Ch. 30 (Blood Coagulation), Ch. 27 (Treatment of Myocardial Ischaemia) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old male truck driver is brought to the emergency department with central crushing chest pain radiating to the left arm, onset 90 minutes ago, diaphoretic and pale. ECG shows 4-mm ST elevation in leads II, III, aVF and reciprocal ST depression in leads I and aVL (inferior STEMI). BP is 100/60 mmHg, HR 54 bpm. Primary PCI is not available — the nearest cath lab is 3 hours away. You have 10 minutes to initiate definitive pharmacological treatment. Which drugs do you give, in what order, and which fibrinolytic is you first choice? His previous cardiologist had given him streptokinase 2 years ago for a prior MI — does this change your choice?
WHY THIS MATTERS
Ischaemic heart disease causes approximately 9 million deaths per year globally — more than any other single condition. The pharmacological tools to manage it span the entire spectrum of drug classes: nitrates for symptom relief, antiplatelets to prevent thrombosis, anticoagulants to limit clot propagation, fibrinolytics to dissolve coronary thrombus, beta-blockers for remodelling prevention, and statins for atherosclerosis stabilisation. No other area of pharmacology requires the rapid, time-critical synthesis of multiple drug decisions simultaneously. The anti-anginal and ACS pharmacology you master in this SDL will save lives — literally — from the first week of your clinical career.
RECALL
Recall from physiology (PY) and previous pharmacology SDLs:
- Myocardial oxygen demand is determined by: heart rate (major determinant — the majority of coronary flow occurs in diastole; tachycardia shortens diastolic filling time), ventricular wall tension (= systolic BP × ventricular radius / 2 × wall thickness), and contractility. Drugs that reduce these factors relieve angina.
- Platelet activation cascade (PY/BI): vascular injury → collagen exposure → platelet adhesion (via GP1b-vWF) → ADP released → P2Y12 receptor activation → shape change + aggregation; thromboxane A2 (TXA2) produced by COX-1 amplifies aggregation. Aspirin blocks COX-1 → ↓TXA2; P2Y12 inhibitors block ADP-mediated amplification.
- Coagulation cascade: extrinsic (TF + VIIa) and intrinsic (XIIa cascade) pathways converge at factor X → Xa → prothrombin → thrombin → fibrinogen → fibrin. Heparin potentiates antithrombin III → inhibits thrombin (IIa) and Xa. (Detailed in cvs1-blood-coagulation SDL)
- Nitric oxide (NO) (PY/BI): synthesised from arginine; activates guanylyl cyclase → ↑cGMP → smooth muscle relaxation. Organic nitrates are NO prodrugs — they release NO in vascular smooth muscle.
Pathophysiology of IHD: Oxygen Supply-Demand Imbalance and the ACS Spectrum
Ischaemic heart disease arises when myocardial oxygen demand exceeds supply — most commonly because of atherosclerotic narrowing of one or more coronary arteries. The clinical manifestation depends on the severity and acuity of the supply-demand mismatch.
In stable angina, a fixed coronary stenosis (typically >70% luminal narrowing) limits coronary flow reserve — the ability to increase flow with demand. At rest, supply is adequate; with exertion or emotional stress, demand increases (↑HR, ↑BP, ↑contractility) and outstrips the fixed supply → transient, reversible ischaemia → chest pain that resolves with rest or nitrate. The atherosclerotic plaque is stable (fibrous cap intact).
In acute coronary syndrome (ACS), a vulnerable plaque undergoes rupture or erosion — the fibrous cap is breached, exposing the thrombogenic lipid-rich necrotic core to flowing blood. Platelets adhere to exposed collagen via GP1b-vWF, activate (release ADP, TXA2, serotonin), and aggregate to form a platelet-rich white thrombus, which is then consolidated by the coagulation cascade into a red fibrin-rich clot. If the thrombus is occlusive, STEMI results (complete occlusion → transmural infarction); if partially occlusive or fragmented (distal microemboli), NSTEMI or unstable angina results.
Pharmacological intervention targets multiple steps in this cascade: antiplatelets prevent initial platelet aggregation and propagation; anticoagulants prevent fibrin formation; fibrinolytics dissolve formed clot (STEMI only); and anti-anginal drugs reduce the oxygen demand imbalance.
Peripheral vascular disease (PVD) — also mandated by PH4.8 — shares the same atherosclerotic mechanism but in the limb arteries. Claudication (exertional calf pain) results from fixed arterial stenoses limiting limb perfusion; critical limb ischaemia represents severe, rest-pain disease. Pharmacological management: antiplatelet therapy (aspirin, clopidogrel), statin therapy, and cilostazol for claudication.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
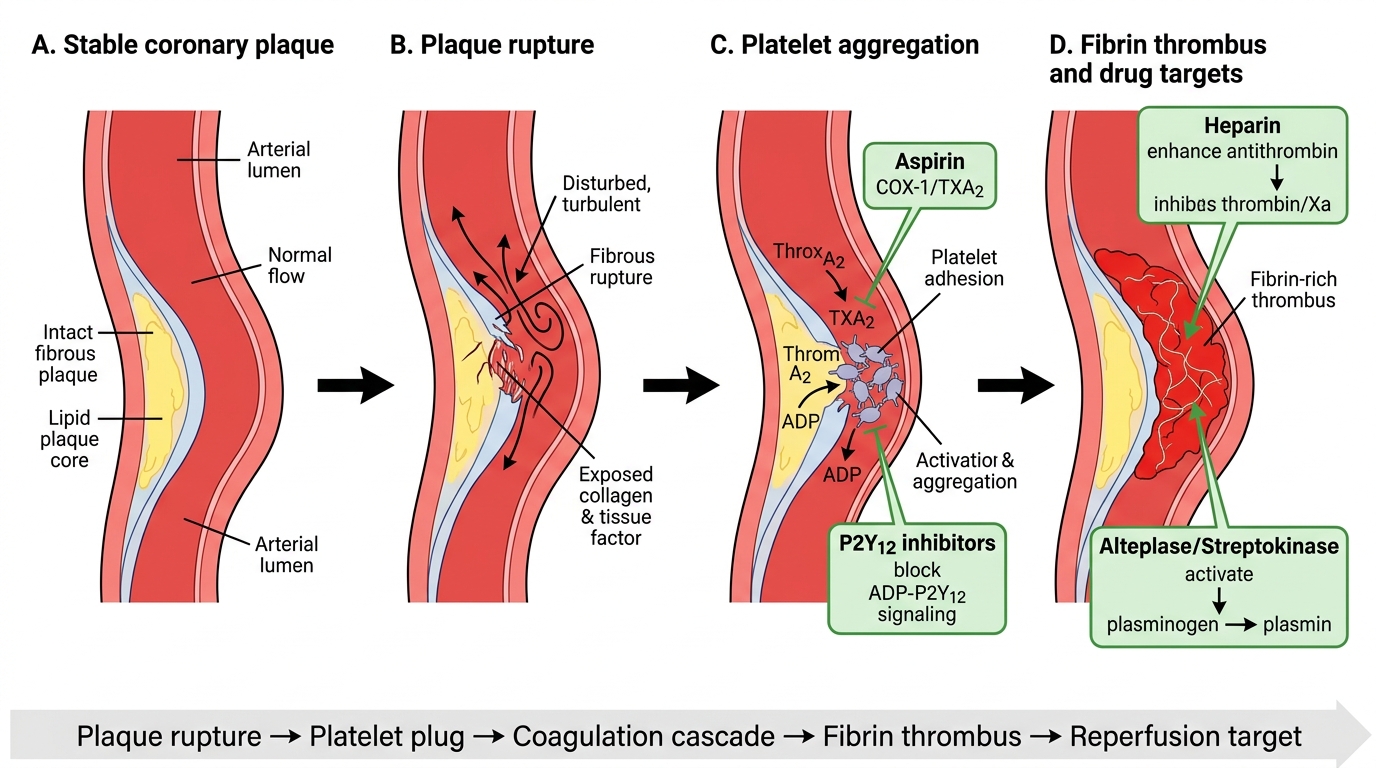
Coronary Plaque Rupture, Thrombosis, and Antithrombotic Drug Targets
Therapeutic Goals in IHD: Symptom Relief and Event Prevention
The pharmacological management of IHD pursues two distinct but complementary goals that must not be confused: symptomatic relief (reducing anginal frequency and severity) and event prevention (reducing the risk of MI, stroke, and cardiovascular death — the MACE endpoints).
Symptomatic relief drugs (reduce ischaemia): nitrates (venodilators → ↓preload; vasodilators → ↓afterload), beta-blockers (↓HR → more diastolic perfusion time; ↓O2 demand), CCBs (↓afterload; non-DHP also ↓HR). These drugs do NOT prolong survival in stable angina. They improve quality of life.
Event prevention drugs (reduce MACE, prolong life): antiplatelets (aspirin + P2Y12 inhibitors), anticoagulants (in ACS and for post-ACS bridging), high-intensity statins (plaque stabilisation + LDL lowering), ACEi/ARBs (post-MI remodelling prevention, afterload reduction in HFrEF), beta-blockers (post-MI survival benefit). These drugs do NOT necessarily relieve acute symptoms but are obligatory for secondary prevention.
In practice, the prescribing plan for any IHD patient addresses both pillars simultaneously. A patient presenting with STEMI receives: (1) antiplatelets + anticoagulant + reperfusion (fibrinolysis or PCI) for the acute event, and (2) statin + ACEi + beta-blocker + DAPT for long-term secondary prevention.
Stable angina management hierarchy: lifestyle modification → sublingual GTN for acute attacks (on-demand) → beta-blocker ± long-acting nitrate or DHP-CCB (first-line prophylaxis) → combination of beta-blocker + CCB → add ranolazine (second-line) → revascularisation assessment if pharmacologically refractory.
Classification of IHD Drugs
The pharmacological armamentarium for IHD is most usefully organised into three clinical categories, each addressing a distinct aspect of the disease.
Category A — Anti-Anginal Drugs (chronic stable angina):
1. Organic nitrates: GTN (sublingual for acute attacks; transdermal/oral for prophylaxis); isosorbide dinitrate (ISDN); isosorbide mononitrate (ISMN — active metabolite of ISDN, preferred for predictable bioavailability).
2. Beta-blockers: atenolol, metoprolol, bisoprolol — reduce HR and contractility → ↓O2 demand; first-line for effort angina.
3. Calcium channel blockers: amlodipine (DHP) for add-on; verapamil or diltiazem (non-DHP) when beta-blockers contraindicated.
4. Ranolazine: late Na-channel inhibitor → reduces Na-overload → reduces Ca-overload (via Na-Ca exchanger) → reduces diastolic tension; reduces anginal frequency without affecting HR or BP; used as add-on.
Category B — Acute Coronary Syndrome drugs:
1. Antiplatelets: aspirin (irreversible COX-1 inhibitor); P2Y12 inhibitors: clopidogrel (thienopyridine prodrug, CYP2C19-dependent), ticagrelor (reversible, not a prodrug), prasugrel (prodrug, faster).
2. Anticoagulants: unfractionated heparin (UFH), low-molecular-weight heparin — enoxaparin (subcutaneous, predictable), fondaparinux (selective factor Xa inhibitor), bivalirudin (direct thrombin inhibitor).
3. Fibrinolytics (STEMI only): streptokinase (bacterial protein, non-fibrin-specific, 1.5 MIU IV over 60 min, one-time use only due to antibodies); alteplase (recombinant tPA, fibrin-specific, IV bolus + infusion), tenecteplase (IV bolus, weight-based, fibrin-specific).
Category C — Secondary Prevention:
High-intensity statin + aspirin + P2Y12 inhibitor (DAPT 12 months post-ACS) + ACEi or ARB + beta-blocker (if LVEF reduced or HF) + PPI (gastroprotection during DAPT).
Category D — Peripheral Vascular Disease:
Cilostazol (PDE3 inhibitor → cAMP → platelet inhibition + vasodilation → improves claudication symptoms); aspirin or clopidogrel (antiplatelet); high-intensity statin; risk-factor control.
SELF-CHECK
A patient with stable angina is on atenolol 50 mg/day but continues to have exertional chest pain. Which additional drug is most appropriate?
A. Verapamil 120 mg twice daily
B. Amlodipine 5 mg once daily
C. Sublingual GTN on demand only
D. Isosorbide mononitrate (ISMN) 60 mg once daily
Reveal Answer
Answer: B. Amlodipine 5 mg once daily
When a beta-blocker alone does not control stable angina, the preferred add-on is a long-acting dihydropyridine CCB (amlodipine). The combination of beta-blocker + DHP-CCB is additive (both reduce O2 demand — beta-blocker via ↓HR; amlodipine via ↓afterload). Verapamil (non-DHP) combined with a beta-blocker is dangerous — both drugs slow AV conduction and reduce HR, increasing risk of complete heart block and severe bradycardia. Sublingual GTN is for acute attack relief, not prophylaxis. ISMN is a valid option but is second-line add-on after CCB, and nitrate tolerance requires a nitrate-free interval.