Page 15 of 33
PH4.8 | PH4.8 | Ischemic Heart Disease Pharmacotherapy — SDL Guide (Part 2)
Anti-Anginal Drugs: Nitrates, Beta-Blockers, and CCBs
Organic nitrates are the oldest anti-anginal drugs and remain irreplaceable for acute anginal relief. They undergo bioactivation (via mitochondrial aldehyde dehydrogenase, ALDH2) to release nitric oxide (NO) in vascular smooth muscle, which activates guanylyl cyclase → ↑cGMP → smooth muscle relaxation → vasodilation. At standard doses, nitrates predominantly cause venodilation (↓preload → ↓ventricular end-diastolic pressure → ↓wall tension → ↓O2 demand). At higher doses, coronary and arteriolar dilation also occurs. Effects on angina: reduced cardiac work (preload reduction) + coronary vasodilation at stenotic sites.
Pharmacokinetics of GTN: sublingual tablets or spray — rapid absorption across oral mucosa; onset 2–5 minutes, duration 20–30 minutes. Extensive hepatic first-pass metabolism (>95%) makes oral GTN impractical; sublingual bypass avoids first-pass effect. Transdermal GTN patches provide prolonged plasma levels but require a nitrate-free interval of 8–12 hours daily to prevent tolerance.
Nitrate tolerance is the attenuation of vasodilatory effects with continuous exposure, occurring within 24 hours of sustained-release or transdermal therapy. Mechanism: decreased bioactivation (oxidised ALDH2), superoxide production, and neurohormonal counter-regulation. Prevention: use intermittent dosing — apply transdermal patch for 12 hours (on/off schedule), take ISMN with an eccentric schedule (e.g., 8 AM + 2 PM — not at bedtime, leaving an 8–10h nitrate-free interval overnight).
Beta-blockers are the cornerstone of stable angina prophylaxis. By blocking β1 receptors, they reduce: (1) resting and exercise heart rate → prolonged diastolic filling time → more coronary perfusion time; (2) myocardial contractility → reduced O2 demand. The result is a higher exercise threshold before angina develops. They are the only anti-anginal drugs with proven mortality benefit post-MI (reduce remodelling and arrhythmias). Note: in COMMIT-CCS-2, routine early IV beta-blocker given to all acute STEMI patients caused increased cardiogenic shock in haemodynamically unstable patients — IV beta-blockers in acute STEMI should be reserved for haemodynamically stable patients with tachycardia or hypertension, not routinely.
Calcium channel blockers in stable angina: DHP-CCBs (amlodipine, felodipine) reduce afterload (↓systolic BP → ↓wall tension) without significantly affecting HR — useful as add-on to beta-blocker. Non-DHP CCBs (verapamil, diltiazem) also reduce HR (negative chronotropy) — appropriate as monotherapy when beta-blockers are contraindicated (asthma, severe bradycardia). Never combine non-DHP CCB + beta-blocker (severe bradycardia, AV block).
ACS Pharmacotherapy: Antiplatelets, Anticoagulants, and Fibrinolytics
Acute coronary syndrome pharmacotherapy is time-critical — every minute of myocardial ischaemia is irreversible muscle loss. The pharmacological strategy addresses the platelet-thrombus-fibrin cascade at multiple points simultaneously.
Aspirin (acetylsalicylic acid): Irreversibly inhibits COX-1 in platelets (and COX-2 at higher doses — anti-inflammatory, antipyretic). In platelets (anucleate — cannot synthesise new COX): irreversible blockade of TXA2 synthesis for the platelet's lifetime (~7–10 days). Loading dose for ACS: 300 mg immediately (chewed for rapid buccal absorption); maintenance 75–100 mg/day. The ISIS-2 trial demonstrated aspirin reduces STEMI mortality by ~25% — one of the most important findings in cardiovascular pharmacology.
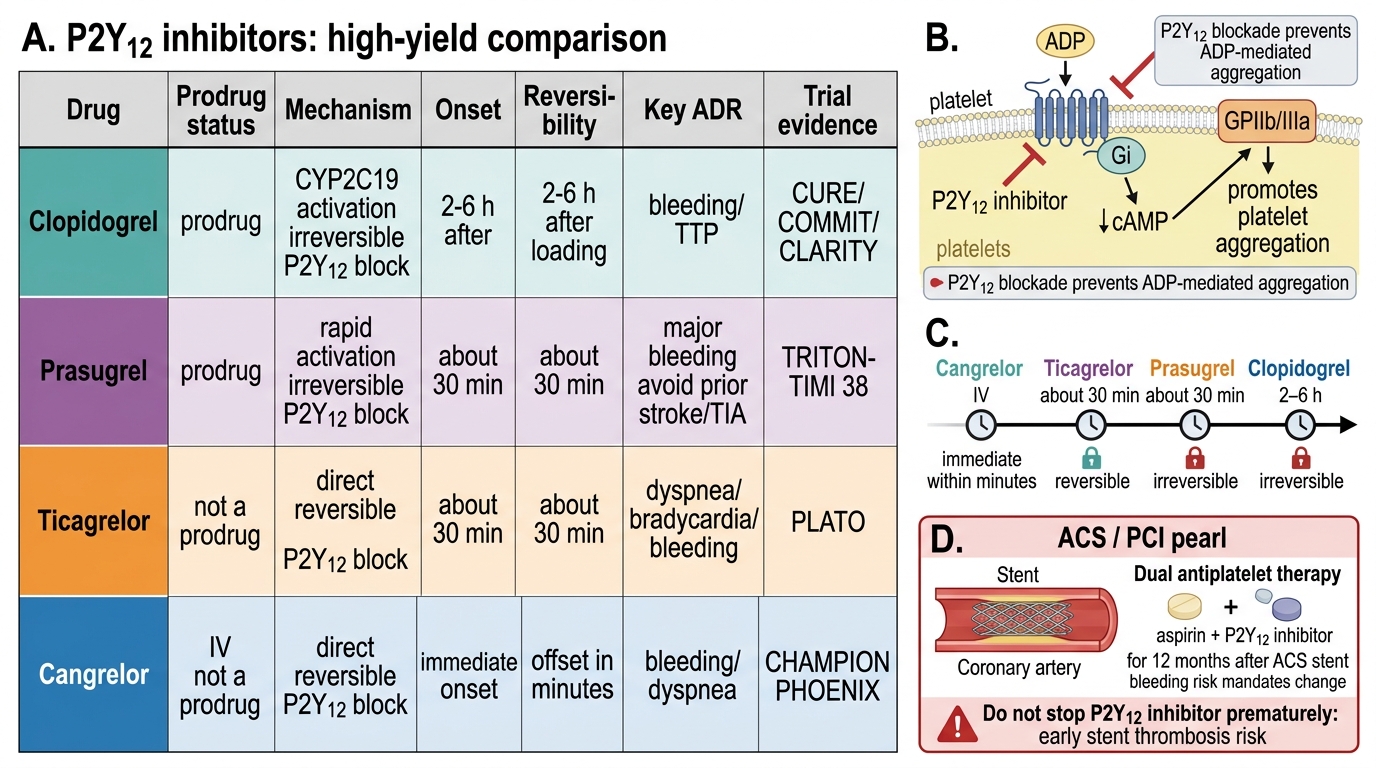
P2Y12 inhibitors: Block the ADP receptor P2Y12 on platelets, preventing ADP-mediated platelet amplification and GP IIb/IIIa activation. Three agents with important pharmacological distinctions:
- Clopidogrel: thienopyridine prodrug — requires hepatic conversion by CYP2C19 to active thiol metabolite. Irreversible P2Y12 blockade; platelets recover over ~5–7 days after stopping. Loss-of-function CYP2C19 polymorphisms (10–15% of patients; more common in Asian populations) reduce active metabolite formation → clopidogrel resistance → inadequate platelet inhibition. Loading dose 300–600 mg, maintenance 75 mg/day. Older agent, widely used due to low cost.
- Ticagrelor: cyclopentyl-triazolopyrimidine, NOT a thienopyridine, NOT a prodrug — active as ingested. Reversible P2Y12 antagonist. More rapid and consistent inhibition than clopidogrel; does not require CYP2C19 metabolism — no resistance phenotype. The PLATO trial (18,000+ ACS patients) showed ticagrelor reduces the composite of CV death + MI + stroke vs clopidogrel (9.8% vs 11.7%) with similar major bleeding but more dyspnoea (mechanism: adenosine accumulation — ticagrelor also blocks adenosine re-uptake). Loading 180 mg, maintenance 90 mg BD. Preferred over clopidogrel for ACS by most current guidelines.
- Prasugrel: thienopyridine prodrug; faster and more potent activation than clopidogrel (single CYP3A4/CYP2C19 step vs clopidogrel's two-step pathway). Irreversible inhibition. TRITON-TIMI 38 showed prasugrel superior to clopidogrel in ACS with PCI for MACE, but with significantly more major bleeding. Absolute contraindications: prior stroke/TIA (unacceptable net benefit due to intracranial bleeding), age >75 years, body weight <60 kg (these groups had excess bleeding without ischaemic benefit). Generally reserved for ACS patients undergoing PCI who do not have these contraindications.
Anticoagulants in ACS: Used to prevent thrombus extension while the platelet thrombus is stabilised by antiplatelets. Options:
- Unfractionated heparin (UFH): IV infusion; potentiates antithrombin III → inhibits thrombin (IIa) + Xa + IXa; dose monitored by aPTT. Standard in STEMI if fibrinolysis is used.
- Enoxaparin (LMWH): SC once or twice daily; primarily inhibits Xa (anti-Xa:anti-IIa ratio ~3:1 for enoxaparin); no aPTT monitoring needed (predictable pharmacokinetics); superior to UFH in NSTEMI/UA (ESSENCE trial). Dose-reduce in CKD (eGFR <30); avoid in severe CKD.
- Fondaparinux: synthetic selective factor Xa inhibitor (pentasaccharide); SC daily; renal excretion; contraindicated if eGFR <20. OASIS-5 trial showed non-inferior to enoxaparin in NSTEMI with less major bleeding. NEVER use as sole anticoagulant if PCI is performed (risk of catheter thrombosis — give UFH bolus at the time of PCI).
Fibrinolytics (thrombolytic therapy — STEMI only): Activate plasminogen → plasmin → clot lysis. ONLY indicated for STEMI when primary PCI is not available within 120 minutes of first medical contact and when contraindications are absent. Give within 12 hours of symptom onset; most benefit within 3 hours.
- Streptokinase: non-fibrin-specific (activates plasminogen in solution and on clot indiscriminately); 1.5 million IU IV over 60 min; allergic reactions possible (bacterial protein); forms neutralising antibodies — cannot be used more than once (no re-use within at least 5 years, and many guidelines say never). Cheapest fibrinolytic; widely available in developing countries.
- Alteplase (tPA): recombinant tissue plasminogen activator; fibrin-specific (binds to fibrin → activates fibrin-bound plasminogen preferentially); IV accelerated infusion; used when streptokinase allergic or when prior streptokinase has been given. Tenecteplase (TNK-tPA) is a single IV bolus, weight-based — simplest administration.
Fibrinolytic contraindications (absolute): prior intracranial haemorrhage, ischaemic stroke <3 months, known structural intracranial lesion (AVM/neoplasm), active major bleeding (not menses), suspected aortic dissection, significant closed-head trauma <3 months. Relative contraindications: uncontrolled hypertension (SBP >180 mmHg), current anticoagulation, traumatic CPR, recent major surgery (<3 weeks), pregnancy.
P2Y12 Inhibitors: Comparison and Clinical Use
SELF-CHECK
A 61-year-old man presents with anterior STEMI. He received streptokinase during a previous MI 3 years ago. Primary PCI is unavailable. The most appropriate fibrinolytic agent now is:
A. Repeat streptokinase 1.5 MIU infusion
B. Alteplase (tPA) IV accelerated regimen
C. Heparin infusion alone (no fibrinolytic)
D. Aspirin loading + ticagrelor (antiplatelet therapy only)
Reveal Answer
Answer: B. Alteplase (tPA) IV accelerated regimen
Streptokinase is a bacterial protein that elicits antibody formation after its first use. Repeat administration within 5 years (and by many recommendations ever) is contraindicated — the pre-formed antibodies neutralise its thrombolytic activity and may cause severe allergic reactions including anaphylaxis. Alteplase (recombinant tPA) is fibrin-specific and does not elicit neutralising antibodies — it is the appropriate fibrinolytic when prior streptokinase has been given. Heparin alone without a fibrinolytic is insufficient for reperfusion in STEMI when PCI is unavailable. Antiplatelets alone do not lyse the occlusive coronary thrombus.
CLINICAL PEARL
DAPT duration and bleeding risk — the balance: After ACS with stent placement, dual antiplatelet therapy (aspirin + ticagrelor or clopidogrel) for 12 months is standard. The P2Y12 inhibitor should NOT be stopped prematurely — stent thrombosis risk is highest in the first 3–6 months. If a patient requires elective surgery during this period: consult with cardiology and haematology before stopping antiplatelet. If a patient develops major bleeding on DAPT: identify the source, control it, and make a shared decision about whether the antiplatelet can be restarted. Never stop both agents simultaneously if avoidable — aspirin alone is acceptable in most scenarios when P2Y12 must be stopped temporarily. Always add a PPI (pantoprazole, omeprazole) when prescribing DAPT to reduce GI bleeding risk.
Clinical Decision-Making: ACS and Peripheral Vascular Disease
Effective IHD pharmacotherapy integrates the acute treatment plan with a long-term secondary prevention strategy, tailored to the patient's clinical syndrome, comorbidities, and reperfusion strategy.
Acute STEMI management plan (mnemonic MONABASH):
- Morphine (IV) — for pain if not relieved by nitrates; may reduce sympathetic activation
- Oxygen — only if SpO2 <94% (hyperoxia may increase infarct size)
- Nitrates — sublingual GTN for immediate pain relief; avoid if SBP <90 mmHg (RV infarction) or if patient took a PDE5 inhibitor (sildenafil/tadalafil) in last 24–48h (dangerous hypotension)
- Aspirin 300 mg loading dose (chewed)
- Beta-blocker (oral, haemodynamically stable patients only) — rate control, prevents arrhythmias; avoid if cardiogenic shock, severe bradycardia, or acute HF signs
- Anticoagulant (UFH or enoxaparin)
- Statin (high-intensity: atorvastatin 80 mg) — plaque stabilisation; start within 24h
- Heparin continuation + P2Y12 inhibitor (ticagrelor preferred)
Then → reperfusion decision:
- Primary PCI if available within 90 min door-to-balloon (or 120 min from first medical contact) — gold standard.
- Pharmacological fibrinolysis if PCI unavailable within 120 min — give within 12h of symptoms, greatest benefit within 3h.
NSTEMI/UA management: No fibrinolytics (thrombus is non-occlusive; fibrinolytics may worsen outcomes). Give: aspirin + P2Y12 inhibitor (ticagrelor preferred; clopidogrel if ticagrelor not available) + anticoagulant (enoxaparin or fondaparinux preferred) + beta-blocker + statin + ACEi (if LVEF reduced). Angiography + PCI within 24–48h for high-risk features (elevated troponin, ST changes, haemodynamic instability).
Long-term secondary prevention post-ACS:
- DAPT (aspirin 75 mg + P2Y12 inhibitor): 12 months; consider extending to 24 months in high-thrombosis-risk, low-bleeding-risk patients (PEGASUS trial)
- High-intensity statin (atorvastatin 40–80 mg) indefinitely
- ACEi or ARNI + beta-blocker if LVEF <40% (evidence from multiple trials)
- PPI (pantoprazole 40 mg) while on DAPT
- Eplerenone if LVEF <40% + HF symptoms or diabetes post-MI (EPHESUS trial)
Peripheral vascular disease (PVD) pharmacotherapy (mandated by PH4.8):
- Cilostazol (phosphodiesterase-3 inhibitor → ↑cAMP in platelets and vascular smooth muscle → platelet inhibition + vasodilation) — reduces claudication distance in peripheral arterial disease; contraindicated in HF (PDE3 inhibitors are harmful in HF — milrinone trial precedent).
- Antiplatelet therapy: clopidogrel preferred over aspirin in PVD (CAPRIE trial: clopidogrel superior in symptomatic PVD); both are used.
- Statin — mandatory for all PVD patients (reduces cardiovascular events, slows plaque progression).
- Structured exercise therapy is the most effective intervention for claudication — pharmacotherapy is adjunctive.
SELF-CHECK
Which statement about ticagrelor is CORRECT?
A. Ticagrelor is a prodrug that requires CYP2C19 activation to exert its effect
B. Ticagrelor causes irreversible P2Y12 receptor blockade
C. Ticagrelor does not require CYP2C19 activation and causes reversible P2Y12 blockade
D. Ticagrelor is contraindicated in patients with prior stroke or TIA
Reveal Answer
Answer: C. Ticagrelor does not require CYP2C19 activation and causes reversible P2Y12 blockade
Ticagrelor is chemically distinct from clopidogrel and prasugrel (it is not a thienopyridine). It is NOT a prodrug — it is pharmacologically active as administered, without requiring CYP2C19 conversion. Its P2Y12 receptor blockade is REVERSIBLE (compared to the irreversible binding of clopidogrel's active metabolite and prasugrel's active metabolite). This reversibility means platelet function returns 3–5 days after stopping, vs 5–7 days for clopidogrel. Option A (prodrug + CYP2C19) describes clopidogrel; option B (irreversible) also applies to clopidogrel/prasugrel; option D (contraindicated in prior stroke/TIA) describes prasugrel, not ticagrelor — ticagrelor can be used cautiously in prior stroke patients.
Self-Assessment: IHD Pharmacology Decision Framework
Use these reference summaries to consolidate your understanding before the assessment.
P2Y12 inhibitor comparison:
| Feature | Clopidogrel | Ticagrelor | Prasugrel |
|---|---|---|---|
| Prodrug | Yes (CYP2C19) | No | Yes (CYP3A4/2C19) |
| Onset | Slow (2–6h) | Faster (~2h) | Fastest (<1h) |
| Reversibility | Irreversible | Reversible | Irreversible |
| PLATO/TRITON advantage | Reference | Superior PLATO | Superior TRITON-TIMI 38 |
| Prior stroke/TIA | Safe | Safe | CONTRAINDICATED |
| Age >75 or wt <60kg | Caution | Caution | CONTRAINDICATED |
Fibrinolytic absolute contraindications (memorise all):
1. Prior intracranial haemorrhage (at any time)
2. Ischaemic stroke <3 months
3. Known intracranial structural lesion (AVM, neoplasm)
4. Active significant bleeding (excluding menses)
5. Suspected aortic dissection
6. Significant head trauma <3 months
Nitrate interactions to remember:
- GTN + PDE5 inhibitors (sildenafil, tadalafil, vardenafil) → severe hypotension (cGMP accumulation from both pathways). Contraindicated within 24h of sildenafil/vardenafil or 48h of tadalafil.
- Tolerance prevented by nitrate-free interval (8–12h daily).